
Abstract
Background
A microfluidic real-time polymerase chain reaction (PCR) system can rapidly detect the viral DNA in specimens. Detection of herpes simplex virus (HSV) and varicella-zoster virus (VZV) DNA in tears is a useful diagnostic tool for herpes simplex virus keratitis (HSK) and herpes zoster ophthalmicus (HZO).
Methods
In total, 20 patients were included in this cross-sectional study. Among them, 8 patients with infectious epithelial HSK and 12 patients with HZO were included in HSK and HZO groups, respectively. In addition, 8 patients with non-herpetic keratitis and 4 healthy individuals without keratitis were included in the control group. Numbers of HSV and VZV DNA copies in tears of all patients and individuals were evaluated using a microfluidic real-time PCR system. Regarding HSV/VZV DNA test, tear specimens were collected by filter paper method using Schirmer’s test paper, and subsequently, DNA was extracted from the filter paper using an automated nucleic acid extractor. Afterward, quantitative PCR was performed using a microfluidic real-time PCR system.
Results
From tear collection to real-time PCR result determination, the HSV/VZV DNA test took approximately 40 min. In the HSK group, the sensitivity and specificity of the HSV DNA tests were 100% each. The median value (range) of number of HSV DNA copies for affected eyes was 3.4 × 105 copies/μL (under a lower detection limit of 7.6). In the HZO group, the sensitivity and specificity of the VZV DNA tests were 100% each. The median value (range) of number of VZV DNA copies for affected eyes was 5.3 × 105 copies/μL (under a lower detection limit of 5.6 × 10–2).
Conclusion
In conclusion, quantitative PCR for HSV and VZV DNA in tears using a microfluidic real-time PCR system is useful for diagnosing and monitoring HSK and HZO.
Similar content being viewed by others


Background
Herpes simplex keratitis (HSK) is a keratitis caused by primary infection or reactivation of herpes simplex virus (HSV), with a wide variety of clinical manifestations including infectious epithelial keratitis, neurotrophic keratitis, stromal keratitis, and endotheliitis [1]. Typical infectious epithelial keratitis, including dendritic keratitis, and geographic keratitis is diagnosed by clinical findings and viral culture methods. However, atypical infectious epithelial keratitis, neurotrophic keratitis, stromal keratitis, and endotheliitis are often difficult to diagnose clinically. Consequently, supporting tests such as antigen testing and nucleic acid testing using polymerase chain reaction (PCR) methods have been considered [2,3,4]. According to a previous study, quantitative PCR is a useful diagnostic tool for infectious epithelial keratitis caused by HSV [5, 6].
Herpes zoster, caused by reactivation of the latent varicella-zoster virus (VZV) within a unilateral first branch of the trigeminal nerve, is complicated by herpes zoster ophthalmicus (HZO). HZO is characterized by the development of a variety of anterior eye diseases, including blepharitis, conjunctivitis, keratitis, and episcleritis [7]. Diagnosis of herpes zoster is based on clinical findings of skin rash, results of morphologic test by Tzanck smear [8], or detection of VZV DNA by PCR in the specimens obtained from the skin rash of patients with acute herpes zoster [9]. In clinical practice, refractory keratitis and episcleritis lasting for weeks to months are observed in some patients with HZO. Therefore, an ophthalmologic test to assess the viral activity of VZV in these patients is long-awaited. Quantitative evaluation of the VZV DNA using real-time PCR has been reported to be useful in determining the severity of the disease and the response to treatment [10].
However, the conventional real-time PCR method for estimating the amount of HSV and VZV DNA has been deemed unsuitable to use as a clinical test because of the complicated procedure and the time required for measurement.
This study aimed to establish a rapid detection method for measuring the amount of HSV/VZV DNA in tear fluid using a microfluidic real-time PCR system and to investigate its usefulness in the diagnosis of HSV and VZV keratitis.
Methods
This cross-sectional and observational study was approved by the Institutional Review Board of the Nihon University Itabashi hospital (approval number: RK-190709–2) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients enrolled in this study.
Patients
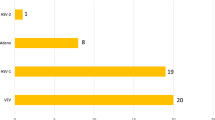
In total, 20 patients with clinically diagnosed HSK and HZO, who visited Nihon University Itabashi Hospital, Tokyo, Japan between September 2019 and June 2022 were enrolled in this study. In addition, 8 patients with non-herpetic keratitis and 4 healthy individuals without keratitis were enrolled as controls. Next, the patients and controls were divided into the following three groups: HSK (n = 8), HZO (n = 12), and control (n = 12). The patients with non-herpetic keratitis included the following: two with atopic keratoconjunctivitis; two with phlyctenular keratoconjunctivitis; two with allergic conjunctivitis; one with Stevens-Johnson syndrome; and one with ocular cicatricial pemphigoid. Demographic data are presented in Tables 1, 2, and 3.
The inclusion criteria for the HSK group were patients who experienced infectious epithelial keratitis—diagnosed based on the clinical findings of dendritic or geographic keratitis by slit-lamp examination. Exclusion criteria were the following: 1) patients who had stromal keratitis or endotheliitis form of HSK; and 2) patients who had atypical infectious epithelial keratitis.
The inclusion criteria for the HZO group were patients who experienced VZV keratitis, conjunctivitis, and/or scleritis associated with varicella-zoster dermatitis in the area of distribution of the first branch of the trigeminal nerve. In addition, the exclusion criteria were the following: 1) patients experiencing uveitis without keratitis, conjunctivitis, and scleritis and 2) patients with varicella (initial infection).
Real-time PCR for HSV and VZV DNA
Tear sampling method
The tear specimens were collected by filter paper method using Schirmer’s test paper (Schirmer Tear Production Measuring Strips, Ayumi Pharmaceutical Co., Tokyo, Japan) [5]. According to the Schirmer test technique, the Schirmer’s test paper was inserted into the lower conjunctival fornix and left in place for 1 min. Next, a 5 mm tip of the Schirmer’s test paper was cut off to extract the DNA. Tear specimens collected using Schirmer’s test paper were dissolved in cold lysis buffer [0.32 M Sucrose 5.48 g, 10 mM Trig/HCL 0.5 mL, 5 mM MgCl2 0.25 mL, and 1% Tween 20 (polyoxyethylene sorbitan monolaurate) 0.5 mL], and DNA was extracted using automated nucleic acid extractor (mag LEAD® , Hitachi, Tokyo, Japan), which required approximately 26 min.
Microfluidic real-time PCR system for HSV and VZV DNA
Measurement of tear specimens
Quantitative real-time PCR was performed using a microfluidic real-time PCR system (GeneSoC®, Kyorin, Tokyo, Japan). Gene SoC® can show three colors; therefore, simultaneous measurements of HSV DNA (Cy5) and VZV DNA (FAM) were performed in this study. Since the time required for real-time PCR was approximately 12 min, the HSV and VZV DNA test results were available in 40 min following the collection of tears.
The PCR mix contained cold lysis buffer including DNA extracts 200 μL, HSV-1 primer & probe [Probe (Cy5): TAG TGG GCC TCC ATG GG, HSV1F: GGG CCG TGA TTT TGT TTG TC, HSV1R: CCG CCA AGG CAT ATT TGC] 2.5 μL, HHV3 TaqMan probe (FAM) (TaqMan gene expression assay, Life Technologies Japan, Carlsbad, Tokyo, Japan) 1.0 μL, 10 × FAST Buffer I (Takara Bio Inc, Shiga, Japan) 2.0 μL, dNTP Mixture (Takara Bio) 1.6 μL, SpeedSTAR™ HS DNA Polymerase (Takara Bio) 0.4 μL, and distilled water 3.9 μL.
Preparation of calibration curve
For the preparation of the calibration curve, commercially available genomic DNA of Human herpes virus 1 (HHV-1, ATCC® VR-589DQ™) (American Type Culture Collection, VA, USA) 7.6 × 105 copies/μL was prepared as a standard solution for HSV DNA, and genomic DNA of Human herpes virus 3 (HHV-3, ATCC® VR-1367DQ™) (American Type Culture Collection) 5.6 × 105 copies/μL was prepared as a standard solution for VZV DNA. A dilution series of each standard viral DNA solution was prepared and measured three times each using the microfluidic real-time PCR system. Then, the mean value of the measured values was calculated to create a calibration curve.
Results
Preparation of calibration curve in quantitative PCR for HSV and VZV DNA
We developed a calibration curve to determine the amount of HSV and VZV DNA in tears (Fig. 1). The measurement ranges for HSV DNA and VZV DNA tests in tears were 7.6 × 101–7.6 × 105 and 5.6 × 10–3–5.6 × 105 copies/μL, respectively.

Calibration curve in quantitative PCR for HSV and VZV DNA in tears. We developed a calibration curve to determine the amount of HSV and VZV DNA in tears. a. The measurement ranges for HSV DNA tests in tears were 7.6 × 101–7.6 × 105 copies/μL. b. The measurement ranges for VZV DNA tests in tears were 5.6 × 10–3–5.6 × 105 copies/μL. PCR, polymerase chain reaction; HSV, herpes simplex virus; VZV, varicella-zoster virus
Analysis of sensitivity, specificity, positive predictive value, and negative predictive value
Tear specimens with a measured value were classified as positive, and those with a value under the detection limit were classified as negative (Table 4). In the HSK group, all eight patients had positive results of the HSV DNA test (in tears). In the HZO group, all 12 patients had positive results of the VZV DNA test (in tears). Furthermore, all 12 individuals in the control group had negative results for both HSV and VZV DNA tests.
The sensitivity, specificity, positive predictive value, and negative predictive value of both HSV and VZV DNA tests were 100% each (Table 4). In addition, no HSK and HZO patients had positive VZV and HSV DNA tests, respectively (Table 5).
HSV and VZV DNA levels in tears of patients
HSV and VZV DNA levels in the tears of each patient are shown in Tables 1 and 2, respectively. HSV and VZV DNA levels of all patients were within the measurement range. Median values of HSV and VZV DNA levels in tears for affected eyes were 3.4 × 105 and 5.3 × 105 copies/μL, respectively.
In the HSV group, all affected eyes were positive, while all unaffected eyes were under the detection limit of the HSV DNA tests (Fig. 2a). Six of the eight patients were complicated by atopic dermatitis with atopic keratoconjunctivitis (AKC). All six patients with AKC were treated with anti-allergic eye drops, steroid eye drops, and immunosuppressive eye drops, and none were on immunotherapy.

Comparison of HSV and VZV DNA levels in tears between affected and unaffected eyes. a. HSV DNA levels in tears of affected eyes are significantly higher than those of unaffected eyes. HSV DNA levels in all tear samples in unaffected eyes are under the detection limit. b. VZV DNA levels in tears of affected eyes are significantly higher than those of unaffected eyes. **, p < 0.01, Mann–Whitney U-test; HSV, herpes simplex virus; VZV, varicella-zoster virus; ND, not detected
In the HZO group, all eyes (affected and unaffected) tested positive in VZV DNA tests, although the VZV DNA levels in tears in the affected eyes were significantly higher than in the unaffected ones (Fig. 2b).
Representative case of HSV keratitis
A 45-year-old man (HSV2 in Table 1) with atopic keratoconjunctivitis (AKC) complicated by herpes simplex virus necrotizing keratitis in the right eye was followed up in the ophthalmology outpatient department of our hospital. AKC was active in his right eye, but necrotizing keratitis had healed into a corneal leukoma. After his initial visit two years ago, he presented to the outpatient department (Day 0) with a foreign body sensation in his right eye for several days. Bulbar conjunctival hyperemia, palpebral conjunctival hyperemia and swelling with papillary formation, and punctate corneal epitheliopathy were observed in his right eye (Figs. 3a and b). HSV DNA test using tear specimens of his right eye was performed using a microfluidic real-time PCR system; however, the results were under the lower detection limit. As a result, the ocular surface disease was diagnosed as AKC. His right eye with AKC with improved interstitial keratitis had been treated with acyclovir ophthalmic ointment (2 times per day), fluorometholone ophthalmic suspension 0.1% (one time per day), and moxifloxacin ophthalmic solution (2 times per day), and his left eye with AKC had been treated with tacrolimus ophthalmic suspension (2 times per day).

Clinical course and features of the patient with HSV keratitis. Slit-lamp examination photographs of a patient with HSV keratitis at Days 0, 42, and 49. a, and b: Photographs at Day 0 show corneal leucoma with fluorescein staining positive superficial punctate keratopathy. c, and d: Photographs at Day 42 show geographic keratitis with a dendritic tail. e, and f: Photographs at Day 49 show improvement in geographic keratitis. The area of epithelial defect with fluorescein staining gradually decreased. HSV, herpes simplex virus
On Day 42, the foreign body sensation in his right eye recurred, and he revisited the outpatient department. Geographic keratitis was observed in his right cornea, and the result of HSV DNA test using tear specimens of his right eye was positive with 2.3 × 107 copies/μL (Figs. 3c and d). The patient was treated with acyclovir ophthalmic ointment (5 times/day), fluorometholone ophthalmic suspension 0.1% (1 time/day), moxifloxacin hydrochloride (2 times/day), and valacyclovir 500 mg orally twice daily.
On Day 49, the geographic ulcer improved and HSV DNA value in tears was under the lower limit of detection (Figs. 3e and f). In this case, the microfluidic real-time PCR test was useful in the differential diagnosis between AKC and HSK, and in determining the efficacy of antiviral drugs against HSK. (Table 6).
Representative case of HZO
Case 1
A 74-year-old woman (VZV5 in Table 2) was referred to our ophthalmology department due to complaints of foreign body sensation and blurred vision in her right eye associated with herpes zoster infection in the area of distribution of the first branch of the trigeminal nerve. In the dermatological clinic one day earlier (Day 0), she was diagnosed with herpes zoster and was given antiviral medication. On Day 1, follicular conjunctivitis, pseudodendritic keratitis, and scleritis were observed during ophthalmological examination using a slit-lamp (Figs. 4a and b). During the first VZV DNA test on day 1, 3.9 × 106 and 2.1 × 102 copies/μL of VZV DNA were observed in right and left eyes, respectively, as shown in Table 7. She was treated with acyclovir systemically (750 mg/day of intravenous administration for 7 days), and acyclovir ophthalmic ointment instillation (5 times/day). The clinical course and features of the patient are shown in Figs. 4a and b. Finally, her keratitis and scleritis improved on Day 22 (Figs. 4c and d), and subsequently, the results of the VZV DNA test of both eyes were under the lower limit of detection.

Clinical course and features of the patient with VZV keratitis. Slit-lamp examination photographs of the patients with varicella-zoster ophthalmicus. a, and b: Clinical findings of case 1 on Day 1 show multiple pseudodendritic keratitis with positive fluorescein staining and scleritis. c, and d: Clinical findings of case 1 on Day 22 show that varicella-zoster ophthalmicus improved. e, and f: Clinical findings of case 2 on Day 35 show improved keratitis and continued scleritis. VZV, varicella-zoster virus
Case 2
A 49-year-old man (VZV3 in Table 2) was referred to our ophthalmology department due to complaints of swelling and difficulty in opening the right eyelids, which was associated with herpes zoster infection in the area of distribution of the first branch of the trigeminal nerve.
In the dermatological clinic three days earlier (Day 0), he was diagnosed with herpes zoster and was given antiviral medication. On Day 3, follicular conjunctivitis, pseudodendritic keratitis, and scleritis were observed during ophthalmological examination using a slit-lamp. During the first VZV DNA test on day 1, 3.5 × 107 and 9.9 × 103 copies/μL of VZV DNA were observed in right and left eyes, respectively, as shown in Table 8. Subsequently, he was treated with famciclovir 1500 mg daily systemically, and acyclovir ophthalmic ointment instillation (5 times/day). On Day 31, his eyelid swelling and conjunctivitis improved; however, scleritis on the temporal side remained. In addition, the results of the VZV DNA test were under the lower detection limit on Days 7 and 31 in the left and right eyes, respectively. On Day 38, punctate subepithelial keratitis and scleritis (Figs. 4e and f) were observed in his right eye. Subsequently, the VZV DNA test result in his right eye was re-positive with 6.2 × 101 copies/μL of VZV DNA. On Day 51, the punctate subepithelial keratitis and scleritis showed improvement in his right eye, and the VZV DNA test result was under the lower limit of detection.
Monitoring of VZV DNA levels in tears of these patients indicated that acute phase HZO shows positive VZV DNA in tears, and careful follow-up is required in HZO patients with recurrent keratitis and scleritis due to re-elevated VSV DNA levels in tears.
Discussion
We investigated the utility of the tear test for detecting HSV and VZV DNA in patients with herpetic ocular surface diseases as a clinical examination tool. In addition, in this study, herpetic keratitis including HSK and HZO was diagnosed using a microfluidic real-time PCR system. The current study demonstrated the following clinical advantages: 1) the time required for the detection of HSV and VZV DNA in tears with a microfluidic real-time PCR system was approximately 40 min; 2) the sensitivity and specificity of quantitative PCR test for HSV and VZV DNA in tears of the patients with infectious epithelial keratitis type of HSK and HZO were 100% each; 3) no cross-reaction between HSV and VZV DNA was observed.
Quantitative PCR for HSV DNA in tears is reportedly a useful diagnostic tool for HSK. Our previous multicenter study reported that the diagnosis of HSK using real-time PCR for HSV DNA had a sensitivity and specificity of 55.8% and 100%, respectively [5]. In particular, one of the factors that decreased the sensitivity of tear HSV DNA test in patients with HSK is the influence of the pre-test use of antiviral drugs such as acyclovir ophthalmic ointment, which reduces the number of HSV DNA copies. However, this study demonstrated no difference in sensitivity between the patients with acyclovir treatment and those without. In addition, background factors of herpetic ocular diseases that affect the amount of virus in tear fluid may include treatments with corticosteroids and immunosuppressive drugs, antibody immunotherapy, immune disorders such as collagen diseases and atopic dermatitis, and immunocompromised hosts. The influence of these background factors on the HSV/VZV DNA test in tears is an important issue for the future. Another factor that affects the sensitivity of the HSV DNA test is that the HSV DNA levels in tears vary depending on the clinical form and severity of HSK. The HSV DNA levels in tears are high in infectious epithelial keratitis including dendritic, geographic, and necrotizing keratitis, and low in disciform keratitis and endotheliitis [5, 10]. Therefore, it is important to set a suitable lower detection limit for the HSV DNA test to improve the sensitivity for the diagnosis of HSK. In the current study, the lower limit of detection of HSV DNA test was set at 7.6 × 101 copies/μL; furthermore, the sensitivity and specificity of HSV DNA test were 100% each in patients with and without acyclovir treatment. These results may indicate the usefulness of this HSV DNA test as a clinical diagnostic tool for infectious epithelial HSK. In addition, a high copy number of HSV DNA in tears was detected in an HSK patient with refractory keratitis that resisted topical acyclovir treatment. We considered this a severe case in which the viral load was not sufficiently reduced by topical acyclovir treatment. Therefore, systemic administration of antiviral drugs should be considered for such refractive cases. Accordingly, a clinical test that can rapidly measure the number of HSV DNA copies in the tears of the patients being treated with antiviral drugs is a useful tool for determining the clinical treatment strategy.
In the patients with HZO, corneal findings including pseudodendritic keratitis, corneal subepithelial opacity, disciform keratitis, and interstitial keratitis were observed. These corneal lesions sometimes recur, resist treatment, and become refractory. For these patients with VZV keratitis, the copy number of VZV DNA in tears has been reported to be useful not only in diagnosis but also in determining the severity of the keratitis [11]. In the current study, the copy number of VZV DNA in tears of patients with acute HZO as well as the diagnostic rate (sensitivity) was high. In addition, acute phase HZO was positive for VZV DNA in the tears of both eyes, although the VZV DNA levels in the affected eyes were significantly higher than the unaffected ones. These results suggest that in the treatment of HZO, the need for topical ocular administration of antiviral drugs, in addition to systemic administration of antiviral drugs, should be considered, taking into account the viral load in tears. On the other hand, in our reported patients who were followed up by monitoring copy number of VZV DNA in tears, re-elevation of copy number of VZV DNA in tears was observed. This re-elevation of VZV in tears of patients with HZO has not been studied previously. Therefore, in patients with refractory HZO, VZV DNA levels in tears should be monitored and the results of tear testing should be incorporated into therapeutic drug selection, especially in the indication of steroids.
This study has some limitations. First, the current study did not evaluate the usefulness of HSV DNA test in tears in patients with herpetic stromal keratitis. Herpetic stromal keratitis is divided into disciform and necrotizing keratitis. The copy number of HSV DNA is high in patients with necrotizing keratitis and almost under the detection limit in disciform keratitis in HSV DNA tests in tears [5, 10]. Therefore, the copy number of HSV DNA in the tears of patients with herpetic stromal keratitis may help select an appropriate medical treatment. In other words, steroid eye drops, which are the main drugs used in the treatment of herpetic stromal keratitis, should be administered with caution to patients with high copy numbers of HSV DNA in tears. If we examine a patient with herpetic stromal keratitis, a rapid detectable test for HSV DNA in tears may be a crucial clinical test tool in routine clinical practice. The usefulness of this HSV DNA test in patients with herpetic stromal keratitis should be evaluated in large-scale studies in the future. Second, the usefulness of the HSV and VZV DNA tests for patients with concomitant herpetic endotheliitis and uveitis is unclear because the present patient group did not include any cases of corneal endotheliitis and uveitis. HSV and VZV DNA testing of the aqueous humor is useful in diagnosing herpetic corneal endotheliitis; however, the usefulness of the tear test should be accurately verified. In addition, examining the usefulness of this test system for detecting HSV DNA and VZV DNA in aqueous humor may provide more certainty in the differential diagnosis of corneal endotheliitis and infectious uveitis. Third, viral DNA presumed to be shedding has been detected in the unaffected eyes of both HSK and HZO patients. The establishment of criteria to determine whether the amount of detected viral DNA has pathological significance or not is an important issue in this assay.
Conclusions
Rapid quantitative PCR for HSV and VZV DNA in tears using a microfluidic real-time PCR system is useful for diagnosing, appropriate use of therapeutic agents, and monitoring HSK and HZO.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, S.Y., upon reasonable request.
Abbreviations
- AKC:
-
Atopic keratoconjunctivitis
- HHV:
-
Human herpes virus
- HSV:
-
Herpes simplex virus
- HSK:
-
Herpes simplex keratitis
- PCR:
-
Polymerase chain reaction
- HZO:
-
Herpes zoster ophthalmicus
- VZV:
-
Varicella-zoster virus
References
Holland EJ, Schwartz GS. Classification of herpes simplex virus keratitis. Cornea. 1999;18:144–54.
Inoue Y, Shimomura Y, Fukuda M, Miyazaki D, Ohashi Y, Sasaki H, et al. Multicentre clinical study of the herpes simplex virus immunochromatographic assay kit for the diagnosis of herpetic epithelial keratitis. Br J Ophthalmol. 2013;97:1108–12.
Hirota A, Inada N, Shiraki Y, Shoji J, Yamagami S. Herpes simplex DNA in tears of atypical dendritic keratitis and multiple punctate subepithelial stromal opacity: a case report. Cornea. 2020;39:1177–80.
Fukuda M, Deai T, Hibino T, Higaki S, Hayashi K, Shimomura Y. Quantitative analysis of herpes simplex virus genome in tears from patients with herpetic keratitis. Cornea. 2003;22:S55-60.
Shoji J, Sakimoto T, Inada N, Kamei Y, Matsubara M, Takamura E, et al. A diagnostic method for herpes simplex keratitis by simultaneous measurement of viral DNA and virus-specific secretory IgA in tears: an evaluation. Jpn J Ophthalmol. 2016;60:294–301.
Qiu J, Huang F, Wang Z, Xu J, Zhang C. The evaluation of diagnostic efficiency for stromal herpes simplex keratitis by the combination of tear HSV-sIgA and HSV-DNA. Graefes Arch Clin Exp Ophthalmol. 2017;255:1409–15.
Liesegang TJ. Herpes zoster ophthalmicus natural history, risk factors, clinical presentation, and morbidity. Ophthalmology. 2008;115:S3-12.
Nahass GT, Goldstein BA, Zhu WY, Serfling U, Penneys NS, Leonardi CL. Comparison of Tzanck smear, viral culture, and DNA diagnostic methods in detection of herpes simplex and varicella-zoster infection. JAMA. 1992;268:2541–4.
Cohen PR. Tests for detecting herpes simplex virus and varicella-zoster virus infection. Dermatol Clin. 1994;12:51–68.
Kakimaru-Hasegawa A, Kuo CH, Komatsu N, Komatsu K, Miyazaki D, Inoue Y. Clinical application of real-time polymerase chain reaction for diagnosis of herpetic diseases of the anterior segment of the eye. Jpn J Ophthalmol. 2008;52:24–31.
Inata K, Miyazaki D, Uotani R, Shimizu D, Miyake A, Shimizu Y, et al. Effectiveness of real-time PVR for diagnosis and prognosis of varicella-zoster keratitis. Jpn J Ophthalmol. 2018;62:425–31.
Acknowledgements
We thank Mr. Mizuo Nakauchi (Kyorin Pharmaceutical Co., Ltd.) for his assistance with examination using the GeneSoc® microfluidic real-time PCR system.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
H.A. and J.S. were engaged in background research on the subject, collection of patient data, and data analysis, and were major contributors to the writing of the manuscript. N.I., Y.T., and R.A. were engaged in the collection of patient data and data analysis. S.Y. oversaw the study and reviewed the submitted manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of the Nihon University Itabashi hospital (approval number: RK-190709–2) and written informed consent was obtained from all patients enrolled in this study.
Consent for publication
Written informed consent was obtained from the patient for publication of this study and any accompanying images. A copy of the written consent is available for review by the Editor of this journal. All study participants approved the manuscript for publication.
Competing interests
J.S. has previously received honoraria from Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., AbbVie GK, and Rohto Nitten Co., Ltd., outside the submitted work. H.A., Y.S., N.I., Y.T., and R.A. declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hirota, A., Shoji, J., Inada, N. et al. Rapid detection and diagnosis of herpetic keratitis using quantitative microfluidic polymerase chain reaction system for herpes simplex and varicella-zoster virus DNA: a case series. BMC Ophthalmol 23, 177 (2023). https://doi.org/10.1186/s12886-023-02938-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-023-02938-w