
Abstract
Background
Anaemia during pregnancy causes adverse outcomes to the woman and the foetus, including anaemic heart failure, prematurity, and intrauterine growth restriction. Iron deficiency anaemia (IDA) is the leading cause of anaemia and oral iron supplementation during pregnancy is widely recommended. However, little focus is directed to dietary intake. This study estimates the contribution of IDA among pregnant women and examines its risk factors (including dietary) in those with moderate or severe IDA in Lagos and Kano states, Nigeria.
Methods
In this cross-sectional study, 11,582 women were screened for anaemia at 20-32 weeks gestation. The 872 who had moderate or severe anaemia (haemoglobin concentration < 10 g/dL) were included in this study. Iron deficiency was defined as serum ferritin level < 30 ng/mL. We described the sociodemographic and obstetric characteristics of the sample and their self-report of consumption of common food items. We conducted bivariate and multivariable logistic regression analysis to identify risk factors associated with IDA.
Results
Iron deficiency was observed among 41% (95%CI: 38 – 45) of women with moderate or severe anaemia and the prevalence increased with gestational age. The odds for IDA reduces from aOR: 0.36 (95%CI: 0.13 – 0.98) among pregnant women who consume green leafy vegetables every 2-3 weeks, to 0.26 (95%CI: 0.09 – 0.73) among daily consumers, compared to those who do not eat it.
Daily consumption of edible kaolin clay was associated with increased odds of having IDA compared to non-consumption, aOR 9.13 (95%CI: 3.27 – 25.48). Consumption of soybeans three to four times a week was associated with higher odds of IDA compared to non-consumption, aOR: 1.78 (95%CI: 1.12 – 2.82).
Conclusion
About 4 in 10 women with moderate or severe anaemia during pregnancy had IDA. Our study provides evidence for the protective effect of green leafy vegetables against IDA while self-reported consumption of edible kaolin clay and soybeans appeared to increase the odds of having IDA during pregnancy. Health education on diet during pregnancy needs to be strengthened since this could potentially increase awareness and change behaviours that could reduce IDA among pregnant women with moderate or severe anaemia in Nigeria and other countries.
Similar content being viewed by others


Introduction
Anaemia in pregnancy is a major public health challenge which caused 50 million disability-adjusted life years (DALYs) worldwide in 2019 [1]. Globally, it affected 500 million women of reproductive age 15 – 49 years in the same year; and of these, 32 million were pregnant women [1]. Anaemia is among the leading causes of maternal and perinatal morbidity and mortality globally [2, 3]. The burden of the condition is greater in low- and middle-income countries compared to high-income countries. The variation in anaemia prevalence by region is partly a reflection of the global inequalities in nutrition, literacy level and access to health care; all of which are poorer in low-middle-income countries [4,5,6].
The regions with the highest burden of anaemia in pregnancy are South-East Asia and sub-Saharan Africa, where it affects 244 million and 106 million women of reproductive age, respectively [1]. These two regions are the most populous in the world with a population of 4.8 billion in Asia and 1.5 billion in Africa, each contributing 59% and 18% respectively to the world’s population [7]. The high prevalence of anaemia in these regions is likely because many people are in the poorest wealth quintiles, with low level of educational attainment, and high burden of malnutrition in form of micronutrient deficiencies like iron, folate, zinc, and vitamin B12 deficiencies [8,9,10,11].
Anaemic pregnant women have higher odds for maternal complications like anaemic heart failure, preterm delivery, and postpartum haemorrhage; and a 3.5 times increased risk of death in those with severe anaemia [2, 12]. It is associated with a higher incidence of adverse perinatal outcomes like foetal growth restriction, foetal demise, babies with birth asphyxia, and neonatal death; 62% in anaemic compared to 28% in non-anaemic pregnant women [3, 13].
Serum ferritin is widely used in research and clinical settings for screening for IDA [14]. However, universal screening during pregnancy might be challenging in low-middle-income countries due to inadequate laboratory facility, low staff strength, high antenatal patient load, and poverty. Treatment for IDA in pregnancy includes oral and parenteral iron supplementation. Prevention and treatment also include dietary modifications to improve both the intake and the bioavailability of dietary iron [15, 16]. Poor compliance with oral iron treatment is a problem and is often because of suboptimal adherence associated with multiple dosing, side effects which are mostly gastrointestinal in nature, or poverty [17, 18]. Dietary factors such as inadequate intake of meat and green vegetables significantly increase the odds of having anaemia during pregnancy [19].
[20,21,22,23,24]. In Nigeria, the prevalence of anaemia among women of reproductive age 15 – 49 (defined as finger prick haemoglobin concentration less than 11 g/dL) was 58% based on the most recent nationally representative Nigeria Demographic and Health Survey (NDHS) 2018 [25]. The survey found prevalence of anaemia in pregnancy to be 50% in Lagos state and 47% in Kano state, Nigeria [25].
In particular, iron deficiency was reported in 25 – 46% of pregnant women with anaemia in Nigeria [26]. Iron is a vital component of haematopoiesis [27]. In a recent systematic review from Nigeria, multiparity, being in the third trimester of pregnancy, and low socioeconomic status were identified as risk factors for iron deficiency anaemia (IDA) among pregnant women [26]. In most health facilities in Nigeria routine screening for anaemia in pregnancy is determined by haematocrit, whereas specific screening for IDA is uncommon. As many as 17% of Nigerian women who registered for ANC do not receive iron supplementation; and of those who do, 17% will not take the iron supplements while 91% of those who will take the iron supplements have poor adherence with the dosage [28].
There is a paucity of studies assessing prevalence and risk factors for IDA in pregnancy in Nigeria; and none exploring dietary risk factors [26]. The only Nigerian study, found in the literature, on dietary intake and IDA, considered IDA to be same as anaemia in pregnancy and defined IDA as haemoglobin concentration < 11 g/dl [29]. Understanding the factors associated with IDA may help improve counselling of pregnant women, especially with respect to diet which is a modifiable factor.
This study focused on pregnant women with moderate or severe anaemia as this group of pregnant women will often need further evaluation and treatment because of their higher risk of suffering negative consequences during pregnancy [30]. It estimated the contribution of IDA among pregnant women and examined its risk factors (including dietary) in those with moderate or severe IDA in Lagos and Kano states, Nigeria.
Methods
Study setting
This cross-sectional study was conducted at 11 publicly owned health facilities (five at primary, four at secondary, and two at tertiary) in Lagos and Kano states, Nigeria, as part of the IVON trial [31]. The IVON trial was pre-registered in ClinicalTrials.gov on 26/07/2021, with Identifier No. NCT04976179. It is a randomized clinical trial evaluating the effectiveness and safety of intravenous iron versus oral ferrous sulphate for treatment of iron deficiency anaemia during pregnancy. The two most populous states in Nigeria, Lagos and Kano [32] were purposively selected for the trial to capture differentials in provision of health care like disparity in health systems processes, distribution of healthcare workers’ numbers, cadre and skills, and patient characteristics.
Participants
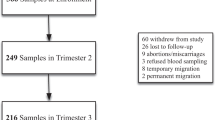
Participants included in this study were 872 pregnant women aged 15-49 years and at 20-32 weeks gestational age enrolled into the IVON trial between August 9, 2021, and October 7, 2022. A sample size of 872 participants would be more than sufficient to estimate the prevalence of iron deficiency among pregnant women with anaemia, based on a prevalence of 63.6% from previous study in a similar setting, using Cochran’s formula and adjusting for 20% attrition [33, 34]. Excluded from the IVON trial and this study were women with haemoglobinopathies, history of blood transfusion in the last three months, active bleeding from any part of the body, recent major surgery, autoimmune diseases, chronic kidney disease, cancer, human immunodeficiency virus infection (HIV), and clinically confirmed malabsorption syndrome. Figure 1 shows the inclusion flow chart for this study.

Flow chart showing inclusion of study participants (pregnant women at 20 – 32 weeks gestation)
A Total number of pregnant women 20-32 weeks of gestation screened for anaemia
B Number of pregnant women who are anaemic
C Number of the pregnant women who had moderate or severe anaemia
D Number of women enrolled into IVON trial
E Number of IVON participants with serum ferritin result at enrolment, included in this study
The IVON trial is a randomized controlled clinical trial evaluating the effectiveness and safety of oral ferrous sulphate versus intravenous ferric carboxymaltose for treatment of iron deficiency anaemia in pregnant Nigerian women
Data collection
As part of routine ANC, all pregnant women attending the health facilities between 20 – 32 weeks gestational age had their haemoglobin (Hb) concentration determined during screening using Hemocue Hb 301 system. Any anaemia refers to anaemia of any severity, which in pregnancy is taken to be Hb concentration < 11 g/dL [35]. Mild anaemia in pregnancy: Hb concentration from 10 to < 11 g/dL [35]. Moderate anaemia in pregnancy: Hb concentration from 7 to < 10 g/dL [35]. Severe anaemia in pregnancy: Hb concentration < 7 g/dl [35]. We used a cut off value of 30 ng/mL for serum ferritin concentration in pregnant women to define ID in this study as it was found to have a higher sensitivity of 92% and a specificity of 98%, and correlates well with bone marrow iron stores, compared to a cut off of 12 ng/mL with sensitivity of 37.5% and specificity of 93.7% [36, 37]. The UK guideline also recommends treatment of pregnant women for iron deficiency when serum ferritin concentration is < 30 ng/mL [38]. At the time of this study, there was a lack of ANC guideline on IDA in Nigeria.
Women found to have moderate or severe anaemia (haemoglobin concentration below 10 g/dL) were invited into the IVON trial following informed consent. An interview was conducted with the consenting woman by a trained research nurse using an online questionnaire on Research Electronic Data Capture (REDCap) hosted by Queen Mary University of London [39]. Data in both the screening and enrolment databases were analysed for this study. Data collected during screening included the health facility name, and self-reported information such as maternal age, gestational age from the medical records and Hb level measured at the screening. Data collected during enrolment included self-reported information such as parity, marital status, ethnicity, place of residence, level of education and occupation of participant, male partner’s occupation (if applicable), and monthly income of participant. Food frequency assessment and participant’s weight and height measurements were collected at enrolment by the research nurse. All study participants were screened for malaria at enrolment using SD BIOLINE Malaria Ag P.f rapid diagnostic test kit [40]. Those who screened positive for malaria were treated with an artemisinin-based combination therapy and offered intermittent preventive therapy (IPT) subsequently to minimize the risk of recurrence, while those who screened negative for malaria were initiated on IPT if not already initiated.
Main outcome
The binary outcome variable: IDA was defined as serum ferritin < 30 ng/mL. To measure serum ferritin, four millilitres (4 mL) of blood was collected from each participant, with Hb concentration < 10 g/dL, into serum separator tubes. The serum extracted was used for serum ferritin assay at Synlab Laboratories Limited, an internationally accredited laboratory, using ARCHITECT Ferritin assay method [41].
Independent variables
Marital status was categorized as single, cohabiting, married, or divorced. Ethnicity was categorised as Igbo, Yoruba, Hausa, and others. Place of residence was categorised as urban or rural. Highest level of education was categorised as no formal education, some primary or completed primary, completed secondary, or completed tertiary or higher. Age was categorised into three groups: 15 – 19, 20 – 34, and ≥ 35 years. Body mass index was categorised as > 18.5 kg/m2 (underweight), 18.5 – < 25 kg/m2 (normal), 25 – < 30 kg/m2 (overweight), and ≥ 30 kg/m2 (obese). Parity was categorized as 0, 1, 2 – 4, and 5 and above, based on the number of pregnancies a woman has carried to 28 weeks gestational age and above. Late second trimester was defined as gestational age between 20 – 26 weeks, and early third trimester was defined as gestational age between 27 – 32 weeks.
Household socioeconomic status (SES) is a measure of an individual or family’s access to resources and it influences health-related outcomes and exposures [42]. It was defined using the Nigerian classification system by Ibadin et al. (2021) taking into consideration the participant and her male partner’s (excluded for the unmarried) occupation and level of education, and which generates scores of 1 – 6; 1 indicating the highest grade and 6 the lowest grade [43]. All participants who had a final score of 1 – 2 were categorised as being in upper socioeconomic class, final score of 3 – 4 as middle class, and 5 – 6 as lower socioeconomic class [43].
Dietary intake was assessed using a pre-tested 17-item food frequency questionnaire (FFQ), adapted from a previous tool [44]. It was redesigned for this study and comprised locally available food items some of which have previously been reported to be iron chelators such as turmeric and tea [45, 46] and performed well on pretesting with a scale reliability coefficient of 0.71. The FFQ contained 15 food items and two types of hot beverages. For the food items, participants were asked to select the frequency of consumption presented as a Likert scale as everyday (always), 3 to 4 times a week (often), every 2 or 3 weeks (sometimes), and don’t eat (never). Edible kaolin clay was included as a food item because it is commonly consumed by pregnant black African women [47] and has previously been reported to be associated with IDA [48]. For beverages, participants selected the average number of cups ingested per day categorised into four groups: 0, 1, 2, 3 or more.
Data analysis
Prevalence of any anaemia in pregnancy was calculated as percentage of all women screened who had Hb < 11 g/dl (B/A in Fig. 1). Prevalence of IDA was estimated as the percentage of women with iron deficiency (serum ferritin < 30 ng/ml) among all women diagnosed with moderate or severe anaemia included in this study. Categorical variables are described as percentages with a 95% confidence interval (CI). Pearson’s Chi square test was used to evaluate the difference in the prevalence of IDA among the pregnant women with moderate or severe anaemia in the study sample, and to compare the distribution of categorical variables. Normality testing was conducted on continuous variables like maternal age, gestational age, haemoglobin concentration and serum ferritin concentration using Shapiro Wilks test to determine their distribution in the study population and to know the most appropriate statistical test to use for analysis. Wilcoxon rank sum test was used to describe and compare the medians of continuous variables (age and gestational age at inclusion in study). The predictive probabilities for IDA at various gestational ages was plotted by doing post estimation for predictive margins following logistic regression.
Frequency of consumption of various food items and hot beverages was presented using a heat map generated on Microsoft Excel using conditional formatting. Frequency of consumption of food items was re-categorized as “no consumption” when frequency is never eaten and as “consumption” for other options. Association between each food item and anaemia was determined using Chi square test. Association of IDA with independent variables such as age group, place of residence, socioeconomic status, parity, and dietary intake were analysed using binary logistic regression.
For socioeconomic status, upper and middle class were combined because there were very few participants (women with moderate or severe anaemia) in the upper social class. Purposeful selection was used for multivariable logistic regression analysis using a 3-step approach [49]. Bivariate logistic regression was done in step 1 and p-value threshold set at 0.25 for selection of variables for the model. In step 2, multivariable logistic regression was conducted with variables selected in step 1, entered in the model, and p-value threshold set at 0.05 for variables that were retained in the model. In step 3, all variables selected in step 2 were retained in the model. Sociodemographic variables which might have an impact on incidence of anaemia such as age, parity, socioeconomic status, geographical location, and gestation age were also included in the model in step 3. Subsequently variables dropped in steps 1 and 2 were included in sequence and any variable that caused a 10% change in the beta coefficient of any of the other variables in the model was retained.
Of the 872 participants included in this study, < 3% were missing any variable, and all analysis were done using complete cases. Statistical analysis was conducted using STATA version 16.0 statistical [50].
Ethics
Approval was obtained from the research ethics committees of all teaching hospitals, ministry of health or health service commission, and primary health care board before commencement of the IVON trial (details in the section on declaration). Eligible participants were invited for anaemia screening. They were counselled on the need for routine screening for anaemia during pregnancy and verbal consent obtained. Those with moderate or severe anaemia were further informed about IVON trial and invited to participate. They were informed that participation was voluntary and that they could withdraw participation at any time. An informed consent was signed by each participant before enrolment into IVON trial. Pregnant women aged 15 to less than 18 were considered able to provide consent themselves based on the International Ethical Guidelines for Health-related Research Involving Humans by the World Health Organization in 2016 which stated that in certain circumstances, minors may be considered emancipated if they are living independently, are married, have children of their own, or are pregnant [51]. In addition, the Federal Ministry of Health, Nigeria, in a report in 2014 deemed adolescents aged 14 and above fit to provide consent themselves in non-surgical sexual and reproductive health research if they are married, head of a household or emancipated [52].
Results
A total of 11,582 pregnant women were screened for anaemia, Fig. 1A including 5,182 women (44.7%) from Lagos and 6,400 (55.3%) from Kano state. A total of 3,681 (31.8%) of the women were screened in primary health centres, 6,213 (53.6%) in secondary health facilities, and 1,688 (14.6%) in tertiary facilities.
The prevalence of anaemia was 4,771/11,582 (41.2%, 95%CI: 40.3–42.1), and moderate or severe anaemia was 1,194/11,582 (10.3%, 95%CI: 9.8–10.9), as shown on Fig. 1B and C. Of the 1,194 pregnant women with moderate or severe anaemia, 1,048 were eligible for the IVON trial, and 909 (86.7%) of them consented Fig. 1D. Thirty-seven of the 909 participants were excluded from this study because one was enrolled after 32 weeks gestational age, two were enrolled below 20 weeks due to incorrect dating, and thirty-four did not have their serum ferritin reported, Fig. 1E.
A total of 872 pregnant women with moderate or severe anaemia were included in the analysis. The median age of the study participants was 27 (IQR: 23–32) years, with a median parity of 1 (IQR: 0–3), and 81.6% having at least secondary level of education, Table 1. Three hundred and fifty-nine had serum ferritin concentration < 30 ng/mL, meaning that iron deficiency was observed among 41.2% (95%CI: 37.9–44.5) of the women with moderate or severe anaemia (Table 2). Among pregnant women with moderate or severe anaemia, serum ferritin concentration was significantly lower among women enrolled in the early third trimester compared to those enrolled in late second trimester (p-value < 0.001), Table 2. The prevalence of malaria parasitaemia was 5.9% (95%CI: 4.4–7.7).
Among the 872 women with moderate or severe anaemia, sociodemographic and anthropometric characteristics such as age, parity, place of residence, level of education, socioeconomic status, income, and body mass index, among those with and without IDA were similar (Table 2). However, contribution of iron deficiency increased with gestational age in pregnant women with moderate or severe anaemia, from 28.4% (95%CI: 19.3–39.0%) at 20 weeks to 53.3% (95%CI: 26.6 – 78.7%) at 32 weeks, (Fig. 2).

Prevalence of iron deficiency anaemia among pregnant women with moderate or severe anaemia, by gestational age in weeks (n = 872)
Pearson chi2(12) = 30.1859 Pr = 0.003
Food consumption
Among the items in the FFQ, participants commonly consumed food items such as peanuts, soybeans, milk and milk products, green vegetables, red meat, poultry, beans, sea food, and beverages such as tea; most at a consumption frequency of every 2-3 weeks or 3–4 times a week (Fig. 3).

Heat map showing frequencies of food and beverage intake among study participants (n = 872)
Figures are presented as percentage of study participants who consume food item at specified frequency.
 75% or greater,
75% or greater,
 50-74.9%,
50-74.9%,
 25-49.9%,
25-49.9%,
 Less than 25%
Less than 25%
The prevalence of edible kaolin clay consumption among pregnant women with moderate or severe anaemia was 16.5% (95%CI: 14.1–19.2). The prevalence was found to be significantly higher in Kano state (19.4%, 95%CI: 15.8 – 23.4) compared to Lagos state (13.7%, 95%CI: 10.6 – 17.2%), p = 0.023. Compared to participants from Lagos, a significantly higher percentage of women in Kano state consumed turmeric (21.9% vs. 28.2%, p = 0.033) and soybeans (57.8% vs. 72.5%, p < 0.001). Compared to Kano, significantly more pregnant women in Lagos consumed turkey (45.5% vs. 64.2%, p < 0.001) and coffee (8.6% vs. 13.0%, p < 0.001). The consumption patterns of other foods were similar across the two states (p > 0.05).
Table 3 shows the results of bivariate association between food consumption by women with moderate or severe anaemia and IDA. There was a statistically significant association between any consumption of edible kaolin clay, soybeans, and green leafy vegetables and iron deficiency among pregnant women with moderate or severe anaemia. A larger proportion of those who consume soybeans had IDA compared to those who do not (41.6% versus 36.2%, p < 0.001). A larger proportion of those who consume edible kaolin clay had IDA compared to those who do not (54.2% versus 38.6%, p = 0.001). Whereas a greater proportion of pregnant women who do not consume green leafy vegetables had IDA compared to those who do (65% versus 41%, p = 0.029).
Tables 4, 5, 6 and 7 show the results of crude and multivariable logistic regression analysis of factors associated with IDA among pregnant women with moderate or severe anaemia. The adjusted odds for IDA was 57% higher in those at 27-32 weeks gestation compared to those at 20-26 weeks (95%CI:1,15-2.15). The adjusted odds for IDA was 70% higher in pregnant women aged 15-19 with moderate or severe anaemia compared to those in age group 20-34 years, though not statistically significant (aOR:1.70, 95%CI:0.91-3.18).
Pregnant women with malaria parasitaemia had 85% lower odds for IDA compared to pregnant women without malaria parasitaemia (aOR:0.15, 95%CI:0.06–0.38). Consumption of green leafy vegetables was found to be associated with 64 – 74% lower adjusted odds of having IDA compared to those who did not consume green vegetables. Pregnant women who consumed edible kaolin clay every day had nine times higher adjusted odds of having IDA compared to those who did not consume it at all (p < 0.001).
Discussion
This study showed that 10.3% of pregnant women recruited for the IVON trial at 20-32 weeks gestational age in public health facilities in Lagos and Kano states had moderate or severe anaemia, and 41.2% of those with moderate or severe anaemia were iron deficient. With increasing gestational age, the contribution of iron deficiency as a cause of anaemia increased from 1 in 4 pregnant women with moderate or severe anaemia at 20 weeks gestational age to 1 in 2 by 32 weeks. Dietary factors associated with higher odds of IDA included consumption of soybeans and edible kaolin clay, while consumption of green leafy vegetables reduced the odds.
The proportion of moderately-severely anaemic pregnant women with iron deficiency found in our study is consistent with an earlier systematic review showing that iron deficiency complicates 25 – 46% of anaemic pregnant women in Nigeria [26]. However, it is lower than prevalence of 64% in pregnant women with moderate or severe anaemia reported in a study in Zaria, a state in Northern Nigeria just like Kano [33]. The lower prevalence of IDA in our study may be partly explained by the differences in the exclusion criteria applied in both studies. We excluded pregnant women who were below 20 weeks or above 32 weeks gestational age, or had HIV, allergic to iron-containing medications or have autoimmune diseases and included only those who consented to partake in a clinical trial. Unlike the Zaria study, our study covered wider and different geographical areas, and recruited participants from all the three levels of public healthcare.
Our analysis confirmed published evidence that with increasing gestation, the incidence of IDA increases [53, 54]. Physiological changes in pregnancy such as an increase in plasma volume cause physiologic haemodilution, a plausible explanation for the increased incidence of anaemia during pregnancy [55]. However, this mechanism might not offer a plausible explanation for the increased incidence of IDA during pregnancy. Considering that pregnancy has been found to cause a two- to three-fold increase in iron demand for haematopoeisis and for the foetus [55], a possibility exists that the demand for iron during pregnancy increases as the foetus grows. However, whether the observed association between IDA and gestational age is a result of the anaemia, or the iron deficiency, or both is a question that calls for future research.
Although difference in prevalence of IDA across geographical locations might suggest location as a possible determinant for IDA, an association between state of residence and the prevalence of IDA was not found in our study. However, we found some disparities in dietary habit across states, as a higher proportion of pregnant women with moderate or severe anaemia in Kano compared to Lagos state consumed foods like soybeans and edible kaolin clay, which have been associated with IDA in this study. We found that daily consumption of edible kaolin clay was associated with a nine-fold increase in odds for IDA in pregnant women with moderate or severe anaemia in this study. Our study reported a prevalence of edible kaolin clay consumption of 16.5% in pregnant women with moderate and severe anaemia. The consumption of edible kaolin clay, during pregnancy, is well known among people from diverse cultures with prevalence of 35.4% in Cameroon [56], and 47.0 - 47.5% in Ghana [57, 58].
Some pregnant women eat edible kaolin clay to suppress pregnancy symptoms such as water brash and nausea, or just for the craving - pica [59, 60]. Edible kaolin clay is obtained from earth and contains kaolinite which prevents proper absorption of iron from the duodenum and might thus cause iron deficiency if consumed frequently [48]. Edible kaolin clay has been found to contain chemicals and heavy metals such as arsenic, lead, nickel, silicon, mercury, cadmium, anthraquinone, small amount of androgens and steroids, and some micro-organisms [61,62,63]. It will be beneficial to explore further the association between edible kaolin clay and IDA to determine if the association is a cause or an effect of IDA as earlier studies have given conflicting reports [48, 64].
Interestingly, eating soybeans 3 – 4 times a day was found to increase odds for IDA by 78% in this study. This conflicts earlier findings that soybeans reduces the incidence of anaemia and iron deficiency [65] because they contain low amounts of ferritin and thus enhance iron bioavailability [65,66,67]. Our finding is corroborated by a study in Chinese population which found a positive association between tofu (contains dried soybeans) intake and haemoglobin concentration, but an inverse association between tofu intake and serum ferritin levels in women [68]. The reason for this is unclear. However, it might be related to micronutrient damage from cooking methods [69] or due to differences in species of soybeans consumed in various regions as soybeans high in phenolic acids have been found to have a higher iron bioavailability compared to species low in phenolic acids [70]. There is a need to explore these possibilities in future research.
Green leafy vegetable consumption was found to be associated with a lower odds of IDA in this study. A recent randomized clinical trial conducted on children aged 4 – 9 years in Ghana involving nutritional intervention using green leafy vegetable powder found that children who consumed the powder had significantly lower prevalence of anaemia and vitamin A deficiency [71]. Similar association was found in a recent cross-sectional study on small scale female farmers in Tanzania [72]. Common green leafy vegetables in Nigeria such as Telfairia occidentalis popularly known as “Ugwu” and Amaranthus hybridus known locally as “Tete adayeba” have high iron concentrations of 0.70 ppm and 0.67 ppm respectively [73]. The high vitamin C content of green leafy vegetables facilitates the absorption and bioavailability of iron. Some studies found that in women with IDA, serum hepcidin and serum ferritin concentration were positively correlated with the frequency of intake of green leafy vegetables [74, 75].
Malaria parasitaemia was associated with lower odds of IDA in our study. Nevertheless, malaria parasitaemia is known to increase odds for anaemia by causing haemolysis [76]. Unlike anaemia which pathogenesis in relation to malaria parasitaemia is clear, the pathogenesis for iron deficiency is unclear. However, scholars propose that ferroportin, a transport protein in erythrocytes, prevents iron accumulation in erythrocytes [77]. This affects erythrocytic schizogony as malaria parasites cannot thrive in iron depleted red blood cells [78]. In addition, ferroportin has been found in abundance in erythrocytes in iron deficient states but diminished in iron replete states [77].
Strengths and limitations
Our study has several strengths compared to previous work in Nigeria, including a large sample size of women screened for anaemia and inclusion of several health facilities at various levels of healthcare (primary, secondary, and tertiary) located in different parts of the country (Northern and Southern Nigeria) [33, 79]. However, the exclusion of pregnant women seeking ANC in private health facilities, restriction to clinical trial participants, and the exclusion of the population of pregnant women within the community who are not attending any antenatal clinic, limits the generalizability of our findings and might have introduced some bias. Our study participants comprised mostly urban women with higher education, than what we would expect in Nigeria as a whole, based on the NDHS data [25]. Of the pregnant women who received ANC in sub-Saharan Africa, 81.2% received care from the public sector while about 15% received ANC from the commercial and not-for-profit private health facilities [80]. We can also not completely rule out the possibility of residual confounding and reverse causality in this study, especially regarding the association with edible kaolin clay consumption.
Based on our findings, there is a need for advocacy on early registration for ANC and regular ANC appointments to facilitate prevention or early diagnosis of IDA bearing in mind the association with increasing gestational age. Screening for iron deficiency in anaemic pregnant women with risk factors for IDA should be considered globally especially in sub-Saharan Africa where the burden of IDA is highest. Focused dietary intervention programmes need to be included in guidelines for management of IDA especially in settings where the compliance rate for the use of haematinics during pregnancy is low. There is a need to discourage consumption of edible kaolin clay, as it is clear from this and other studies that frequent consumption of edible kaolin clay in large amount poses significant health risk; this can be integrated into health education sessions within ANC. Whether non-consumption of edible kaolin clay will reduce incidence of IDA during pregnancy remains debatable, as there has been arguments on possibility of edible kaolin clay consumption being an effect rather than a cause of IDA [48, 64].
Almost 60% of the moderately or severely anaemic pregnant women in this study did not have iron deficiency, suggesting that their anaemia is due to other factors. The prevalence of malaria parasitaemia was also low (5.9%), despite the enrolment period spanning through the peak period of malaria transmission, April to October, in Nigeria [81]. This raises the need to explore in future research other causes of anaemia in pregnant Nigerian women. It will also be of interest in future research to estimate the proportion of non-anaemic pregnant women who are iron-deficient as such women could be effectively managed with dietary modifications alone, considering that non-anaemic iron deficiency has been associated with a higher risk of developing anaemia in pregnancy, increased incidence of low birth weight and neurodevelopmental problems in infants of affected mother [82,83,84].
Conclusion
In our study, 4 in 10 women with moderate or severe anaemia during pregnancy had IDA. We provide evidence for the protective effect of green leafy vegetables against IDA while self-reported consumption of edible kaolin clay and soybeans appeared to increase the odds of having IDA during pregnancy. Our findings have implications for practice and research. They call for evaluation of health education interventions and focused dietary advice and modification during pregnancy since these could potentially increase awareness and change behaviours that could reduce IDA among pregnant women with moderate or severe anaemia in Nigeria and beyond as strategies to improve maternal and perinatal outcomes. Our findings also raise other research questions worth exploring in future research to improve scientific knowledge worldwide on iron deficiency anaemia during pregnancy.
Availability of data and materials
The enrolment data of the ongoing IVON trial was used for this study. The complete dataset analysed for this study is available in the Open Science Framework data repository platform. The link to the dataset is: https://osf.io/6g8fw/.
Abbreviations
- 95%CI:
-
95% Confidence interval
- ANC:
-
Antenatal care
- ANOVA:
-
Analysis of variance
- FFQ:
-
Food frequency questionnaire
- g/dL:
-
Grammes per decilitre
- Hb:
-
Haemoglobin
- HIV:
-
Human immunodeficiency virus
- IDA:
-
Iron deficiency anaemia
- IVON:
-
Intravenous versus oral iron for iron deficiency anaemia in pregnant Nigerian women
- kg/m2:
-
Kilogramme per square metre
- mL:
-
Millilitre
- NDHS:
-
Nigeria Demographic Health Survey
- ng/mL:
-
Nanograms per millilitre
- NGN:
-
Nigerian naira
- NHREC:
-
National Health Research Ethics Committee
- OR:
-
Odds ratio
- ppm:
-
Parts per million
- REDCap:
-
Research electronic data capture
- RLUs:
-
Relative light units
- RR:
-
Relative risk
- WHO:
-
World Health Organization
References
WHO. Anaemia. World Health Organization. 2023. Accessed: 02 Nov 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/anaemia#:~:text=Globally%2C%20it%20is%20estimated%20that,due%20to%20disability%20in%202019.
Brabin BJ, Hakimi M, Pelletier D. An analysis of anemia and pregnancy-related maternal mortality. J Nutr. 2001;131(2):604S-S615.
Debella A, Eyeberu A, Getachew T, Atnafe G, Geda B, Dheresa M. Perinatal outcomes in anemic pregnant women in public hospitals of eastern Ethiopia. Int Health. 2023;15(3):274–80. https://doi.org/10.1093/inthealth/ihac021.
French SA, Tangney CC, Crane MM, Wang Y, Appelhans BM. Nutrition quality of food purchases varies by household income: the SHoPPER study. BMC Public Health. 2019;19(1):231.
GBD 2021 Anaemia Collaborators. Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990–2021: findings from the Global Burden of Disease Study 2021. Lancet Haematol. 2023;10(9):e713–34.
Merid MW, Chilot D, Alem AZ, Aragaw FM, Asratie MH, Belay DG, et al. An unacceptably high burden of anaemia and it’s predictors among young women (15–24 years) in low and middle income countries; set back to SDG progress. BMC Public Health. 2023;23(1):1292.
Worldometer. 7 continents. Accessed: 02 Nov 2023. Available from: https://www.worldometers.info/geography/7-continents/.
Sunuwar DR, Singh DR, Chaudhary NK, Pradhan PMS, Rai P, Tiwari K. Prevalence and factors associated with anemia among women of reproductive age in seven South and Southeast Asian countries: evidence from nationally representative surveys. PLoS One. 2020;15(8):e0236449.
Sinha A, Adhikary M, Phukan JP, Kedia S, Sinha T. A study on anemia and its risk factors among pregnant women attending antenatal clinic of a rural medical college of West Bengal. J Family Med Prim Care. 2021;10(3):1327–31.
van den Broek N. Anaemia and micronutrient deficiencies: Reducing maternal death and disability during pregnancy. Br Med Bull. 2003;67(1):149–60.
Wessells KR, Ouédraogo CT, Young RR, Faye MT, Brito A, Hess SY. Micronutrient status among pregnant women in Zinder, Niger and risk factors associated with deficiency. Nutrients. 2017;9(5):430.
Omotayo MO, Abioye AI, Kuyebi M, Eke AC. Prenatal anemia and postpartum hemorrhage risk: a systematic review and meta-analysis. J Obstet Gynaecol Res. 2021;47(8):2565–76.
Smith C, Teng F, Branch E, Chu S, Joseph K. Maternal and perinatal morbidity and mortality associated with anemia in pregnancy. Obstet Gynecol. 2019;134(6):1234–44.
McMahon LP. Iron deficiency in pregnancy. Obstet Med. 2010;3(1):17–24.
Tandon R, Jain A, Malhotra P. Management of iron deficiency anemia in pregnancy in India. Indian J Hematol Blood Transfus. 2018;34(2):204–15.
Aspuru K, Villa C, Bermejo F, Herrero P, López SG. Optimal management of iron deficiency anemia due to poor dietary intake. Int J Gen Med. 2011;4:741–50.
Fouelifack FY, Sama JD, Sone CE. Assessment of adherence to iron supplementation among pregnant women in the Yaounde gynaeco-obstetric and paediatric hospital. Pan Afr Med J. 2019;34:211.
Siabani S, Siabani S, Siabani H, Moeini Arya M, Rezaei F, Babakhani M. Determinants of compliance with iron and folate supplementation among pregnant women in West Iran: a population based cross-sectional study. J Family Reprod Health. 2018;12(4):197–203.
Osman MO, Nour TY, Bashir HM, Roble AK, Nur AM, Abdilahi AO. Risk factors for anemia among pregnant women attending the antenatal care unit in selected jigjiga public health facilities, Somali Region, East Ethiopia 2019: unmatched case-control study. J Multidiscip Healthc. 2020;13:769–77.
Mf Y. Maternal anaemia and risk of mortality: a call for action. The Lancet. 2018;6(5):E479–80.
Sanghvi TG, Harvey PWJ, Wainwright E. maternal iron-folic acid supplementation programs: evidence of impact and implementation. Food Nutr Bull. 2010;31(2_suppl2):S100–7.
Carpenter RM, Billah SM, Lyons GR, Siraj MS, Rahman QS, Thorsten V, et al. U-Shaped Association between Maternal Hemoglobin and Low Birth Weight in Rural Bangladesh. Am J Trop Med Hyg. 2021;106(2):424–31.
Dewey KG, Oaks BM. U-shaped curve for risk associated with maternal hemoglobin, iron status, or iron supplementation. Am J Clin Nutr. 2017;106(Suppl 6):1694s-s1702.
Ali SA, Tikmani SS, Saleem S, Patel AB, Hibberd PL, Goudar SS, et al. Hemoglobin concentrations and adverse birth outcomes in South Asian pregnant women: findings from a prospective Maternal and Neonatal Health Registry. Reprod Health. 2020;17(2):154.
NDHS. Nigeria Demographic and Health Survey [FR359] 2018. p. 174, 268 pp. Available from: https://dhsprogram.com/pubs/pdf/FR359/FR359.pdf.
Ugwu N, Uneke C. Iron deficiency anemia in pregnancy in Nigeria—A systematic review. Niger J Clin Pract. 2020;23(7):889–96.
De R, Prakash KU, Edison ES. complex interactions in regulation of haematopoiesis-an unexplored iron mine. Genes (Basel). 2021;12(8):1270.
USAID. A rapid initial assessment of the distribution and consumption of iron-folic acid tablets through antenatal care in Nigeria. 2014. Cited 2023 1 Apr 2023. Available from: https://www.spring-nutrition.org/publications/briefs/iron-folic-acid-assessment-nigeria.
Adeboye TE, Bodunde IO, Okekunle AP. Dietary iron intakes and odds of iron deficiency anaemia among pregnant women in Ifako-Ijaiye, Lagos, Nigeria: a cross-sectional study. Pan Afr Med J. 2022;42:23.
Shi H, Chen L, Wang Y, Sun M, Guo Y, Ma S, et al. Severity of anemia during pregnancy and adverse maternal and fetal outcomes. JAMA Network Open. 2022;5(2):e2147046-e.
Afolabi BB, Babah OA, Akinajo OR, Adaramoye VO, Adeyemo TA, Balogun M, et al. Intravenous versus oral iron for iron deficiency anaemia in pregnant Nigerian women (IVON): study protocol for a randomised hybrid effectiveness-implementation trial. Trials. 2022;23(1):763.
National Bureau of Statistics. Demographic statistics bulletin. 2020. Available from: https://nigerianstat.gov.ng/elibrary/read/1241121.
Hassan A-A, Mamman A, Adaji S, Musa B, Kene S. Anemia and iron deficiency in pregnant women in Zaria Nigeria. Sub-Saharan Afr J Med. 2014;1(1):36–9.
Bolarinwa OA. Sample size estimation for health and social science researchers: the principles and considerations for different study designs. Niger Postgrad Med J. 2020;27(2):67–75.
WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. World Health Organization. 2011. Cited 2022 July 24. Available from: https://apps.who.int/iris/handle/10665/85839.
Achebe MM, Gafter-Gvili A. How I treat anemia in pregnancy: iron, cobalamin, and folate. Blood. 2017;129(8):940–9.
van den Broek NR, Letsky EA, White SA, Shenkin A. Iron status in pregnant women: which measurements are valid? Br J Haematol. 1998;103(3):817–24.
Pavord S, Daru J, Prasannan N, Robinson S, Stanworth S, Girling J, et al. UK guidelines on the management of iron deficiency in pregnancy. Br J Haematol. 2020;188(6):819–30.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Abbott. Bioline™ MALARIA Ag P.f. 2018. Available from: https://www.globalpointofcare.abbott/en/product-details/bioline-malaria-ag-pf-hrp-2.html.
Abott. Ferritin. ARCHITECT system.2010. 10 September 2022. Available from: https://www.ilexmedical.com/files/PDF/Ferritin_ARC.pdf.
Psaki SR, Seidman JC, Miller M, Gottlieb M, Bhutta ZA, Ahmed T, et al. Measuring socioeconomic status in multicountry studies: results from the eight-country MAL-ED study. Popul Health Metrics. 2014;12(1):8.
Ibadin M, Akpede GO. A revised scoring scheme for the classification of socio-economic status in Nigeria. Niger J Paediatr. 2021;48(1):26–33.
Singhal S, Goyle A, Gupta R. Quantitative food frequency questionnaire and assessment of dietary intake. Natl Med J India. 1998;11(6):268–75.
Smith TJ, Ashar BH. Iron deficiency anemia due to high-dose turmeric. Cureus. 2019;11(1):e3858.
Al-Basher GI. Green tea activity and iron overload induced molecular fibrogenesis of rat liver. Saudi J Biol Sci. 2019;26(3):531–40.
Madziva C, Chinouya MJ. Clay Ingestion during pregnancy among Black African Women in a North London Borough: understanding cultural meanings, integrating indigenous and biomedical knowledge systems. Frontiers in Sociology. 2020;5:20.
Attarha BO, Mikulic S, Harris C, Scolapio JS. Kaolin clay anemia. Cureus. 2021;13(3):e13796.
Zhang Z. Model building strategy for logistic regression: purposeful selection. Ann Transl Med. 2016;4(6):111.
StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC; 2019.
WHO. International Ethical Guidelines for Health-related Research Involving Humans. World Health Organization. 2016. Available from: https://cioms.ch/wp-content/uploads/2017/01/WEB-CIOMS-EthicalGuidelines.pdf.
FMOH. A Consensus Report on Guidelines for Young Persons’ Participation in Research and Accessing Sexual and Reproductive Health Services in Nigeria. Federal Ministry of Health, Nigeria. 2014. Available from: https://www.popcouncil.org/uploads/pdfs/2014HIV_YoungPersonsSRH-Nigeria.pdf.
Fite MB, Assefa N, Mengiste B. Prevalence and determinants of Anemia among pregnant women in sub-Saharan Africa: a systematic review and Meta-analysis. Arch Public Health. 2021;79(1):219.
Zeisler H, Dietrich W, Heinzl F, Klaritsch P, Humpel V, Moertl M, et al. Prevalence of iron deficiency in pregnant women: a prospective cross-sectional Austrian study. Food Sci Nutr. 2021;9(12):6559–65.
Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89–94.
Essome H, Engbang JPN, Ndedi GP, Valère MK, Boten M, Foumane P, et al. Kaolin clay consumption and pregnancy: prevalence, hematological consequences and outcome of labour in the Douala. Open J Obstetr Gynecol. 2017;07:1166–73.
Konlan KD, Abdulai JA, Konlan KD, Amoah RM, Doat A-R. Practices of pica among pregnant women in a tertiary healthcare facility in Ghana. Nurs Open. 2020;7(3):783–92.
Mensah FO, Twumasi P, Amenawonyo XK, Larbie C, Jnr AKB. Pica practice among pregnant women in the Kumasi metropolis of Ghana. Int Health. 2010;2(4):282–6.
Owumi SE, Oyelere AK. Determination of metal ion contents of two antiemetic clays use in Geophagy. Toxicol Rep. 2015;2:928–32.
Madziva C, Chinouya MJ. Clay ingestion during pregnancy among Black African Women in a North London Borough: understanding cultural meanings, integrating indigenous and biomedical knowledge systems. Front Sociol. 2020;5:20.
Odimegwu JI. Jane-Sharon EE. Nkemehule FE. Okunnuga J. Buhari AO. Okwuegbuna SN, et al. Craving edible clays: anemia or androgens. Glob J Chem Sci. 2021;1(1). https://doi.org/10.53996/2769-6170.gjcs.1000105.
Lar U, Dang, Ogunmola. The effects of geophagy on pregnant Women in Nigeria. Am J Hum Ecol. 2014;3:1–9.
Kortei NK, Annor IA, Aboagye G, Manaphraim NYB, Koryo-Dabrah A, Awude E, et al. Elemental minerals and microbial compositions as well as knowledge and perceptions regarding kaolin (clay) consumption by pregnant women in the Ho municipality of Ghana. Pan Afr Med J. 2019;34:113.
Borgna-Pignatti C, Zanella S. Pica as a manifestation of iron deficiency. Expert Rev Hematol. 2016;9(11):1075–80.
Li L, Zhong W, Kong H, Sun J, Zhang X, Su Y. Evaluation of the Effect of sprout soybeans on the iron status of anemic adolescent girls in Rural China. Plant Foods Hum Nutr. 2019;74(1):28–33.
Lönnerdal B. Soybean ferritin: implications for iron status of vegetarians. Am J Clin Nutr. 2009;89(5):1680S-S1685.
Murray-Kolb LE, Welch R, Theil EC, Beard JL. Women with low iron stores absorb iron from soybeans. Am J Clin Nutr. 2003;77(1):180–4.
Shi Z, Hu X, Yuan B, Pan X, Dai Y, Holmboe-Ottesen G, et al. Strong Negative Association between Intake of Tofu and Anemia among Chinese Adults in Jiangsu, China. J Am Diet Assoc. 2008;108(7):1146–53.
Pereira EJ, Carvalho LM, Dellamora-Ortiz GM, Cardoso FS, Carvalho JL, Viana DS, et al. Effects of cooking methods on the iron and zinc contents in cowpea (Vigna unguiculata) to combat nutritional deficiencies in Brazil. Food Nutr Res. 2014;58. https://doi.org/10.3402/fnr.v58.20694.
Sha X, Chen H, Zhang J, Zhao G. Iron release from soybean seed ferritin induced by cinnamic acid derivatives. Pharmaceuticals (Basel). 2018;11(2):39.
Egbi G, Gbogbo S, Mensah GE, Glover-Amengor M, Steiner-Asiedu M. Effect of green leafy vegetables powder on anaemia and vitamin-A status of Ghanaian school children. BMC Nutrition. 2018;4(1):27.
Stuetz W, Gowele V, Kinabo J, Bundala N, Mbwana H, Rybak C, et al. Consumption of dark green leafy vegetables predicts vitamin a and iron intake and status among female small-scale farmers in Tanzania. Nutrients. 2019;11(5):1025.
Dawodu O. Determination of iron content in indigenous vegetables. 2020.
Mayasari NR, Bai CH, Hu TY, Chao JCJ, Chen YC, Huang YL, et al. Associations of food and nutrient intake with serum hepcidin and the risk of gestational iron-deficiency anemia among pregnant women: a population-based study. Nutrients. 2021;13(10):3501.
Ghatpande NS, Apte PP, Naik SS, Kulkarni PP. Fruit and vegetable consumption and their association with the indicators of iron and inflammation status among adolescent girls. J Am Coll Nutr. 2019;38(3):218–26.
Joseph CM, Albert MT, Herman TK, Jules NT, Zambèze KS, Prospe KMK. Prevalence and associated factors of anemia during pregnancy in Lubumbashi, in the south of Democratic Republic of Congo: situation in 2020. PAMJ Clin Med. 2021;7:19. https://doi.org/10.11604/pamj-cm.2021.7.19.28351.
Zhang DL, Wu J, Shah BN, Greutélaers KC, Ghosh MC, Ollivierre H, et al. Erythrocytic ferroportin reduces intracellular iron accumulation, hemolysis, and malaria risk. Science. 2018;359(6383):1520–3.
Rosenthal PJ, Meshnick SR. Hemoglobin catabolism and iron utilization by malaria parasites. Mol Biochem Parasitol. 1996;83(2):131–9.
Ajepe AA, Okunade KS, Sekumade AI, Daramola ES, Beke MO, Ijasan O, et al. Prevalence and foetomaternal effects of iron deficiency anaemia among pregnant women in Lagos, Nigeria. PLoS One. 2020;15(1):e0227965.
Powell-Jackson T, Macleod D, Benova L, Lynch C, Campbell OM. The role of the private sector in the provision of antenatal care: a study of Demographic and Health Surveys from 46 low- and middle-income countries. Trop Med Int Health. 2015;20(2):230–9.
Ayanlade S, Adeoye N, Babatimehin O. Intra-annual climate variability and malaria transmission in Nigeria. Bull Geogr Socioeconomic Ser. 2013;21:7–19.
Balendran S, Forsyth C. Non-anaemic iron deficiency. Aust Prescr. 2021;44(6):193–6.
Ribot B, Aranda N, Viteri F, Hernández-Martínez C, Canals J, Arija V. Depleted iron stores without anaemia early in pregnancy carries increased risk of lower birthweight even when supplemented daily with moderate iron. Hum Reprod. 2012;27(5):1260–6.
Al-Naseem A, Sallam A, Choudhury S, Thachil J. Iron deficiency without anaemia: a diagnosis that matters. Clin Med (Lond). 2021;21(2):107–13.
Acknowledgements
Appreciation to the IVON trial team for the joint effort in collecting data for this study at the various study sites.
Funding
Open access funding provided by Karolinska Institute. “This work was supported in whole, by the Bill & Melinda Gates Foundation (Investment ID INV-017271) grant for the research titled “Intravenous versus oral iron for iron deficiency anaemia in pregnant Nigerian women (IVON): an open label, randomized controlled trial”, which principal investigator is Professor Bosede B. Afolabi. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission. The funding agency was not involved in the conceptualization of this research idea, data collection, data analysis, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
OAB, BBA, ECL, LB, CH, ABT conceptualized the research ideas. OAB, BBA, ORA, VOA, TAA, MRB, HSG, and NASA were involved in the IVON project monitoring and data collection activities. OAB performed the data analysis under supervision of AIA and LB. OAB prepared the manuscript under the supervision of ECL, BBA, LB, and CH with contributions from AIA, ABT, NASA, HSG, ORA, TAA, MRB, and VOA. BBA was the Principal Investigator of the IVON trial from which enrolment data for this study was extracted. BBA, ECL, CH, and LB reviewed and approved the project title and proposal, supervised the conduct of the research and manuscript preparation as part of the doctoral training of OAB. All authors endorsed the last version of the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained for IVON trial from Lagos University Teaching Hospital HREC (ADM/DCST/HREC/APP/3971), Lagos State Health Service Commissions (LSHSC/2222/VOLIII), Lagos state Primary Health Care Board (LS/PHCB/MS/1128/VOL.VII/100), Aminu Kano Teaching Hospital, Kano (NHREC/28/01/2020/AKTH/EC/2955), Ministry of Health, Kano (MOH/Off/797/T.1/2102) and National Health Research Ethics Committee (NHREC/01/01/2007-04/02/2021). Informed consent was obtained from all participants before enrolment into the study. The research was conducted in accordance with the ethical principles set in the Declaration of Helsinki.
Consent for publication
Not applicable to this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary file 1.
Food frequency questionnaire
Additional file 2: Supplementary file 2.
Summary of screening and inclusion into study by state and facility level.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Babah, O.A., Akinajo, O.R., Beňová, L. et al. Prevalence of and risk factors for iron deficiency among pregnant women with moderate or severe anaemia in Nigeria: a cross-sectional study. BMC Pregnancy Childbirth 24, 39 (2024). https://doi.org/10.1186/s12884-023-06169-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-06169-1