
Abstract
Background
Lung cancer is the second most diagnosed cancer in the world. Up to 84% of diagnosed patients have malnutrition, which can negatively affect quality of life and survival and may worsen with neoadjuvant treatment. Bioelectrical Impedance Analysis-Derived Phase Angle (PhA) in these patients could be a valid tool to assess the nutritional status in order to improve their condition.
Methods
This review provides an update on PhA assessment in lung cancer patients over the past twenty years. We searched PubMed, Embase, Scopus, Web of Science, and Cochrane, for articles regarding the PhA obtained from Bioelectrical Impedance Analysis in lung cancer patients. The authors independently performed a literature search: sample size, patient population, study type, study dates, survival and interventions were evaluated. The final review included 11 studies from different countries.
Results
Eight studies only considered patients with lung cancer, while three studies considered patients with different kind of cancer, including lung. Correlation data between PhA and age are conflicting. In patients undergoing clinical treatment and patients undergoing surgical treatment lower PhA was observed. A lower PhA is associated with a shorter survival. In three studies emerged a relationship between Karnofski Performance Status and Handgrip Strenght with PhA. From one study, univariate logistic regression analysis showed that higher PhA values represent a protective factor for sarcopenia.
Conclusion
Our research underlined interesting, but not conclusive, results on this topic; however more researches are needed to understand the clinical meaning of PhA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung Cancer (LC) is the second most diagnosed cancer worldwide, especially in males. Most recent data have shown an incidence of 2.2 million of new cases (11.4%) and 1,8 million of deaths (18.0%) occurred in 2020. It represents leading cause of cancer death in 93 countries [1]. Following diagnosis, 5-year survival rates ranges from 10 to 20% in most countries, with higher rates in Japan (33%), Israel (27%), and Korea (25%) [1]. In Italy, LC showed a 5-year survival of 16% in men and 23% in women [2]. LC aetiology is multifactorial and complex. In addition to a family history of LC, tobacco smoke currently represents the leading risk factor [2, 3]. Second-hand tobacco use may also increase LC risk, causing more than 3.000 deaths each year [4]. Other lung carcinogens include inhaled chemicals such as arsenic, cadmium and asbestos [5].
LCs are traditionally classified in small cell lung carcinoma (SCLC) and non-small cell lung carcinoma (NSCLC) divided into four major classes (adenocarcinoma, squamous cell carcinoma and large cell carcinoma) [6]. Conventional LC therapies include surgical intervention for resectable diseases and, in selected cases, a combination of radiotherapy (RT) and chemotherapy (CHT) for locally advanced or metastatic disease. Advancements in the understanding of LC molecular pathogenesis has led to the development of targeted strategies like immune checkpoint inhibitor (ICI) in first and later lines of treatment [7].
In addition to cancer-related symptoms, including chronic cough, dyspnoea, pain and adverse effects from anti-neoplastic treatments, LC patients’ may experience fatigue, weight loss or nutritional status alterations, such as malnutrition [8, 9]. Cancer patients are more likely to become malnourished, with a prevalence ranging from 20.0% to 80.0% [10]. Recent studies indicate that dietary nutrient deficiency in cancer patients may induce unintentional body weight loss to sarcopenia, up to cachexia [11]. It is known that malnutrition was prevalent in advanced LC patients [12]: up to 84% of them showed malnutrition status during illness, which can be worsened by ongoing neoadjuvant treatment [12,13,14,15,16,17]. This condition has been associated with poorer prognosis, decreased treatment response, poorer tolerance to treatment, lower quality of life (QoL) and increased healthcare costs [12, 18]. Additionally, sarcopenia, defined as progressive loss of muscle mass and functioning, is highly prevalent among LC patients ranging from 42.8% to 45.0%, in association with increased postoperative complications and increased risk of mortality, regardless of cancer stage and treatment [19]. Furthermore, LC is more commonly linked to cancer cachexia than other types of cancer [16], characterized mainly by a decrease in muscle strength, due to the loss of adipose tissue and skeletal mass [20, 21].
Body Composition (BC) is a crucial requirement for the overall body assessment of cancer patients: it can reflect the nutritional status of patients and predict clinical outcomes and prognosis [22]. Bioelectrical Impedance Analysis (BIA) is a simple, cost-effective and non-invasive method that measures electrical characteristics of human body, i.e. impedance (Z), through application of four electrodes and an applied alternate current, using single (SF-BIA) or multiple (MF-BIA) current frequencies. Z derives from resistive component (Resistance, R) and capacitive component (Reactance, Xc), by equation Z = R2 + Xc2. R indicates how much a substance opposes the flow of electric current: greater resistance indicates greater difficulty of passage. It can be affected by factors such as tissue density or hydration and cell membrane permeability. Reactance reflects the ease with which electricity can flow through tissues: high reactance means that there is more resistance of tissues and less conductivity. It can therefore indicate cellular and membrane integrity.
BIA-derived Phase Angle (PhA) is obtained as [arctangent (Xc /R) × 180°/π]. PhA represent an indicator of cellular health, cell membrane integrity, and better cell function: low values are indicators of apoptosis and cell matrix alteration [23, 24]. Therefore, BIA analysis and the use of the PhA have a good consistency in the application in cancer patients to evaluate nutritional and hydration status [25, 26]. Despite importance of nutritional status and BC for the clinical evaluation of cancer patients, these conditions remain in part an undertreated issue [27]. Thus, nutritional status assessment of these patients is essential for adequate nutritional support, and may also improve QoL and consequently survival post-diagnosis [28, 29]. In the literature, a large number of publications on BIA and in particular of PhA assessment, confirm its prognostic role in different types of cancer (e.g., breast, pancreatic and colon) [30,31,32,33]. Although PhA is a useful prognosis tool even in patients with LC [34], this has not been discussed in detail in scientific literature. So, our review aims to critically report and discuss available clinical data relating to PhA in LC patients, to provide a broad and clear picture of topic.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for performing the present review, considering the possibility of including both cross-sectional and longitudinal studies. Further details about PRISMA checklist and study protocol were provided in Supplementary File. Due to the study type, ethical approval was not required. This systematic revision is not currently registered in any database.
Data sources
Authors independently performed a systematic literature research between 2000 and 2023 of the electronic databases PubMed, Embase, Scopus, Web of Science and Cochrane. The following terms were used as search strategy string on full texts: phase angle" AND (lung or pulmonary) AND (bioelectrical OR impedance OR bia) AND cancer”, "phase angle" AND (bia OR bioelectrical OR bioimpedance) AND cancer”. Zotero and EndNote X7 citation management software were used to manage citations.
Criteria for analysis
In this review, cross-sectional, case–control, and longitudinal studies were included. The measurement of PhA values by BIA was a necessary and indispensable condition for an article to be included. The studies had to be present in the literature in English form and had to be published no earlier than 2000 to include the most recent evidence. Outcome of interest included associations between PhA and survival, mortality, or other variables related to LC patients. Furthermore, it was necessary that studies must have been conducted in the health field. Articles that did not meet these requirements were excluded from the review. All studies include a phase-sensitive BC measurement tool. In all selected studies PhA is calculated by the ratio of R to Xc equal to [arctangent (Xc /R) × 180°/π. BC parameters were not obtained by predictive regression models.
Data extraction and analysis
To assess the suitability of the articles obtained from the literature search, authors carefully and meticulously examined all the titles and abstracts. Subsequently, the authors independently extracted the data from the papers and reported in an excel file. The data included: first author, year of publication, country of origin, design of study, sample size, age, sex, presence of control groups, type of tumour, methods used (BIA, BIVA), focusing on PhA.
Results
Selected studies
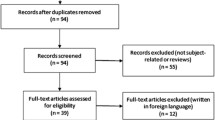
One hundred and sixty-five papers were identified from the systematic search, 92 from Pubmed, 32 from Embase, 6 from Scopus and 38 from Web of Science. After removing duplicates (n = 38), 120 articles were excluded, including 2 reviews, 1 symposium and 117 that did not concern LC. A total of 11 full-text articles were selected for eligibility, as shown in Fig. 1.

Flowchart
General characteristics of included studies
This systematic review includes several types of studies: five prospective studies [35,36,37,38,39], three observational studies [40,41,42], two retrospective studies [34, 43] and one cross-sectional study [44]. Shi et al. showed the highest number of patients involved (804). The remaining selected scientific papers included 30 to 204 patients. Five studies included both males and females, six studies included males only [36, 38, 40,41,42, 44]. However, in two studies [36, 37], we do not know if the percentages of women and men present in the study referred to LC patients or patients with other kind of cancers. General characteristics of studies included in this review are shown completely in Table 1.
Relationship between PhA, general characteristics and cancer features
Four studies investigated the potential relationship between age and PhA. In the study by Ji et al. [36], Pearson’s analysis showed an inverse correlation for age (r = -0.238 p = < 0.001). Shi et al. [39], showed both for men and women, higher PhA in younger (for both, p < 0.001); Spearman’s correlation analysis also showed that PhA was significantly correlated with age (men, r = -0.46, p < 0.001; women, r = -0.24, p < 0.001). In Castanho et al. [44], Pearson’s correlation showed no significant results between PhA and age (r = -0.32). Suzuki et al. showed a negative correlation between age and PhA (r = -0.51; p < 0.001); Spearman’s correlation was used to assess the correlation between age and PhA.
Only 8 of 11, considered data on patients with LC, while 3 studies considered patients with different types of cancer, including LC. Three other studies investigate PhA in different types of cancer, including LC: they respectively include 8, 244 and 26 patients with LC [36, 37, 45]. All studies showed patients with confirmed cancer diagnosis: five studies evaluated NSCLC patients with stage III and IV [34, 38, 40,41,42]. Shi et al. included adenocarcinoma, squamous cell carcinoma, SCLC and other type of LC patients in different stage of disease (from I to IV) [39]. Suzuki et al. and Hui et al. showed data on LC patients but did not specify cancer type or stage [43, 45]. Cancer stage was not specified in two studies [36, 37]. Castanho et al. [44] considered LC patients presenting from stage IB to IIIB. Results showed, by multifactorial analysis of variance, correlations between PhA and tumour size (r = -0.55; p < 0.001) or Karnofski Performance Status (KPS) (r = 0.44; P < 0.05). Three studies included patients not undergoing CHT, RT and without specific treatment information [37, 39, 45] while newly diagnosed patients and/or patients with ongoing therapies were evaluated in remaining studies [34, 36, 38, 42]. Suzuki et al. [43] evaluated LC patients after surgery while patients were evaluated after cancer treatment in two studies [40, 41]. Castanho et al. [44] evaluated patients after surgery and after cancer treatment (CHT, RT).
Relationship between PhA and body composition
The main associations identified in selected studies, between PhA and different variables, are shown in Table 2. In seven studies parameters related to BC have been evaluated [36, 39,40,41, 43, 44]. Castanho et al. [44] correlates PhA with arm circumference and weight loss over time. Authors also indicate that between patients undergoing surgery, those with lowest survival (52 days) showed a lower PhA (3.8°) and a High Extracellular Mass/Body Cell Mass (ECM:BCM) ratio (1:5), independent from tumour size. Whereas, in those treated medically, patients with a lower survival also had lowest PhA (3.9°) and highest ECM/BCM ratio (1:6), this were related to tumour volume (849 ml).
Shi et al. [39] shows that male patients < 65 years, with a lower Body Mass Index (BMI) and lower cancer stage have higher PhA values, but the differences were not statistically significant. In Suzuki et al. [43], Spearman’s correlation showed a positive correlation between PhA and BMI (rho = 0.29; p < 0.001); no correlation with body Fat Mass (FM) was found. In Hui et al. [45] study, PhA was associated with several known prognostic variables, including Fat-Free Mass (FFM) and FFM index (FFMI). However, the Spearman correlation was weak (rho < 0.4; p < 0.001). Two articles assessed different aspect within the same LC patients' population (Stage IV, male patients), including PhA. In Detopoulou et al. [40] were found significant correlations between PhA and FFM (rho = 0.247; p = 0.02), but no significant correlation for waist and hip circumference (cm), waist-hip ratio, body fat (%), BCM (Kg), total body water (TBW), extra-cellular and intra-cellular water (ECW, ICW). In the other study, Spearman’s correlation shows no significance between PhA, anthropometric and BC variables [41]. In Wei Ji et al. [36], in addition to PhA, other variables were also examined, such as appendicular skeletal muscle mass (ASMM), BMI and skeletal muscle mass index (SMI). Pearson’s correlations showed a moderate correlation between PhA values and variables considered (ASMM r = 0.301, p < 0.001; BMI r = 0.450, p < 0.001; SMI r = 0.463, p < 0.001.
Relationship between PhA, nutritional status and nutritional risk
PhA relationships with nutritional status and malnutrition screening scores were evaluated. Shi et al. indicated a significant correlation between PhA and some nutritional index: results of Spearman’s rank correlation test showed correlation with Nutritional Risk Score-2002 (NRS-2002) (men, r = − 0.25, p < 0.001; women, r = − 0.15, p < 0.001). No correlation between PhA and Patient-Generated Subjective Global Assessment (PG-SGA) score was found. Then, logistic regression analysis showed significant correlation between PhA, NRS-2002 score (men, p < 0.001; women, p < 0.001) and PG-SGA score (men, p < 0.001; women, p < 0.001) in both men and women, indicating an association with secondary clinical outcomes such as nutrition and well-being [39]. In Suzuki et al. [43], Spearman’s correlation showed a positive correlation between PhA and albumin (rho = 0.33; p < 0.001), considered a useful biochemical markers for nutrition assessment, and Prognostic Nutritional Index (PNI) (rho = 0.32; p < 0.001), a simple index obtained from serum albumin concentration and total peripheral blood lymphocyte count, used to assess the immune-nutritional status of patients who undergo surgery. In Hui et al. [45] study, PhA was associated with several known prognostic variables, including serum albumin, but correlation was weak (γ < 0.4, p < 0.001; Spearman correlation test). Detopoulou et al. [40] found significant correlations between PhA and dietary pattern (Food pattern 2) rich in potatoes, meat and poultry (rho = 0.254, p = 0.02). No significant results with PhA and other dietary patterns (food pattern 1: whole grains, fruits, vegetables; food pattern 3: high olive oil, low alcohol; food pattern 4: legumes, fish). Finally, in the same patient’s sample, Mediterranean Diet Score (MedDiet Score) was positively related to PhA changes (rho = 0.251; p = 0.02).
Relationship between PhA, prognostic indices, quality of life and survival
Some of the selected studies evaluated the correlation between PhA and some prognostic indices, QoL scores and survival in patients with LC. Five out of eleven studies indicate patient survival data in relation to the PhA [34, 35, 38, 39, 42]; in two studies, indicators associated with survival were evaluated [34, 35, 38, 39, 42,43,44]. Sanchez-Lara et al. and Shi et al. have evaluated QoL in relation to PhA.
Multifactorial analysis of variance showed correlations between PhA and KPS (r = 0.44; P < 0.05) in cross-sectional study by Castanho et al. [44].
In Hui et al. [45] study, PhA was associated with several known prognostic variables, including the Palliative Performance Scale (γ = 0.18; p = 0.007), KPS (γ = 0.18; p = 0.007), Palliative Prognostic Score (γ = -0.21; p = 0.002), and Palliative Prognostic Index (γ = -0.22; p = 0.001). Unadjusted PhA (P = 0.001) was found to be significantly associated with overall survival, as indicated by Kaplan-Meyer curves analysis: a lower value is associated with poor survival (PhA < 3°, median 35 days; 95% CI, 29–41 days).
Sanchez-Lara et al. [38] evaluated the association of PhA, QoL’s dimensions EORTC QLQ C30 (QLQ-C30) and survival in patients with advanced NSCLC. No significant association between PhA and QoL scores were found. The bivariate survival analysis shows that PhA ≤ 5.8° was significantly associated with low overall survival; multivariate analysis indicate for highest PhA values a higher survival rate (HR = 3.02; 95% CI, 1.2–7.11; p = 0.011).
The results of Spearman’s rank correlation test in Shi et al. [39] showed correlation between PhA and QoL. It was found a L-shaped association between PhA and LC survival in both sexes (men p = 0.019 and women p = 0.121); an association between higher PhA and better survival resulted for men and women (p = 0.007 and p < 0.001, respectively). Kaplan–Meier survival curves for patients with high and low PhA values in different cancer stages showed longer OS in patients with high PhA than patients with low PhA, without taking account stage. Univariate Cox regression analysis showed that continuous PhA was significantly associated with mortality in men with LC (p = 0.015); also in women, PhA was significantly associated with survival (p = 0.029). After adjusting for several covariates, in a multivariate-adjusted Cox regression analysis PhA was identified as an independent risk factor for mortality in men (HR = 0.79, 95% CI = 0.65–0.95, p = 0.015), but not in women (p = 0.105) [39].
In Gupta et al., univariate Kaplan–Meier survival analysis showed statistically significant differences (p = 0.02) between patients with PhA < = 5.3 (median survival = 7.6 months; 95% CI: 4.7 to 9.5; n = 81) and those with > 5.3 (12.4 months; 95% CI: 10.5 to 18.7; n = 84) [34].
No correlation with Charlson Comorbidity Index was found in Suzuki et al. (rho = -0.09; p = 0.16). Also, in this study, multivariate logistic analysis reveals that PhA (OR = 0.51, 95% CI: 0.29–0.90, p = 0.018) was an independent predictor of Clavien-Dindo grade ≥ II, index used for surgical complications [43].
Data from univariate survival analysis of Toso et al., stratified by the cancer stage, indicated that LC patients with a PhA ≤ 4.5° had significantly shorter survival compared to those who have a higher PhA (p = 0.01) (median of 3.7 vs 12.1 months in patients with a PhA ≤ 4.5° vs > 4.5°, respectively, from stage IIIB, and 1.4 vs 5.0 months in in patients with a PhA ≤ 4.5° vs > 4.5, respectively from stage IV) [42].
Relationship between PhA, muscle strength and physical efficiency
Navigante et al. [37] evaluated weakness assessed with Hand-grip strength (HGS). In patients with LC only statistically significant result was linear correlation between grip work and PhA (p = 0.007), which was considered very significant (95% CI: 0.3843 to 0.9717).
In Hui et al., PhA was also associated with HGS, but correlation was not very strong (Spearman’s correlation γ < 0.4; p > 0.001) [35].
Wei Ji et al. have evaluated muscle strength and ASMM to define sarcopenia diagnosis: PhA had strongest correlation with SMI (r = 0.463) and HGS (r = 0.354). Logistic regression analysis adjusted for potential confounders showed that higher PhA values represent a protective factor for sarcopenia (OR 0.309, 95% CI, 0.246 0.617; p < 0.001) [36].
Comparison between different groups and PhA
In the study of Toso et al. were reported differences between healthy subjects, patients with IIIB and IV stages.
Comparing patients with healthy controls was found a reduction in PhA value (resulting in a reduction in capacity, but not R. No significant differences between two groups of patients with IIIB and IV stages were found. However, a significant difference between patients with different stages (statistically lower in patients with higher stages) was observed for survival [42].
In Navigante et al. was carried out a comparison between different groups (healthy volunteers vs patients), but in reference to muscle strength (maximal muscle strength, mean muscle strength, median muscle strength) and not to PhA [37].
In the Hui et al. patients’ cohort (n = 204) with different types of cancer (including breast, gastrointestinal, head and neck and gynaecological) two different groups have been distinguished: patients with edema and without edema. Univariate analysis showed a reduced survival for PhA ≤ 3° vs PhA > 3° for total patients (p = 0.045) and no edema patients (p < 0.001). PhA ≤ 3° was associated with shorter survival in the non-oedematous cohort (HR 4.42, 95% CI 2.09–9.36, p < 0.001), but this association did not occur in the whole cohort (HR 1.44, 95% CI 0.99–2.09, p = 0.054) and in the cohort with edema (HR 1.04, 95% CI 0.67–1, 62, p = 0.85) (Cox regression analysis) [35].
Wei Ji et al. evaluated the association between PhA in older male patients with different types of malignancies, with sarcopenia (22.0%) and without. PhA in patients without sarcopenia was 5.02° (SD ± 0.72°), while in sarcopenic was 4.18° (SD ± 0.85°); this difference was statistically significative (p < 0.001) [36].
Discussion
The present review aims to investigate the current data regarding PhA in LC patients. We did not find a large number of studies focused on the assessment of PhA, which made it difficult to reach a comprehensive conclusion on this topic. We found 11 studies evaluating the PhA value obtained from BIA in patients with LC. In order to choose the right cancer treatment and plan carefully, survival prediction is crucial. In any case, new tools are necessary to be applied in daily clinical practice.
In the latest years, a growing body of studies have evaluated the prognostic role of PhA not only in patients with LC, but also in patients with respiratory disease. Indeed, De Benedetto et al. reported that lower PhA is associated with a decreased muscle mass, muscle strength and exercise capacity in patients with idiopathic pulmonary fibrosis, regardless of body weight. Moreover, patients with Chronic Obstructive Pulmonary Disease (COPD) and lower PhA have reduced cell mass, evident skeletal muscle depletion, worsening gas exchange and an increased risk of all-cause mortality [46]. Similarly, a lower PhA has been associated with an increased risk of malnutrition, sarcopenia, fluid retention, systemic inflammation, symptoms, and poorer QoLin patients with cancer. Moreover, a lower PhA may be a novel prognostic factor of poorer overall survival and higher risk of postoperative complications in cancer patients [47].
Overall, lower PhA levels have been associated with poorer physical condition and shorter survival in patients with LC: in Sanchez-Lara et al. [38], Gupta et al. [30,31,32, 34, 48] and Toso et al. [42] LC patients with lower PhA had a shorter survival than patients with higher PhA. In addition, in Shi et al. [39] patients with a higher PhA had a better survival and PhA was an independent risk factor for mortality in men with LC. Navigante et al. [37] in cancer patients without edema, PhA values ≤ 3° were associated with mortality within three days of BIA analysis, while in sarcopenic patients the PhA value was reduced compared to non-sarcopenic patients.
Patients with a lower PhA also had a higher risk of complications after surgical procedures [36]. In the prospective observational study of Uccella et al., it was observed that PhA was an independent prognostic factor of optimal cytoreduction and postoperative complications among patients with primary diagnosis of advanced ovarian cancer [49]. Similarly, in the prospective observational study of Inci et al. (The Risk-Gin trial) the authors observed that patients undergoing surgery for gynecological cancer with PhA < 4.75° and HGS < 44 kg in both hands had a three-fold increased risk of 30 days severe postoperative complications [50].
Thus, in addition to being a marker of cellular function, muscle mass and nutritional status, PhA may be a predictive factor of acute catastrophic complications risk. Interestingly, PhA was weakly but significantly associated with other prognostic variables, suggesting that it captures some additional information compared to existing prognostic factors. Further studies are needed to examine physiological and cellular changes associated with PhA.
Gupta et al. have evaluated role of PhA in the prognosis of 52 patients with advanced colorectal cancer: patients with PhA ≤ 5.7º had an 8-months average survival rate (Kaplan–Meier method), while those with PhA > 5.57º had a 40-month average survival rate [32]. Bosy-Westphal et al. [51] showed that patients with PhA < the fifth percentile had a deterioration in nutritional and functional status, decreased QoL and increased morbidity and mortality. The fifth percentile was a clinically relevant indicator of cancer cachexia. In this context, Hui et al. [35]investigated the association between PhA and survival in individuals with terminal cancer, where the increment of 1 degree in PhA was associated with higher survival rates.
In the prospective observational study by Paiva et al. PhA is reported as an independent prognostic factor, and Norman et al. [52]showed that in cancer patients, PhA values (stratified by age, sex, and BMI) below the fifth percentile of reference corresponded to a significant deterioration in nutritional status. In addition, these patients showed decreased HGS, increased incidence of weight loss, dyspnoea, fatigue, and increased risk of mortality. In three articles positive correlation has emerged between HGS and PhA, so weakness is related to the reduction in PhA in cancer patients. In other patient’s populations, it was shown that impaired muscle strength was associated with a poorer prognosis [53, 54]. In addition, correlations between HGS, PhA and other BIA variables have emerged in adolescents and young adults [55].
In Navigante et al. [37], univariate logistic regression analysis showed that higher PhA values represent a protective factor for sarcopenia. In Pérez-Camargo et al. [56] palliative care patients with cancer (the most frequently were gastric cancer, gynecological cancer, LC, and haematological malignancies) and severe sarcopenia had a lower mean PhA (3.9°) compared to patients without sarcopenia (mean PhA was 4.1°) showing that PhA is an independent measurement that can be associated to detect sarcopenia. Moreover, authors found that sarcopenic patients had a shorter overall survival and an increased risk of death compared to patients without sarcopenia. A recent review [57] indicated that PhA and sarcopenia are related to LC prognosis through different mechanisms including inflammation and oxidative stress. Detection of sarcopenia and the evaluation of BC and PhA can be a valuable tool for identifying and timely intervention of the state of malnutrition of the cancer patient. Timely analysis of patient’s nutritional status is essential, as it allows to avoid significant loss of cell mass and lean mass, but ensures a proper nutritional approach in order to avoid aggravation of the general condition of the patient. Moreover, to obtain an accurate clinical interpretation of PhA, simultaneous assessment of hydration and BCM status is required [58]. These informations could be derived from the analysis of vector length on the R/Xc plot using Bioelectrical Impedance Vectorial Analysis (BIVA) (a scatterplot that represents R in X-axis and Xc in Y-axis divided by height in meters). In healthy subjects, a balance is observed between BCM and hydration status of FFM: malnutrition, sarcopenia and cachexia can lead to a loss of BCM and cell membrane surface area, provoking cell damage and a reduction in PhA [58].
According to the American Cancer Society (ACS), one of the first hallmarks of several types of cancer, including LC, is unexplained weight loss. In addition, treatments such as RT and CHT could generate side effects that cause inappetence to patients (e.g., mouth ulcers, nausea, vomiting). Tumour growth leading to extreme loss of appetite and weight in association with systemic signs of inflammation may be breeding grounds for cachexia [59]. Cachexia leads to a considerable loss of skeletal muscle mass (SMM) that cannot be completely compensated with traditional nutritional supports. Furthermore, it may be an underlying condition in patients with sarcopenia. We know that malnutrition and cachexia are often present in cancer patients [13]: this state can worsen the effects of anticancer therapies, with premature discontinuation of treatment, patient's QoL decreased and higher risk of mortality [60, 61]. Nutritional status in cancer patients, especially the elderly, should be evaluated before and during CHT [61]. However, evaluation and detection of malnutrition status is not simple and instantaneous in patients. Therefore, it is preferable and useful to use the different variables defined by the BIA, to evaluate the changes in cellular membrane and body water levels. Future research on the use of PhA in clinical practice will be valuable in establishing cut-off values to better categorize oncology patients [58].
Limitations
To our knowledge, this is the most recent review focusing on the assessment of BIA-derived PhA in LC patients, however, we had to consider several limitations. Although several search engines outside PubMed were used, the review included only 11 studies of which only 8 were aimed at analysing PhA exclusively on patients with LC. Only four studies related to this topic were published in 2022, the other articles we included in our work were published between 2000 and 2013, so we do not have a large number of recent evidence.
Finally, accurate data on PhA relationships and other variables such as anthropometric values, HGS test, ECM/BCM ratio, tumour stage, tumour volume, etc., are absolutely necessary for a broader understanding of how PhA can be beneficial for this population. No information about PhA timing measurement by bioimpedance were provided in selected studies Monitoring the health of these patients is very important in order to be able to act promptly with targeted integrated therapies involving nutrition and physical activity, so further studies are needed. Patients with LC are at greater risk of malnutrition, sarcopenia and cachexia, with implications for physical function and overall QoL. Therefore, before making an assessment of the BC and PhA, it would be useful to consider the stage of the disease, cancer therapies carried out and the side effects, comorbidities and possible states of inflammation. All measurement should be performed in standard conditions and, in these specific cases, in days that do not correspond with cancer therapy. Patients with chronic respiratory disease could experience dysfunction in skeletal muscle mass (SMM) and BC changes as consequence of smoking, alcohol abuse, systemic inflammation, systemic oxidative stress, hormonal deficiencies, comorbidities, aging, and inappropriate diet [46, 47]. Moreover, fat-free mass depletion and decreased muscle strength are common features of these patients. In this context, usefulness of PhA as a health status marker was investigated by a growing body of study. Similarly, patients with cancer patients have multiple comorbidities (chronic kidney disease) which may impact BC and cellular function. Moreover, patients with cancer frequently have fluid retention including edema, ascites, and pleural effusions. These factors may complicate the interpretation of PhA because this parameter is affected by altered ECW/ICW, or fluid disruption. Therefore, given the few studies currently available and the high number of factors that can affect BC measurements (hydration status, concomitant intake of food, alcohol use, physical activity, menstrual cycle, use of specific drugs that increase cell retention and catabolism, etc.) it should maintain accurate standardization in measurement.
Conclusions
The evaluation of PhA by BIA analysis in LC patients is not widely discussed in scientific literature. However, early identification in nutritional status changes in cancer patients represents a crucial aspect to improve patient’s quality of life both post-diagnosis and during and after anticancer therapies, avoiding possible states of malnutrition and sarcopenia, which can aggravate patient’s status. This systematic review shows an association between a very low PhA and an increased risk of a deficent physical condition, linked to reduced survival in lung cancer patients. In the selected studies, various cut-offs point for PhA have been reported that need to be interpreted with caution: to date, it is not possible to define a single threshold or cut off point for PhA due to technical differences in commercial BIA devices (single-, multiple-frequency and BIS). Given the high incidence of this cancer and the low number of studies on this issue, it would be important and necessary to make greater use of this screening method in clinical practice.
Availability of data and materials
All the data analysed for this review are present in the tables; there are no additional files.
Abbreviations
- ACS:
-
American Cancer Society
- ASMM:
-
Appendicular Skeletal Muscle Mass
- BC:
-
Body composition
- BCM :
-
Body Cellular Mass
- BIA:
-
Bioelectrical Impedance Analysis
- BIVA:
-
Bioelectrical Impedance Vectorial Analysis
- BMI:
-
Body Mass Index
- CC:
-
Calf Circumference
- CHT:
-
Chemotherapy
- COPD:
-
Chronic Obstructive Pulmonary Disease
- ECM:
-
Extra-cellular Mass
- ECW:
-
Extra-cellular Water
- FFM:
-
Fat-Free Mass
- FFMI:
-
Fat-Free Mass index
- FM:
-
Fat Mass
- HGS:
-
Hand-grip strength
- HRQoL:
-
Health Related Quality of Life
- ICI:
-
Immune checkpoint inhibitor
- ICW:
-
Intra-Cellular Water
- KPS:
-
Karnofski Performance Status
- LC :
-
Lung Cancer
- MDS:
-
Mediterranean Dietary Score
- MF-BIA:
-
Multiple-frequency Bioelectrical Impedance Analysis
- NRS-2002:
-
Nutritional Risk Score-2002
- NSCLC:
-
Non-small cell lung carcinoma
- OS:
-
Overall Survival
- PhA:
-
Phase Angle
- PG-SGA :
-
Patient-Generated Subjective Global Assessment
- PNI:
-
Prognostic Nutritional Index
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QLQ – C30:
-
Quality of Life Questionnaire – Cancer 30
- QoL :
-
Quality of Life
- R:
-
Resistance
- RT:
-
Radiotherapy
- SCLC:
-
Small cell lung carcinoma
- SF-BIA :
-
Single-frequency Bioelectrical Impedance Analysis
- SMI:
-
Skeletal Muscle Mass Index
- SMM:
-
Skeletal Muscle Mass
- TLC :
-
Total Lymphocyte Count
- TBW:
-
Total Body Water
- Xc:
-
Reactance
- Z:
-
Impedance
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49.
I Numeri del Cancro in Italia 2022 [https://www.aiom.it/i-numeri-del-cancro-in-italia/].
Zhang P, Chen PL, Li ZH, Zhang A, Zhang XR, Zhang YJ, Liu D, Mao C. Association of smoking and polygenic risk with the incidence of lung cancer: a prospective cohort study. Br J Cancer. 2022;126(11):1637–46.
Kim CH, Lee YC, Hung RJ, McNallan SR, Cote ML, Lim WY, Chang SC, Kim JH, Ugolini D, Chen Y, et al. Exposure to secondhand tobacco smoke and lung cancer by histological type: a pooled analysis of the International Lung Cancer Consortium (ILCCO). Int J Cancer. 2014;135(8):1918–30.
Luo J, Hendryx M, Ducatman A. Association between six environmental chemicals and lung cancer incidence in the United States. J Environ Public Health. 2011;2011: 463701.
Zheng M. Classification and Pathology of Lung Cancer. Surg Oncol Clin N Am. 2016;25(3):447–68.
Mele MC, Rinninella E, Cintoni M, Pulcini G, Di Donato A, Grassi F, Trestini I, Pozzo C, Tortora G, Gasbarrini A, et al. Nutritional support in lung cancer patients: the state of the art. Clin Lung Cancer. 2021;22(4):e584–94.
Beckles MA, Spiro SG, Colice GL, Rudd RM. Initial evaluation of the patient with lung cancer: symptoms, signs, laboratory tests, and paraneoplastic syndromes. Chest. 2003;123(1 Suppl):97S–104S.
Polanski J, Jankowska-Polanska B, Rosinczuk J, Chabowski M, Szymanska-Chabowska A. Quality of life of patients with lung cancer. Onco Targets Ther. 2016;9:1023–8.
Arends J, Baracos V, Bertz H, Bozzetti F, Calder PC, Deutz NEP, Erickson N, Laviano A, Lisanti MP, Lobo DN, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187–96.
Porro C, La Torre ME, Tartaglia N, Benameur T, Santini M, Ambrosi A, Messina G, Cibelli G, Fiorelli A, Polito R, et al. The potential role of nutrition in lung cancer establishment and progression. Life (Basel). 2022;12(2):270.
Pilikidou M, Palyvou F, Papadopoulou SK, Tsiouda T, Tsekitsidi E, Arvaniti K, Miziou A, Tsingerlioti Z, Apostolidis G, Ntiloudis R, et al. Lung cancer, treatment and nutritional status. Mol Clin Oncol. 2021;15(6):248.
Dewys WD, Begg C, Lavin PT, Band PR, Bennett JM, Bertino JR, Cohen MH, Douglass HO, Jr., Engstrom PF, Ezdinli EZ et al.: Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med 1980, 69(4):491–497.
Ravasco P, Monteiro-Grillo I, Vidal PM, Camilo ME. Nutritional deterioration in cancer: the role of disease and diet. Clin Oncol (R Coll Radiol). 2003;15(8):443–50.
Prado CM, Lieffers JR, Bowthorpe L, Baracos VE, Mourtzakis M, McCargar LJ. Sarcopenia and physical function in overweight patients with advanced cancer. Can J Diet Pract Res. 2013;74(2):69–74.
Fortunati N, Manti R, Birocco N, Pugliese M, Brignardello E, Ciuffreda L, Catalano MG, Aragno M, Boccuzzi G. Pro-inflammatory cytokines and oxidative stress/antioxidant parameters characterize the bio-humoral profile of early cachexia in lung cancer patients. Oncol Rep. 2007;18(6):1521–7.
Duguet A, Bachmann P, Lallemand Y, Blanc-Vincent MP. Good clinical practice in nutritional management in cancer patients: malnutrition and nutritional assessment. Bull Cancer. 1999;86(12):997–1016.
Polanski J, Chabowski M, Swiatoniowska-Lonc N, Dudek K, Jankowska-Polanska B, Zabierowski J, Mazur G: Relationship between Nutritional Status and Clinical Outcome in Patients Treated for Lung Cancer. Nutrients 2021;13(10):3332.
Lin TY, Chen YF, Wu WT, Han DS, Tsai IC, Chang KV, Ozcakar L. Impact of sarcopenia on the prognosis and treatment of lung cancer: an umbrella review. Discov Oncol. 2022;13(1):115.
Bapuji SB, Sawatzky JA. Understanding weight loss in patients with colorectal cancer: a human response to illness. Oncol Nurs Forum. 2010;37(3):303–10.
Argiles JM, Lopez-Soriano FJ, Busquets S. Mechanisms and treatment of cancer cachexia. Nutr Metab Cardiovasc Dis. 2013;23(Suppl 1):S19–24.
Wang J, Tan S, Gianotti L, Wu G. Evaluation and management of body composition changes in cancer patients. Nutrition. 2023;114:112132.
Yamada Y, Buehring B, Krueger D, Anderson RM, Schoeller DA, Binkley N. Electrical Properties Assessed by Bioelectrical Impedance Spectroscopy as Biomarkers of Age-related Loss of Skeletal Muscle Quantity and Quality. J Gerontol A Biol Sci Med Sci. 2017;72(9):1180–6.
Barbosa-Silva MC, Barros AJ. Bioelectrical impedance analysis in clinical practice: a new perspective on its use beyond body composition equations. Curr Opin Clin Nutr Metab Care. 2005;8(3):311–7.
Almada-Correia I, Neves PM, Makitie A, Ravasco P. Body Composition Evaluation in Head and Neck Cancer Patients: A Review. Front Oncol. 2019;9:1112.
Branco MG, Mateus C, Capelas ML, Pimenta N, Santos T, Makitie A, Ganhao-Arranhado S, Trabulo C, Ravasco P: Bioelectrical Impedance Analysis (BIA) for the Assessment of Body Composition in Oncology: A Scoping Review. Nutrients 2023, 15(22):792.
Caccialanza R, Cotogni P, Cereda E, Bossi P, Aprile G, Delrio P, Gnagnarella P, Mascheroni A, Monge T, Corradi E, et al. Nutritional support in cancer patients: update of the Italian Intersociety Working Group practical recommendations. J Cancer. 2022;13(9):2705–16.
Shintani Y, Ikeda N, Matsumoto T, Kadota Y, Okumura M, Ohno Y, Ohta M. Nutritional status of patients undergoing chemoradiotherapy for lung cancer. Asian Cardiovasc Thorac Ann. 2012;20(2):172–6.
Marin Caro MM, Laviano A, Pichard C. Nutritional intervention and quality of life in adult oncology patients. Clin Nutr. 2007;26(3):289–301.
Gupta D, Lis CG, Dahlk SL, Vashi PG, Grutsch JF, Lammersfeld CA. Bioelectrical impedance phase angle as a prognostic indicator in advanced pancreatic cancer. Br J Nutr. 2004;92(6):957–62.
Gupta D, Lammersfeld CA, Vashi PG, King J, Dahlk SL, Grutsch JF, Lis CG. Bioelectrical impedance phase angle as a prognostic indicator in breast cancer. BMC Cancer. 2008;8:249.
Gupta D, Lammersfeld CA, Burrows JL, Dahlk SL, Vashi PG, Grutsch JF, Hoffman S, Lis CG. Bioelectrical impedance phase angle in clinical practice: implications for prognosis in advanced colorectal cancer. Am J Clin Nutr. 2004;80(6):1634–8.
Grundmann O, Yoon SL, Williams JJ. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients–a comprehensive review. Eur J Clin Nutr. 2015;69(12):1290–7.
Gupta D, Lammersfeld CA, Vashi PG, King J, Dahlk SL, Grutsch JF, Lis CG. Bioelectrical impedance phase angle in clinical practice: implications for prognosis in stage IIIB and IV non-small cell lung cancer. BMC Cancer. 2009;9:37.
Hui D, Bansal S, Morgado M, Dev R, Chisholm G, Bruera E. Phase angle for prognostication of survival in patients with advanced cancer: preliminary findings. Cancer. 2014;120(14):2207–14.
Ji W, Liu X, Zheng K, Yang H, Cui J, Li W. Correlation of phase angle with sarcopenia and its diagnostic value in elderly men with cancer. Nutrition. 2021;84:111110.
Navigante A, Morgado PC, Casbarien O, Delgado NL, Giglio R, Perman M. Relationship between weakness and phase angle in advanced cancer patients with fatigue. Support Care Cancer. 2013;21(6):1685–90.
Sanchez-Lara K, Turcott JG, Juarez E, Guevara P, Nunez-Valencia C, Onate-Ocana LF, Flores D, Arrieta O. Association of nutrition parameters including bioelectrical impedance and systemic inflammatory response with quality of life and prognosis in patients with advanced non-small-cell lung cancer: a prospective study. Nutr Cancer. 2012;64(4):526–34.
Shi J, Xie H, Ruan G, Ge Y, Lin S, Zhang H, Zheng X, Liu C, Song M, Liu T, et al. Sex differences in the association of phase angle and lung cancer mortality. Front Nutr. 2022;9:1061996.
Detopoulou P, Tsiouda T, Pilikidou M, Palyvou F, Mantzorou M, Perzirkianidou P, Kyrka K, Methenitis S, Kondyli FS, Voulgaridou G, et al. Dietary habits are related to phase angle in male patients with non-small-cell lung cancer. Curr Oncol. 2022;29(11):8074–83.
Detopoulou P, Tsiouda T, Pilikidou M, Palyvou F, Tsekitsidi E, Mantzorou M, Pezirkianidou P, Kyrka K, Methenitis S, Voulgaridou G et al: Changes in Body Weight, Body Composition, Phase Angle, and Resting Metabolic Rate in Male Patients with Stage IV Non-Small-Cell Lung Cancer Undergoing Therapy. Medicina (Kaunas) 2022;58(12):1779.
Toso S, Piccoli A, Gusella M, Menon D, Bononi A, Crepaldi G, Ferrazzi E. Altered tissue electric properties in lung cancer patients as detected by bioelectric impedance vector analysis. Nutrition. 2000;16(2):120–4.
Suzuki Y, Kushimoto Y, Ishizawa H, Kawai H, Ito A, Matsuda Y, Hoshikawa Y. The phase angle as a predictor of postoperative complications in patients undergoing lung cancer surgery. Surg Today. 2023;53(3):332–7.
Castanho IA, Lopes AJ, Koury JC, Tessarollo B, Silva AC, Nunes RA. Relationship between the phase angle and volume of tumours in patients with lung cancer. Ann Nutr Metab. 2013;62(1):68–74.
Hui D, Moore J, Park M, Liu D, Bruera E. Phase Angle and the Diagnosis of Impending Death in Patients with Advanced Cancer: Preliminary Findings. Oncologist. 2019;24(6):e365–73.
De Benedetto F, Marinari S, De Blasio F. Phase angle in assessment and monitoring treatment of individuals with respiratory disease. Rev Endocr Metab Disord. 2023;24(3):491–502.
Amano K, Bruera E, Hui D. Diagnostic and prognostic utility of phase angle in patients with cancer. Rev Endocr Metab Disord. 2023;24(3):479–89.
Naughton MJ, Weaver KE. Physical and mental health among cancer survivors: considerations for long-term care and quality of life. N C Med J. 2014;75(4):283–6.
Uccella S, Mele MC, Quagliozzi L, Rinninella E, Nero C, Cappuccio S, Cintoni M, Gasbarrini A, Scambia G, Fagotti A. Assessment of preoperative nutritional status using BIA-derived phase angle (PhA) in patients with advanced ovarian cancer: Correlation with the extent of cytoreduction and complications. Gynecol Oncol. 2018;149(2):263–9.
Inci MG, Richter R, Woopen H, Rasch J, Heise K, Anders L, Mueller K, Nasser S, Siepmann T, Sehouli J. Role of predictive markers for severe postoperative complications in gynecological cancer surgery: a prospective study (RISC-Gyn Trial). Int J Gynecol Cancer. 2020;30(12):1975–82.
Bosy-Westphal A, Danielzik S, Dorhofer RP, Later W, Wiese S, Muller MJ. Phase angle from bioelectrical impedance analysis: population reference values by age, sex, and body mass index. JPEN J Parenter Enteral Nutr. 2006;30(4):309–16.
Norman K, Stobaus N, Pirlich M, Bosy-Westphal A. Bioelectrical phase angle and impedance vector analysis–clinical relevance and applicability of impedance parameters. Clin Nutr. 2012;31(6):854–61.
Hodgev VA, Kostianev SS. Maximal inspiratory pressure predicts mortality in patients with chronic obstructive pulmonary disease in a five-year follow-up. Folia Med (Plovdiv). 2006;48(3–4):36–41.
Cooper R, Kuh D, Hardy R, Mortality Review G. Falcon, Teams HAS: Objectively measured physical capability levels and mortality: systematic review and meta-analysis. BMJ. 2010;341: c4467.
Sacco AM, Valerio G, Alicante P, Di Gregorio A, Spera R, Ballarin G, Scalfi L. Raw bioelectrical impedance analysis variables (phase angle and impedance ratio) are significant predictors of hand grip strength in adolescents and young adults. Nutrition. 2021;91–92: 111445.
Perez Camargo DA, Allende Perez SR, Verastegui Aviles E, Rivera Franco MM, Meneses Garcia A, Herrera Gomez A, Urbalejo Ceniceros VI. Assessment and impact of phase angle and sarcopenia in palliative cancer patients. Nutr Cancer. 2017;69(8):1227–33.
Detopoulou P, Voulgaridou G, Papadopoulou S. Cancer, Phase Angle and Sarcopenia: The Role of Diet in Connection with Lung Cancer Prognosis. Lung. 2022;200(3):347–79.
Bellido D, Garcia-Garcia C, Talluri A, Lukaski HC, Garcia-Almeida JM. Future lines of research on phase angle: Strengths and limitations. Rev Endocr Metab Disord. 2023;24(3):563–83.
Blauwhoff-Buskermolen S, Versteeg KS, de van der Schueren MA, den Braver NR, Berkhof J, Langius JA, Verheul HM. Loss of Muscle Mass During Chemotherapy Is Predictive for Poor Survival of Patients With Metastatic Colorectal Cancer. J Clin Oncol 2016;34(12):1339-1344.
Aapro M, Arends J, Bozzetti F, Fearon K, Grunberg SM, Herrstedt J, Hopkinson J, Jacquelin-Ravel N, Jatoi A, Kaasa S, et al. Early recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Ann Oncol. 2014;25(8):1492–9.
Caillet P, Liuu E, Raynaud Simon A, Bonnefoy M, Guerin O, Berrut G, Lesourd B, Jeandel C, Ferry M, Rolland Y, et al. Association between cachexia, chemotherapy and outcomes in older cancer patients: A systematic review. Clin Nutr. 2017;36(6):1473–82.
Funding
This research was funded by Ministry of Health (5X1000_2021_2).
Author information
Authors and Affiliations
Contributions
M.P., G.B. and L.S. have proposed, designed and edited data analysis of this systematic review; M.P. and G.P. wrote the main manuscript text and prepared Fig. 1 and Tables 1 and 2. All work was supervised by E.C and L.S. All authors have read and revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Prete, M., Ballarin, G., Porciello, G. et al. Bioelectrical impedance analysis—derived phase angle (PhA) in lung cancer patients: a systematic review. BMC Cancer 24, 608 (2024). https://doi.org/10.1186/s12885-024-12378-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12378-4