
Abstract
Background
The pathogenesis of macular hole formation is widely accepted as a tractional force at the vitreo-retinal interface in fovea. We report a case of macular hole after intravitreous aflibercept injection for age-related macular degeneration (AMD) associated with contraction of the retinal pigment epithelium (RPE) at the edge of a fibrovascular pigment epithelial detachment (PED).
Case presentation
A 94-year old man with neovascular AMD affecting his left eye accompanied by a fibrovascular PED was examined for severe vision loss. Although RPE tear in his left eye was identified before the first aflibercept intravitreous injection performed in order to treat neovascular AMD, he received three aflibercept injections as induction treatment. After induction treatment, a full thickness macular hole was identified associated with the contracted rolled RPE edge beneath the retina.
Conclusion
Macular hole is commonly formed associated with tangential vitreous traction. Current report suggests that rapid contraction of the RPE underneath the retina can be one of the causes of a macular hole, and one of the side effects of anti-VEGF therapy for neovascular AMD.
Similar content being viewed by others


Background
Neovascular Age-Related Macular Degeneration (wet AMD) is the major cause of legal blindness among the elderly people in many countries. Anti-vascular endothelial growth factor (VEGF) therapy is now the major treatment in order to prevent severe vision loss and possibly improve vision. Tears of the retinal pigment epithelium (RPE) are recognized as complication of wet AMD in patients with pigment epithelial detachments (PED) [1]. Although several recent reports indicated that anti-VEGF antagonists, such as pegaptanib, bevacizumab, and ranibizumab might increase the risk of tears of RPE compared to natural course [2-5]. Cunningham et al. reported that there aren’t significantly differences of the incident of RPE tear after ranibizumab treatment for wet AMD patients in ANCHOR, MARINA, and PIER study compared to natural course [6]. Idiopathic macular holes are full-thickness retinal defects in the foveal neurosensory retina. The pathogenesis of macular hole formation is widely accepted as an abnormal anteroposterior and tangential vitreous traction performed in foveal retinal surface [7]. We present a recent case of macular hole after intravitreous aflibercept injection associated with contraction of the RPE at the edge of a PED.
Case presentation
A 94-year-old man presented with sudden visual disturbance of his left eye. At the first visit, the best corrected visual acuity (BCVA) in the right eye was 0.046 log MAR and in the left eye was 1.7 log MAR. The axial length of the right eye was 23.46 mm, and that of left eye was 23.47 mm. Fundus examination showed multiple drusen in the right eye, and subretinal bleeding and vascularized PED associated with wet AMD in the left eye. Fluorescein (FA) and Indocyanine (IA) angiography showed occult with no classic choroidal neovascularization (CNV) in the fovea and an RPE tear at the edge of PED. OCT showed a large PED and serous neurosensory retinal detachment. (Figure 1) After the first aflibercept intravitreous treatment, tear of the RPE and rolled RPE were clearly noted beneath the retina. OCT showed thinning of the central retina in the center of fovea stretched by the rolled and contracted RPE that was exacerbated after the second aflibercept injection. After the third injection performed as part of the induction treatment, the BCVA in the left eye was 1.7 log MAR, and full thickness macular hole formed due to stretched by rolled RPE contraction. (Figure 2) Observation was recommended because the patient did not desire any additional intervention. One year after first aflibercept treatment, fundus examination showed subretinal fibrosis, and full thickness macular hole remained open. The BCVA in the left eye was 1.7 log MAR, same as that seen at baseline.

Macular findings before treatment. A 94-year-old man was treated with intravitreal aflibercept injection. At baseline, the best-corrected visual acuity was 1.7 log MAR. (A) Color fundus photograph shows subretinal hemorrhage, serous retinal detachment (SRD), and pigment epithelial detachment (PED). (B) Fluorescein angiography image showing leakage due to occult CNV and staining due to vascularized PED, and hyperfluorescence due to RPE tear. (C) Indocyanine green angiography image shows no underlying polypoidal lesion. (D) Optical coherence tomography (OCT) image showing PED and SRD.

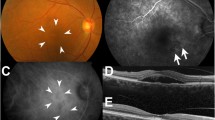
The progression findings for macular hole formation. (A,C) One month after first aflibercept injection. The color fundus photograph shows a tear of the RPE, rolled RPE flap beneath the retina, and subretinal fibrosis. OCT shows rolled RPE flap and SRD. (B,D) One month after second aflibercept injection. The color fundus photograph shows contracted subretinal fibrosis. OCT shows thin foveal retina secondary to traction associated with the rolled RPE flap. (E, F,G, H) One month after third aflibercept injection. The color fundus photograph shows contracted subretinal fibrosis and RPE tear (E). Fluorescein angiography shows choroidal flush due to a macular hole (F). Indocyanine green angiography shows blocked fluorescence due to subretinal fibrosis (G). OCT shows full thickness macular hole with shrunken, rolled RPE flap (H). Arrows show the edge of rolled RPE flap (A, B, E).
Discussion
RPE tear is well known as the complication of wet AMD, especially common in the patients with PED [8]. Although some reports suggested that anti-VEGF therapy might increase the risk of RPE tear as a complication of wet AMD treatment, subanalysis report of large scale prospective study revealed that the incidence of RPE tear after ranibizumab treatment is not significantly higher compared to natural course [6]. Tear of RPE as a complication has been reported with each different anti-VEGF agent, including bevacizumab, ranibizumab, pegaptanib, and aflibercept [2-4,9]. A recent retrospective study showed that the risk of RPE tear is significantly higher in patients with vascularized PED (vPED) than without PED, and shorter duration of PED and higher PED are significant risk factors [5]. The exact pathogenesis of RPE tear is unknown. But a recent report speculated that rapid involution and contraction of neovascular tissue adherent to the undersurface of the RPE may impart a substantial contractile force to tears [10]. The pathogenesis of macular hole formation is widely associated with anteroposterior vitreo-macular traction [11]. Although macular hole formation associated with AMD is rare, there have been reports AMD-associated macular hole development [12-15]. Okamoto et al. reported that traction of epiretinal membrane caused by exudative changes derived from CNV is supposed to be one of the reason for macular hole formation accompanied by AMD [14]. Raiji et al. reported full thickness macular hole formation overlying PED after intravitreous ranibizumab injection. They speculated the etiology as the tractional forces of vitreomacular adhesion and pushing or stretching forces of the choroidal neovascular complex may contribute to macular hole formation [15].
In this case, the patient received aflibercept injections for his wet AMD with vascularized PED. Tear of RPE at the edge of the PED occurred before the first injection and the rolled RPE flap involuted underneath the retina. Rolled RPE flap associated with subretinal fibrosis resulted in traction on the fovea from underneath the retina during aflibercept treatment. The contracted fovea above and beneath retina was split and there was progression to a full thickness macular hole. He didn’t receive surgical procedure for closing macular hole, because the macular hole was over an area devoid of RPE due to the RPE tear and that surgical closure of the hole would not likely lead to improvement in vision. His BCVA remained stable during further observation.
To our knowledge, this is the first case report of macular hole formation secondary to an RPE tear and contraction of the RPE edge and subretinal fibrosis following multiple intravitreal aflibercept injections. Although the incidence of full thickness macular hole formation, as a complication after anti-VEGF therapy is low, one should be mindful of such complications associated with anti-VEGF injections.
Conclusion
Macular hole is commonly formed associated with tangential vitreous traction in the fovea. Current report suggests that rapid contraction of the RPE underneath the retina can be one of the causes of a macular hole, and one of the side effects of anti-VEGF therapy for neovascular AMD.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal.
Abbreviations
- AMD:
-
Age-related macular degeneration
- CNV:
-
Choroidal neovascularization
- FA:
-
Fluorescein angiogram
- IA:
-
Indocyanine green angiogram
- RPE:
-
Retinal pigment epithelium
- PED:
-
Pigment epithelial detachments
References
Chang LK, Sarraf D. Tears of the retinal pigment epithelium: an old problem in a new era. Retina. 2007;27:523–34.
Shah CP, Hsu J, Garg SJ, Fischer DH, Kaiser R. Retinal pigment epithelial tear after intravitreal bevacizumab injection. Am J Ophthalmol. 2006;142:1070–2.
Guber J, Praveen A, Saeed MU. Higher incidence of retinal pigment epithelium tears after ranibizumab in neovascular age-related macular degeneration with increasing pigment epithelium detachment height. Br J Ophthalmol. 2013;97:1486–7.
Chang LK, Flaxel CJ, Lauer AK, Sarraf D. RPE tears after pegaptanib treatment in age-related macular degeneration. Retina. 2007;27:857–63.
Doguizi S, Ozdek S. Pigment epithelial tears associated with Anti-Vegf therapy: incidence, long-term visual outcome, and relationship with pigment epithelial detachment in Age-related Macular Degeneration. Retina. 2014;34:1156–62.
Cunningham ET, Feiner L, Chung C, Tuomi L, Ehrlich JS. Incidence of retinal pigment epithelial tears after intravitreal ranibizumab injection for neovascular age-related macular degeneration. Ophthalmology. 2011;118:2447–52.
Smiddy WE, Flynn HW. Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004;137:525–37.
Pauleikhoff D, Löffert D, Spital G, Radermacher M, Dohrmann J, Lommatzsch A, et al. Pigment epithelial detachment in the elderly. Clinical differentiation, natural course and pathogenetic implications. Graefes Arch Clin Exp Ophthalmol. 2002;240:533–8.
Saito M, Kano M, Itagaki K, Oguchi Y, Sekiryu T. Retinal pigment epithelium tear after intravitreal aflibercept injection. Clin Ophthalmol. 2013;7:1287–9.
Nagiel A, Freund KB, Spaide RF, Munch IC, Larsen M, Sarraf D. Mechanism of retinal pigment epithelium tear formation following intravitreal anti-vascular endothelial growth factor therapy revealed by spectral-domain optical coherence tomography. Am J Ophthalmol. 2013;156:981–8. e2.
Steel DHW, Lotery AJ. Idiopathic vitreomacular traction and macular hole: a comprehensive review of pathophysiology, diagnosis, and treatment. Eye (Lond). 2013;27 Suppl 1:S1–21.
Grigoropoulos V, Emfietzoglou J, Nikolaidis P, Theodossiadis G, Theodossiadis P. Full-thickness macular hole after intravitreal injection of ranibizumab in a patient with retinal pigment epithelium detachment and tear. Eur J Ophthalmol. 2010;20:469–72.
Moisseiev E, Goldstein M, Loewenstein A, Moisseiev J. Macular Hole following Intravitreal Bevacizumab Injection in Choroidal Neovascularization Caused by Age-Related Macular Degeneration. Case Rep Ophthalmol. 2010;1:36–41.
Okamoto T, Shinoda H, Kurihara T, Nagai N, Tsubota K, Ozawa Y. Intraoperative and fluorescein angiographic findings of a secondary macular hole associated with age-related macular degeneration treated by pars plana vitrectomy. BMC Ophthalmol. 2014;14:114.
Raiji VR, Eliott D, Sadda SR. Macular hole overlying pigment epithelial detachment after intravitreal injection with ranibizumab. Retin Cases Brief Rep. 2013;7:91–4.
Acknowledgments
This work was supported in part by JSPS KAKENHI Grant # Kiban C26462641. The authors acknowledge the MD members of Kyushu University Hospital for the AMD case work, and co-medical staff for assisting the medical procedures.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YO and RA wrote the manuscript; SN, SY, and TI reviewed the manuscript; and YO, SN, SY, and TI performed medical treatment for AMD management. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Oshima, Y., Apte, R.S., Nakao, S. et al. Full thickness macular hole case after intravitreal aflibercept treatment. BMC Ophthalmol 15, 30 (2015). https://doi.org/10.1186/s12886-015-0021-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-015-0021-3