
Abstract
Background
Short-term exposure to air pollution is associated with acute lower respiratory infections (ALRI) in children. We investigated the relationship between hospitalization for ALRI in children and air pollutant concentrations from January 1, 2014 to December 31, 2020 in Lanzhou City.
Methods
We collected data on air pollutant concentrations and children’s hospitalization data during the study period. A time series regression analysis was used to assess the short-term effects of air pollutants on ALRI in children, and subgroup analyses and sensitivity analyses were performed.
Results
A total of 51,206 children with ALRI were studied, including 40,126 cases of pneumonia and 11,080 cases of bronchiolitis. The results of the study revealed that PM2.5, PM10, SO2 and NO2 were significantly associated with hospitalization for ALRI in children aged 0–14 years. For each 10 µg/m3 increase in air pollutant concentration in lag0-7, the relative risk of ALRI hospitalization in children due to PM2.5, PM10, SO2 and NO2 increased by 1.089 (95%CI:1.075, 1.103), 1.018 (95%CI:1.014, 1.021), 1.186 (95%CI:1.154. 1.219) and 1.149 (95%CI:1.130, 1.168), respectively.
Conclusions
PM2.5, PM10, SO2 and NO2 short-term exposures were positively associated with ALRI, pneumonia and bronchiolitis hospitalizations in Lanzhou, China. Local governments should make efforts to improve urban ambient air quality conditions to reduce hospitalization rates for childhood respiratory diseases.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Previous studies demonstrated that short-term exposure to air pollutants could cause various adverse health effects in people of different ages, such as respiratory and cardiovascular diseases [1,2,3,4,5]. Children have immature respiratory development, narrow bronchi, higher lung ventilation rates and lower immune capacity [6]. Therefore, children are more vulnerable to air pollution than adults. Acute lower respiratory infections (ALRI), including pneumonia and bronchiolitis, are a frequent respiratory disease and account for nearly one-fifth of the world’s mortality in young children and hospitalization for ALRI can account for 30–50% of pediatric hospitalizations [7, 8]. ALRI poses a huge threat to the life and health of children.
Currently, a number of studies have shown a strong correlation between air pollution and ALRI in children [9,10,11,12,13,14]. For instance, a Korean study found that exposure to fine particulate matter (PM2.5) was associated with ALRI hospitalization in children [15]. A study found an association between PM2.5 and hospitalization for pneumonia and bronchitis in children in the United States [16].
Similarly, the harmful effects of air pollutants on the respiratory tract of children have been found in several studies in China [17,18,19]. However, studies on the association of air pollutants with lower respiratory tract infections in children have focused on the harmful effects of ambient particulate matter in China and the majority of studies were from economically developed regions in eastern China. Only a few involved the effects of gaseous air pollutants on lower respiratory tract diseases in children [20,21,22]. Environmental particulate matter, such as PM2.5 and coarse particulate matter (PM10), can trigger oxidative stress and inflammation in lung tissues directly and can also enter the bloodstream through the respiratory tract. It causes not only damage to the respiratory tract but also extensive damage to the cardiovascular system [23]. Gaseous air pollutants, such as sulfur dioxide (SO2) and nitrogen dioxide (NO2), often damage mucous membranes and cause constriction of the airways [24]. Nonetheless, there is a limited amount of research on the correlation between air pollutants and hospitalization for ALRI in children.
The social and economic development level and the air pollution level will vary according to the geographical environment [25]. Lanzhou City is located in the inland area of northwest China, and its economic development is relatively backward. Air pollution is more serious than in southeastern China. Lanzhou is a typical river valley city, and the topographical features make air pollutants tend to disperse untimely. The adverse effects of air pollution are exacerbated by the gradual increase in hazy weather.
We performed this study to assess the association of major air pollutants (PM2.5, PM10, SO2, and NO2) with hospitalization for pediatric ALRI in Lanzhou, China. We also analyzed the association of air pollutants with hospitalization for specific etiologies, namely pneumonia and bronchitis. In addition, we also performed gender, age and seasonal stratified analyses.
Methods
Study area
Lanzhou is an inland city in northwest China. It is geographically situated on the Loess Plateau and has a temperate continental climate with relatively dry climate and low precipitation throughout the year. Lanzhou is an important transportation city in China and an important node city of the Silk Road Economic Belt. Lanzhou City has eight county-level administrative regions under its jurisdiction. Our study area is the four main urban areas (Chengguan, Qilihe, Xigu and Anning).
Hospitalizations data
We collected information on inpatients aged 0–14 years from January 1, 2014 to December 31, 2020 from seven large general hospitals in Lanzhou City. These data included patient case number, admission diagnosis, age, gender, time of admission, and home address. Admission diagnoses were coded according to the International Classification of Diseases, 10th Revision (ICD-10). We selected the diseases involved in this study according to ICD-10 codes: acute lower respiratory infections (J12-J18 and J20-J22), pneumonia (J12-J18) and bronchiolitis (J20-J21) [26, 27]. We excluded patients whose home address was not within the study area for visits. We removed patients with errors and missing gender and age. To exclude double counting of the same patient due to multiple visits, we included only the first visit record of the patient during the study period. Because multiple visits by a patient may be due to referrals, transfers, or follow-up visits.
Air pollution and meteorological data
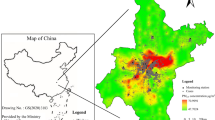
During the study period, air pollutant concentration data were recorded at four national air quality testing stations in urban Lanzhou. The arithmetic mean of the 24-h average concentration values of the major air pollutants at each monitoring station was taken. Four air pollutants that are closely related to respiratory diseases were selected: PM2.5, PM10, SO2, and NO2 [28]. In this study, as individual exposure levels could not be accurately estimated, the average of all pollutant monitoring station data was considered as the previously defined individual exposure level. Lanzhou City is a river-valley type city, and the terrain is characterized by a narrow east–west direction and a narrow north–south direction facing the mountains. Residential areas are mainly concentrated on both sides of the city roads, and the location of the air quality monitoring station is not more than 15 km away from the residential areas [29, 30]. Therefore, the monitoring data from the air quality testing station can well represent the exposure concentration of the residents. Figure 1 shows the location of the four national air quality monitoring stations in Lanzhou. We obtained meteorological data, including daily average temperature and average relative humidity data from China Meteorological website Data Service Center (http://data.cma.cn) for the periods from January 1, 2014 to January 31, 2020. During the study period, we did not find any missing pollutant concentration data and meteorological data.

Location of air quality monitoring stations in Lanzhou
Statistical analysis
Time series studies have been widely utilized to study the short-term effects of air pollution on human health. Prior to modeling, we provided a descriptive statistical analysis of the relevant data. Similarly, we analyzed the correlations between major air pollutants and meteorological factors using Spearman correlation coefficients. Hospitalization of children for ALRI is considered a small probability event and follows a quasi-Poisson distribution. We used generalized linear models and distributional lag models with a family of quasi-Poisson distributions to investigate the effect of air pollutants on hospitalization for ALRI in children. We formulated a cross-basis for air pollutant with a linear function in both the predictor space and the lag structure stratification with constraints. Meteorological factors and long-term trends are controlled by natural cubic spline functions. By combining the previous relevant studies [31,32,33], we constructed the following statistical model:
where t is the observation day. Yt is the dependent variable, indicating the number of children admitted for ALRI on day t. E(Yt) is the expected value of hospital admissions due to ALRI for children on that day. α is the intercept in the model. cb denotes the cross-basis function, which determines the matrix with the linear and lag matrices of air pollutants using a linear function and a natural cubic spline function with three dfs, respectively. xt indicates PM2.5, PM10, SO2 and NO2. l is the lag of the xt. ns is the natural cubic spline function, time is the time variable, tempt is the average temperature on day t, rht is the average relative humidity on day t, and df is the degree of freedom. DOW is a dummy variable denoting the control week effect, and Holiday is a dummy variable denoting the control public holiday. We set the degrees of freedom for the variables of interest in this study based on previous related studies [28, 34]. The ultimate incorporated model the degrees of freedom for time, temperature, and humidity were 7, 3, and 3 respectively.
Based on the experience of previous related studies [35], we constructed eight single-lag structures (lag0-lag7) and seven cumulative lag structures (lag0-1 ~ lag0-7) to estimate the short-term effects of air pollutants on children’s disease (ALRI, pneumonia and bronchiolitis) hospitalization. The estimates were expressed as relative risk (RR) values and corresponding 95% confidence intervals (CIs) for each 10 µg/m3 increase in concentrations of PM2.5, PM10, SO2, and NO2 for childhood ALRI hospitalizations. We further conducted subgroup analyses to estimate the effect of air pollutant concentration variations on age (< 5 years and 5–14 years) [26, 27], gender (boy or girl) and season (cool season from October to March and warm season from April to September). We then further assessed the significant differences between the effect estimates of the stratified analyses by calculating 95% CIs using the following equation:
where \({\widehat{\mathrm{Q}}}_{1}\) and \({\widehat{\mathrm{Q}}}_{2}\) indicate the estimates for two subgroups (e.g., boy and girl), \(\mathrm{S}{\widehat{\mathrm{E}}}_{1}\) and \(\mathrm{S}{\widehat{\mathrm{E}}}_{2}\) are their appropriate standard errors.
We selected the maximum effect time for the short-term effects of air pollutants on children’s ALRI for sensitivity analysis. Based on previous related studies, we assessed the stability of the model results by constructing a two-pollutant model and varying the degrees of freedom of the time variable (df = 6 ~ 10) [36]. All statistical analyses for this study were performed using R software. Two-sided tests with P values less than 0.05 were considered statistically significant.
Results
Descriptive statistics of children’s ALRI hospitalization, air pollutants and meteorological factors
From January 1, 2014 to December 31, 2020, a total of 51,206 ALRI patients 0–14 years old were hospitalized in Lanzhou City, of which 40,126 (78.36%) were admitted for pneumonia and 11,080 (21.64%) were admitted for bronchiolitis. Table 1 summarizes the descriptive statistics of daily hospitalizations, air pollutant concentrations and meteorological factors. During the study period, the average daily ALRI hospitalization was 20 (range 0–91), of which 16 were pneumonia-related (range 0–81) and 4 were bronchiolitis-related (range 0–18). The mean concentrations of PM2.5, PM10, SO2 and NO2 during the study period were 47.8, 112.0, 20.6 and 48.2 µg/m3, respectively. The average daily temperature was 11.1 °C and the average relative humidity was 51.6%.
Figure 2 represents the temporal trends of the main air pollutants during the period of study and what we can know is that air pollution has seasonal trends, especially PM2.5 and SO2.

Temporal changes in air pollutant concentrations in 2014–2020
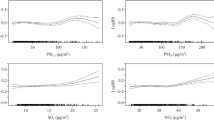
Figure 3 shows the concentration–response relationships of four air pollutants with ALRI, pneumonia, and bronchitis. We can find that increased concentrations of PM2.5, PM10, SO2 and NO2 all lead to an increased relative risk of hospitalization for ALRI, pneumonia and bronchiolitis, and none of them has a threshold.

The exposure-response curves between air pollutants and ALRI hospitalizations in children
Table S1 shows the Spearman correlation coefficients of the main air pollutants and meteorological factors. All of the air pollution are positively correlated with each other. Among them, PM2.5 is highly positively correlated with PM10 with a correlation coefficient of 0.85. Air pollutants are negatively correlated with both temperature and relative humidity.
Figure 4 and Table S2 show the short-term effects of the four air pollutants on children hospitalized (ALRI, pneumonia and bronchiolitis) on the day of admission and at the various lag days.

Relative risk (95%CI) of overall and cause-specific ALRI hospital admissions associated with an increase of 10 µg/m3 in PM2.5, PM10, SO2 and NO2 along different lag structures, using single pollutant models
PM2.5 had a harmful effect on ALRI and pneumonia at different lag days and both had a maximum lag effect at lag0-7, with RR values of 1.089 (95% CI:1.075,1.103) and 1.094 (95% CI:1.079, 1.109), respectively. PM2.5 had a harmful effect on bronchiolitis at most lag days, except for lag1, lag2 and lag7, similarly the maximum lag effect was seen in lag0-7, RR = 1.067, (95% CI:1.048,1.086).
PM10 had a similar effect on ALRI and pneumonia admissions. In the single lag structure, there was a harmful effect only at lag0, lag2, and lag3, with no harmful effect at any other single lag days. However, there was a harmful effect at all cumulative lag days, and the largest effect occurred at lag0-7, RR = 1.018 (95% CI:1.014,1.021) and RR = 1,018 (95% CI:1.043,1.021), respectively. However, the effect of PM10 on bronchiolitis was harmful only at the cumulative lag days with a maximum effect RR = 1.015 (95% CI:1.010, 1.020) at lag0-7.
SO2 has a similar effect on ALRI and pneumonia. The effect was harmful only at lag0, lag1 and lag6 in single lag days. However, it was harmful at all cumulative lags, and the maximum lag effect occurred at lag0-7, RR = 1.186 (95% CI:1.154,1.219) and RR = 1,188 (95% CI:1.154,1.224), respectively. The effect of SO2 on bronchiolitis at lag0, lag3, lag5 and lag0-1 ~ lag0-7 was harmful, with a maximum effect of RR = 1.185 (95% CI:1.133, 1.239) at lag0-6.
NO2 had a comparable effect on ALRI and pneumonia admissions. At all single lag days, the effect estimates of the effects were not harmful only at lag3 and lag7. However, at all cumulative lag days, NO2 had a harmful effect on ALRI and pneumonia admissions, with the largest lag effects occurring at lag0-7, with RRs of 1.149 (95% CI:1.130,1.168) and 1.155 (95% CI:1.135,1.176), respectively. The effect is harmful for NO2 on bronchiolitis at lag0, lag2, lag6 and lag0-1 ~ lag0-7 with maximum effect RR = 1.115 (95% CI:1.085, 1.146) at lag0-6.
Subgroup analysis by gender, age and season
Table 2 shows the relative risk estimates for different air pollutants for each disease. There were no statistically significant between-group differences for different diseases stratified by gender for different air pollutant exposures (p > 0.05), but the pollutant exposures all showed deleterious effects (Table S3). Age subgroup results showed statistically significant differences in the harmful effects of only PM2.5 and NO2 on hospitalization for both ALRI and pneumonia (p < 0.05). The harmful effects of PM2.5 are stronger in the < 5 years age group, while those of NO2 are stronger in the 5–14 years age group. No results with significant differences for age stratification were observed for any of the remaining pollutant exposures (p > 0.05), but the pollutant exposures all had harmful effects (Table S4). Seasonal subgroup results showed statistically significant differences in the harmful effects of PM2.5 on hospitalizations for ALRI and bronchiolitis, and PM10 and NO2 on hospitalizations for ALRI, pneumonia and bronchiolitis (p < 0.05). The effects of short-term exposure to the four air pollutants on childhood ALRI hospitalization were stronger in the cold season compared to the warm season. However, pollutant exposure had deleterious effects on ALRI and pneumonia hospitalization in both warm and cold seasons. In contrast, the harmful effects of pollutant exposure on bronchiolitis hospitalization were only observed in the cold season (Table S5).
Sensitivity analysis
Firstly, we chose the time of maximum effect of each air pollutant to verify the stability of the model by constructing a two-pollutant model. PM2.5 and PM10 are highly correlated with a Spearman correlation coefficient of 0.85, therefore we do not introduce them into the same model at the same time. Table S6 summarizes the results of the two-pollutant model. We can find that the effect between particulate matter and ALRI, pneumonia and bronchiolitis hospitalization is diminished after controlling for gaseous pollutants, but it is still statistically significant. Similarly, when we control for particulate matter, the effect between gaseous pollutants and their outcome changes ALRI, pneumonia and bronchiolitis hospitalizations is attenuated, but still statistically significant.
Secondly, we also chose the time of maximum effect of each air pollutant and performed sensitivity analysis by changing the degrees of freedom of the time variable (Table S7). We found that changing the degrees of freedom of time to 6, 8, 9 and 10 did not significantly change the short-term effects of air pollutants on ALRI, pneumonia and bronchiolitis.
Discussion
This study assessed the correlation between short-term exposure to air pollution and the risk of hospitalization for ALRI in children from 2014 to 2020 in Lanzhou, China, using a time-series analysis. Our findings suggest that short-term exposure to air pollutants leads to an increased risk of hospitalization for ALRI, pneumonia, and bronchitis in children after controlling for temperature and relative humidity. PM2.5 had a stronger deleterious effect compared to PM10. The estimated relative risk of childhood ALRI hospitalization from SO2 exposure was greater than that from NO2 at lag0-7. However, NO2 exhibited a deleterious effect on childhood ALRI hospitalization at all lag times, except at Lag7. In conclusion, our findings add to the evidence that air pollutants increase the risk of ALRI in children in developing countries and regions.
The harmful effects of particulate matter on children with ALRI are consistent with the findings of previous studies. Our study found that for every 10 µg/m3 increase in PM2.5 concentration, the relative risk of hospitalization for ALRI, pneumonia and bronchitis in children increased by 1.089 (95% CI: 1.075, 1.103), 1.094 (95% CI: 1.079, 1.1094) and 1.067 (95% CI: 1.048, 1.086) respectively at lag0-7. For each 10 µg/m3 increase in PM10 concentration, the relative risk of hospitalization for ALRI and pneumonia in children increased by the same amount, RR = 1.018 (95% CI:1.014,1.021) at lag0-7. The relative risk of hospitalization for bronchitis was increased by 1.015 (95% CI:1.01,1.02) at lag0-7. The harmful effect has been found in several other studies. For example, a study in Vietnam found that every 10 µg/m3 increase in PM2.5 concentration was associated with a 3.51 (95% CI: 0.96,6.12) increase in the risk of hospital admission for ALRI in children at lag3 [11]. A Korean study also found a strong linear correlation between PM2.5 and childhood ALRI hospitalization and an increase of 1.20% (95% CI: 0.71, 1.71) in ALRI hospitalization for every 10 µg/m3 increase in PM2.5 concentration at lag0-7 [15]. A study conducted in Sichuan, China, found a 1.23% (95% CI: 0.21,2.26) increase in the risk of hospitalization for childhood bronchitis for every 10 µg/m3 increase in PM2.5 at lag0-7 [28]. Another study in the region, Sichuan, found that for each 10 µg/m3 increase in PM2.5 at lag4 and PM10 at lag0-10, the relative risk of hospitalization for childhood pneumonia was 1.0064 (95% CI:1.0004,1.0124) and 1.0168 (95% CI:1.0089,1.0248), respectively [19]. A study in Jinan, China found a correlation between PM2.5 and PM10 and childhood pneumonia admissions, with each 10 µg/m3 increase in PM2.5 and PM10 associated with 6% (95% CI:1.02,1.10) increase in lag1 and 4% (95% CI:1.00,1.08) increase in lag2, respectively [37]. A study in Hefei, China, showed that for every 10 µg/m3 increase in PM2.5 and PM10 concentrations at lag0-2, the risk of hospitalization for pneumonia increased by 1.21% (95% CI:0.34%, 2.09%) and 1.10% (95% CI:0.44%, 1.76%), respectively [38]. These studies also showed a stronger effect of PM2.5 compared to PM10 on children’s ALRI hospitalization. Unlike our study, the time to maximum harmful effects did not occur at the same time for different particulate matter and their risk values for hospitalization for ALRI in children were not identical. It could be caused by various regions, particulate matter composition in the urban environment and social lifestyles and habits.
We found that PM2.5 had the strongest harmful effect on hospitalization for pneumonia compared to fine bronchitis and ALRI at lag0-7, RR = 1.094 (95% CI:1.079, 1.109). Components of PM2.5, such as elemental carbon, organic carbon and nitrate, are associated with hospitalization for respiratory diseases in children such as pneumonia and bronchitis, and are most correlated with pneumonia [39]. Due to the complex composition and smaller aerodynamic diameter of PM2.5, it can easily enter deeper into the respiratory tract and deposit in the lung tissue. It can enter the circulatory system through the blood gas barrier and cause more extensive damage to the body. PM10 has a relatively small impact on children’s ALRI hospitalization, but still has harmful effects. Currently, the toxicological mechanisms of PM2.5 damage to the respiratory system are mainly free radical peroxidation, imbalance of intracellular calcium homeostasis and inflammatory damage [40].
Gaseous air pollutants also have harmful effects on children with ALRI. A Brazilian study found a 7% relative risk of pneumonia hospitalization for NO2 at lag1 [41]. A study conducted in eastern China similarly found that for each 10-unit increase in SO2 and NO2, pediatric pneumonia hospitalizations increased by 11.21% (95% CI:4.70%, 18.10%) and 5.42% (95% CI:3.07%, 7.82%), respectively [35]. SO2 is mainly originated from the combustion of coal, oil and other sulfur-containing minerals. When SO2 enters the respiratory tract, it can form the corresponding derivatives, the sodium bisulfite and sulfite, which are toxic to the respiratory system [42]. NO2 is primarily sourced from vehicle exhaust. Short-term exposure to NO2 may enhance airway inflammation by modulating Th1/Th2 differentiation and activating the JAK-STAT pathway, thereby causing lung injury [43].
The results of gender stratified analysis showed that PM2.5, PM10 and SO2, except NO2, had a stronger harmful effect on ALRI hospitalization in boys. A Korean study similarly found a stronger association between PM2.5 exposure and ALRI in boys (1.31%, 95% CI: 0.75, 1.86) [15]. It is consistent with several studies in other regions of China, such as Hefei and Guangzhou [17, 38]. However, in contrast to these studies, we found that NO2 had a stronger harmful effect on girls. This might be attributed to the more severe air pollution conditions in Lanzhou compared to the eastern regions of China. During our study period, the average daily NO2 concentration in Lanzhou was 48.2 µg/m3. In comparison, the average NO2 concentrations in Ningbo and Guangzhou, China were 39.7 µg/m3 and 45.2 µg/m3 [17, 35]. Gender differences in the effects of air pollution on respiratory disease in children still exist and the corresponding mechanisms are unclear. The different sensitivity of boys and girls to air pollutants may be due to the interaction of anatomical, genetic and physiological differences as well as behavioral factors [44]. Furthermore, boys spend more time outdoors than girls, which may also contribute to boys’ greater vulnerability to air pollution.
Age-stratified results showed that PM2.5, PM10 and SO2 were more significant hazards for children hospitalized with ALRI in the < 5 years age group. The results are compatible with previous studies [38]. Children in the < 5 years old age group are more susceptible to the effects of air pollution because of their weaker immune defenses and immature respiratory systems. NO2 was more associated with ALRI hospitalization in children aged 5–14 years. A study from southern Brazil also found NO2 to be associated with respiratory hospitalization only in children aged 6–15 years (IRR = 1.14, 95% CI:1.11,1.17) [45]. The main source of NO2 is traffic pollution. School-age children are more likely to spend more time outdoors and have more exposure to traffic pollution, so they are more affected by NO2.
Seasonal stratification analysis showed that the effects of PM2.5, PM10, SO2 and NO2 on children’s ALRI hospitalization were more powerful in the cold season. Cold stimulation impairs the ciliary function of the respiratory mucosa thereby inhibiting the clearance of pollutants [46]. Cold air increases the number of inflammatory cells in the lower respiratory tract, such as centrophages and macrophages [47]. In addition, the cold has a relationship with air pollution, such as the cooling effect of nitrate particles and organic carbon of PM2.5 components on the climate, and the possible coexistence of extreme cold and particulate pollution [48]. In addition, cold air and gaseous air pollutants have a combined damaging effect on the respiratory tract [49]. This all makes the impact of air pollutants on respiratory diseases more significant in the cold season.
The strengths of our study are as follows: to our knowledge, this is the first study in Lanzhou on the relationship between exposure to major air pollutants and hospital admissions for ALRI in children. We stratified the outcomes of childhood ALRI hospitalizations by pollutants, diseases (pneumonia and bronchitis), gender, age and season. There are some limitations in our study. Firstly, this is an ecological study and, similar to other studies, we used averages from fixed national air quality monitoring stations as an indicator of individual exposure levels, which inevitably leads to exposure measurement error. Secondly, our study did not include individual confounding factors such as second-hand smoke exposure, personal history of disease, activity patterns, etc., which may also have an impact on individual exposure.
Conclusion
Our findings show that PM2.5, PM10, SO2 and NO2 short-term exposures were positively associated with ALRI, pneumonia and bronchiolitis hospitalizations in Lanzhou, China. Moreover, PM2.5, PM10 and SO2 had stronger effects on the boy group and the 5–14 years age group, while NO2 had the opposite but still significant deleterious effects. All pollutants were stronger for children ALRI hospitalization in the cold season. Therefore, efforts should be made to improve urban ambient air quality conditions to reduce hospitalization rates for respiratory diseases in children.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due the data is collected for administrative purposes but are available from the corresponding author on reasonable request.
References
Slama A, Śliwczyński A, Woźnica J, Zdrolik M, Wiśnicki B, Kubajek J, Turżańska-Wieczorek O, Gozdowski D, Wierzba W, Franek E. Impact of air pollution on hospital admissions with a focus on respiratory diseases: a time-series multi-city analysis. Environ Sci Pollut Res Int. 2019;26(17):16998–7009.
Phosri A, Ueda K, Phung VLH, Tawatsupa B, Honda A, Takano H. Effects of ambient air pollution on daily hospital admissions for respiratory and cardiovascular diseases in Bangkok, Thailand. Sci Total Environ. 2019;651(Pt 1):1144–53.
Quintyne KI, Sheridan A, Kenny P, O’Dwyer M. Air quality and its association with cardiovascular and respiratory hospital admissions in Ireland. Ir Med J. 2020;113(6):92.
Sacramento DS, Martins LC, Arbex MA, Pamplona YAP. Atmospheric pollution and hospitalization for cardiovascular and respiratory diseases in the city of Manaus from 2008 to 2012. ScientificWorldJournal. 2020;2020:8458359.
Żyrek D, Krzemińska A, Żyrek N, Wajda A, Pabian W, Pacholski M, Sokolski M, Zymliński R. Effects of exposure to air pollution on acute cardiovascular and respiratory admissions to the hospital and early mortality at emergency department. Adv Clin Exp Med. 2022;31(10):1129–38.
Chen CH, Chan CC, Chen BY, Cheng TJ, Leon Guo Y. Effects of particulate air pollution and ozone on lung function in non-asthmatic children. Environ Res. 2015;137:40–8.
Mehta S, Shin H, Burnett R, North T, Cohen AJ. Ambient particulate air pollution and acute lower respiratory infections: a systematic review and implications for estimating the global burden of disease. Air Qual Atmos Health. 2013;6(1):69–83.
Collaborators GL. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17(11):1133–61.
Horne BD, Joy EA, Hofmann MG, Gesteland PH, Cannon JB, Lefler JS, Blagev DP, Korgenski EK, Torosyan N, Hansen GI, et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am J Respir Crit Care Med. 2018;198(6):759–66.
Sonego M, Pellegrin MC, Becker G, Lazzerini M. Risk factors for mortality from acute lower respiratory infections (ALRI) in children under five years of age in low and middle-income countries: a systematic review and meta-analysis of observational studies. PLoS One. 2015;10(1):e0116380.
Luong LTM, Dang TN, Thanh Huong NT, Phung D, Tran LK, Van Dung D, Thai PK. Particulate air pollution in Ho Chi Minh city and risk of hospital admission for acute lower respiratory infection (ALRI) among young children. Environ Pollut (Barking, Essex : 1987). 2020;257:113424.
Cai YS, Gibson H, Ramakrishnan R, Mamouei M, Rahimi K. Ambient air pollution and respiratory health in Sub-Saharan African children: a cross-sectional analysis. Int J Environ Res Public Health. 2021;18(18):9729.
Cheng J, Su H, Xu Z. Intraday effects of outdoor air pollution on acute upper and lower respiratory infections in Australian children. Environ Pollut (Barking, Essex : 1987). 2021;268(Pt A):115698.
Abudureyimu K, Suryadhi MAH, Yorifuji T, Tsuda T. Exposure to fine particulate matter and acute upper- and lower-respiratory tract infections (AURI and ALRI) in children under five years of age in India. Arch Environ Occup Health. 2023;78(1):1–6.
Oh J, Han C, Lee DW, Jang Y, Choi YJ, Bae HJ, Kim S, Ha E, Hong YC, Lim YH. Short-term exposure to fine particulate matter and hospitalizations for acute lower respiratory infection in Korean children: a time-series study in seven metropolitan cities. Int J Environ Res Public Health. 2020;18(1):144.
Glick AF, Tomopoulos S, Fierman AH, Elixhauser A, Trasande L. Association between outdoor air pollution levels and inpatient outcomes in pediatric pneumonia hospitalizations, 2007 to 2008. Acad Pediatr. 2019;19(4):414–20.
Liang Z, Meng Q, Yang Q, Chen N, You C. Size-specific particulate matter associated with acute lower respiratory infection outpatient visits in children: a counterfactual analysis in Guangzhou, China. Front Public Health. 2021;9:789542.
Zhuang J, Bai H, Sun J, Zhang T, Li J, Chen Y, Zhang H, Sun Q. The association between fine particulate matter and acute lower respiratory infections in Yancheng City, China. Environ Sci Pollut Res Int. 2021;28(43):61723–31.
He Y, Jiang W, Gao X, Lin C, Li J, Yang L. Short-term effects and economic burden of air pollutants on acute lower respiratory tract infections in children in Southwest China: a time-series study. Environ Health. 2023;22(1):6.
Zheng PW, Wang JB, Zhang ZY, Shen P, Chai PF, Li D, Jin MJ, Tang ML, Lu HC, Lin HB, et al. Air pollution and hospital visits for acute upper and lower respiratory infections among children in Ningbo, China: a time-series analysis. Environ Sci Pollut Res Int. 2017;24(23):18860–9.
Guo J, Ma M, Xiao C, Zhang C, Chen J, Lin H, Du Y, Liu M. Association of air pollution and mortality of acute lower respiratory tract infections in Shenyang, China: a time series analysis study. Iran J Public Health. 2018;47(9):1261–71.
Wang J, Cao H, Sun D, Qi Z, Guo C, Peng W, Sun Y, Xie Y, Liu X, Li B, et al. Associations between ambient air pollution and mortality from all causes, pneumonia, and congenital heart diseases among children aged under 5 years in Beijing, China: a population-based time series study. Environ Res. 2019;176:108531.
Thangavel P, Park D, Lee YC. Recent insights into particulate matter (PM(2.5))-mediated toxicity in humans: an overview. Int J Environ Res Public Health. 2022;19(12):7511.
Upadhyay S, Chakraborty A, Thimraj TA, Baldi M, Steneholm A, Ganguly K, Gerde P, Ernstgård L, Palmberg L. Establishment of repeated in vitro exposure system for evaluating pulmonary toxicity of representative criteria air pollutants using advanced bronchial mucosa models. Toxics. 2022;10(6):277.
Liang D, Wang YQ, Wang YJ, Ma C. National air pollution distribution in China and related geographic, gaseous pollutant, and socio-economic factors. Environ Pollut (Barking, Essex : 1987). 2019;250:998–1009.
Xiao D, Guo W, Xu D, Chen J, Liang Z, Zhang X. Three exposure metrics for fine particulate matter associated with outpatient visits for acute lower respiratory infection among children in Guangzhou, China. Front Public Health. 2022;10:876496.
Liang Z, You C, Zhang X, Wang X, Xiao D, He S, Wu F, Meng Q. Three exposure metrics of size-specific particulate matter associated with acute lower respiratory infection hospitalization in children: a multi-city time-series analysis in China. Sci Total Environ. 2022;816:151636.
He Y, Jiang W, Liao JQ, Jing L, Li J, Yang L. Short-term effects of air pollutants on hospital admissions for acute bronchitis in children: a multi-city time-series study in Southwest China. World J Pediatr. 2022;18(6):426–34.
Dong J, Wang Y, Wang J, Bao H. Association between atmospheric PM(2.5) and daily outpatient visits for children’s respiratory diseases in Lanzhou. Int J Biometeorol. 2021;65(7):989–99.
Wu T, Yang X, Chu A, Xie X, Bai M, Peng Y, Zhang Z. Acute effects of fine particulate matter (PM2.5) on hospital admissions for cardiovascular diseases in Lanzhou, China: a time-series study. Environ Sci Europe. 2022;34(1):55.
Liang S, Sun C, Liu C, Jiang L, Xie Y, Yan S, Jiang Z, Qi Q, Zhang A. The influence of air pollutants and meteorological conditions on the hospitalization for respiratory diseases in Shenzhen city, China. Int J Environ Res Public Health. 2021;18(10):5120.
Zhou X, Gao Y, Wang D, Chen W, Zhang X. Association between sulfur dioxide and daily inpatient visits with respiratory diseases in Ganzhou, China: a time series study based on hospital data. Front Public Health. 2022;10:854922.
Ibrahim MF, Hod R, Ahmad Tajudin MAB, Wan Mahiyuddin WR, Mohammed Nawi A, Sahani M. Children’s exposure to air pollution in a natural gas industrial area and their risk of hospital admission for respiratory diseases. Environ Res. 2022;210:112966.
Pu X, Wang L, Chen L, Pan J, Tang L, Wen J, Qiu H. Differential effects of size-specific particulate matter on lower respiratory infections in children: a multi-city time-series analysis in Sichuan, China. Environ Res. 2021;193:110581.
Zhou X, Guo M, Li Z, Yu X, Huang G, Li Z, Zhang X, Liu L. Associations between air pollutant and pneumonia and asthma requiring hospitalization among children aged under 5 years in Ningbo, 2015–2017. Front Public Health. 2022;10:1017105.
Xu H, Wang X, Tian Y, Tian J, Zeng Y, Guo Y, Song F, Xu X, Ni X, Feng G. Short-term exposure to gaseous air pollutants and daily hospitalizations for acute upper and lower respiratory infections among children from 25 cities in China. Environ Res. 2022;212(Pt D):113493.
Lv C, Wang X, Pang N, Wang L, Wang Y, Xu T, Zhang Y, Zhou T, Li W. The impact of airborne particulate matter on pediatric hospital admissions for pneumonia among children in Jinan, China: a case-crossover study. J Air Waste Manag Assoc. 2017;67(6):669–76.
Wang X, Xu Z, Su H, Ho HC, Song Y, Zheng H, Hossain MZ, Khan MA, Bogale D, Zhang H, et al. Ambient particulate matter (PM(1), PM(2.5), PM(10)) and childhood pneumonia: the smaller particle, the greater short-term impact? Sci Total Environ. 2021;772:145509.
Ostro B, Roth L, Malig B, Marty M. The effects of fine particle components on respiratory hospital admissions in children. Environ Health Perspect. 2009;117(3):475–80.
Xing YF, Xu YH, Shi MH, Lian YX. The impact of PM2.5 on the human respiratory system. J Thorac Dis. 2016;8(1):E69-74.
Souza LS, Nascimento LF. Air pollutants and hospital admission due to pneumonia in children: a time series analysis. Rev Assoc Med Bras (1992). 2016;62(2):151–6.
Li R, Meng Z. Effects of SO2 derivatives on expressions of MUC5AC and IL-13 in human bronchial epithelial cells. Arch Toxicol. 2007;81(12):867–74.
Ji X, Han M, Yun Y, Li G, Sang N. Acute nitrogen dioxide (NO2) exposure enhances airway inflammation via modulating Th1/Th2 differentiation and activating JAK-STAT pathway. Chemosphere. 2015;120:722–8.
Silveyra P, Fuentes N, Rodriguez Bauza DE. Sex and gender differences in lung disease. Adv Exp Med Biol. 2021;1304:227–58.
Agudelo-Castañeda DM, Calesso Teixeira E, Alves L, Fernández-Niño JA, Rodríguez-Villamizar LA. Monthly-term associations between air pollutants and respiratory morbidity in South Brazil 2013–2016: a multi-city, time-series analysis. Int J Environ Res Public Health. 2019;16(20):3787.
Clary-Meinesz CF, Cosson J, Huitorel P, Blaive B. Temperature effect on the ciliary beat frequency of human nasal and tracheal ciliated cells. Biol Cell. 1992;76(3):335–8.
Larsson K, Tornling G, Gavhed D, Müller-Suur C, Palmberg L. Inhalation of cold air increases the number of inflammatory cells in the lungs in healthy subjects. Eur Respir J. 1998;12(4):825–30.
D’Amato M, Molino A, Calabrese G, Cecchi L, Annesi-Maesano I, D’Amato G. The impact of cold on the respiratory tract and its consequences to respiratory health. Clin Transl Allergy. 2018;8:20.
Hälinen AI, Salonen RO, Pennanen AS, Kosma VM. Combined respiratory effects of cold air with SO(2) or NO(2) in single 1-hour exposures of hyperventilating guinea pigs. Inhal Toxicol. 2000;12(8):693–713.
Acknowledgements
The authors acknowledge the contribution and collaboration of all those who participated in this study.
Funding
This study was supported by the Gansu Provincial Science and Technology Program Project (Key R&D Program) (20YF3FA027) and the Fundamental Research Funds for the Central Universities (lzujbky-2020-9).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Wan-cheng Zhang, Jiang-long Ling, Run-ping Zhang, Ji-yuan Dong, Li Zhang, Rentong Chen and Ye Ruan. The first draft of the manuscript was written by Wan-cheng Zhang and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the principles in the Declaration of Helsinki. The data used in this dissertation were inpatient data collected for administrative purposes and did not contain any identifiable personal information. The Institutional Review Board (IRB) at School of Public Health, Lanzhou University, granted exemptions from obtaining ethical approval and consent to participate because the data collected did not involve any direct or indirect identification of participants. The researchers ensured the privacy and confidentiality of the data throughout the study, adhering to the guidelines and regulations set forth in the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Spearman correlation between air pollutions and meteorological factors in Lanzhou, China, 2014–2020. Table S2. Relative risk (95% CI) of single-pollutant model results in hospital admissions with ALRI, pneumonia and bronchiolitis associated with a 10 µg/m3 increase in air pollutant concentrations with different lag days. Table S3. Relative risk (95% CI) of single-pollutant model results in hospital admissions with ALRI, pneumonia and bronchiolitis associated with a 10 µg/m3 increase in air pollutant concentrations with different lag days by gender. Table S4. Relative risk (95% CI) of single-pollutant model results in hospital admissions with ALRI, pneumonia and bronchiolitis associated with a 10 µg/m3 increase in air pollutant concentrations with different lag days by age. Table S5. Relative risk (95% CI) of single-pollutant model results in hospital admissions with ALRI, pneumonia and bronchiolitis associated with a 10 µg/m3 increase in air pollutant concentrations with different lag days by season. Table S6. Relative risk (95% CI) of ALRI, pneumonia and bronchiolitis hospitalizations associated with a 10 µg/m3 increase in air pollutant concentrations in single and two-pollutant models. Table S7. Relative risk (95% CI) in hospital admissions for ALRI, pneumonia and bronchiolitis associated with a 10μg/m3 increase in air pollutant concentrations in sensitivity analyses.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, W., Ling, J., Zhang, R. et al. Short-term effects of air pollution on hospitalization for acute lower respiratory infections in children: a time-series analysis study from Lanzhou, China. BMC Public Health 23, 1629 (2023). https://doi.org/10.1186/s12889-023-16533-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16533-7