
Abstract
Background
Existing evidence suggests that children and adolescents who had experienced childhood maltreatment (CM) are at higher suicidal risk. However, the mediation role of resilience in this association remains unclear. We aim to investigate the mediation via resilience in the associations between CM and three suicidal risk indicators (suicidal ideation, SI; suicidal plan, SP; suicidal attempt, SA) among a large sample of Chinese children and adolescents.
Methods
A population-based cross-sectional survey was conducted in southwestern China Yunnan province. A total of 9723 children and adolescents were included and analyzed by using a multi-stage stratified cluster sampling design. Univariate and multivariate logistic regression models were fitted to explore the associations between CM, resilience, and the three suicidal risk indicators, dose-response trends further elucidated by using the restricted cubic splines. Path models were adopted to estimate the mediation of resilience.
Results
The estimated prevalence rates for one-year SI, SP and SA were 32.86% (95% CI: 31.93–33.80%), 19.36% (95% CI: 18.57–20.16%) and 9.07% (95% CI: 8.51–9.66%). After adjustment, CM significantly associated with all 3 suicidal risk indicators, and the odds ratios (ORs) were 2.13 (95% CI: 1.91–2.37), 2.45 (95% CI: 2.13–2.81), and 3.61 (95% CI: 2.90–4.52) for one-year SI, SP, and SA, respectively. Path models revealed that resilience significantly mediated the associations between CM and the three suicidal risk indicators, and among all dimensions of resilience, family support presented the strongest mediation consistently.
Conclusions
Our study results suggest that intervention measures which focusing on improving psychological resilience might be effective in reducing suicidal risk for children and adolescents who had experienced maltreatment. Prospective studies should be done to corroborate our findings.
Similar content being viewed by others


Introduction
Although suicide rates had declined prominently in recent years, suicide remains a leading cause of death [1, 2]. Compared to other age groups, children and adolescents are at higher risk of suicide, emphasizing the fact that more attention should be paid to this vulnerable age group [2,3,4]. The ideation-to-action framework proposed by Klonsky et al. stresses on a continuous developmental process of suicide starts from suicidal ideation (SI), via suicidal plan (SP) and suicidal attempt (SA), ends with completed suicide [5,6,7,8]. It has been well validated that SI, SP and SA are important indicators for imminent suicide [9, 10].
Currently available evidence suggests prominent association between adverse childhood experiences, particularly childhood maltreatment (CM), and the increased suicidal risk [11, 12]. Studies showed that at least one in four maltreated youths reported a history of SI, SP, or SA [13]. A meta-analysis of young people demonstrated that CM was associated with as much as 2.5-fold odds of SI, and 3.38-fold odds of SA [14]. However, direct intervention on CM has been proved costly, hard to implement, and less effective [15, 16]. Under this circumstance, finding other modifiable mediating factors which lie in the association between CM and suicide, could be a plausible way in reducing CM related suicide among youths.
Resilience has attracted considerable study interest in the field of positive psychology recently [17]. The American Psychological Association defines resilience as “the process of adapting well in the face of adversity, trauma, tragedy, threats or even significant sources of stress” [18]. Resilience is a multidimensional definition contains goal concentration, emotion regulation, positive perception, family support and interpersonal assistance [19]. Some previously published studies suggest that a higher level of resilience was associated with decreased risk of suicidal behaviors in youths [20,21,22]. Meanwhile, both cross-sectional and longitudinal studies have shown that children and adolescents who had experienced CM were observed a lower level of resilience [23, 24]. Therefore, it is reasonable to suspect that resilience plays as a significant mediator in the CM-suicide association. After extensive literature searching, we only identified two studies that investigated the mediation of resilience in the association between CM and SI [24, 25], whereas for the other two important suicidal risk indicators, SP and SA, no pertinent studies have been published.
In the present study, by using a large representative sample of Chinese children and adolescents, we intend to estimate the possible mediation of resilience in the association between CM and suicidal risk indicators. Specifically, the two primary hypotheses will be tested: (1) Resilience significantly mediates the associations between CM and suicidal risk indicators; (2) Different dimensions of resilience discordantly mediate the above associations. The major findings of this study can shed light in constructing effective intervention strategies and measures in reducing CM associated suicidal risk in children and adolescents.
Materials and methods
Study design and procedure
A cross-sectional survey was conducted in Zhenxiong, Yunnan Province, China, from May 9 to 31, 2021. Study subjects were determined by using a multi-stage stratified cluster sampling method with probability proportionate to sample size (PPS) design. First, 6 counties/streets were randomly chosen from all administrative areas in Zhenxiong; second, a certain number of schools based on pre-calculated sample size were randomly selected within each of the chosen counties/streets; finally, 2–4 classes from each grade within the chosen schools were randomly determined, and all eligible students within the chosen classes were included for survey. Exclusion criteria for study subjects include: (1) Aged below 10 years, for only children aged 10 years or above can fully understand the concept and consequence of suicide [26]; or (2) Aged 18 years or above; or (3) Had difficulties in hearing or communication; or (4) Refused to participate. For sample size calculation, we conservatively set the prevalence of suicidal risk at 30%, with an acceptable error of 1.2% and effective response rate of 90%, resulting in an initial sample size of 6225. Considering that sampling error for cluster sampling is greater than simple random sampling, the design effect was set at 1.5, which confirmed the required sample size of 9338. In the end, altogether 9969 eligible study subjects were included.
The survey contains two phases. In the first phase, all eligible study subjects were required to fill in self-administered questionnaires. After completion, finished questionnaires will be carefully checked by pre-trained quality control personnels deployed at the site, who were postgraduates in public health from Kunming Medical University. The second phase is clinical diagnosis. Respondents who were screened positive in the first phase will be face-to-face interviewed by professional pediatric psychiatrists to see whether a clinical diagnosis can be reached. More details regarding to this two-phase survey process can be referred to in our previous paper [27]. In this study, we only used database collected in the first phase. The study protocol was reviewed and approved by the Ethnics Review Committee of Kunming Medical University. Prior to the survey, written informed consents were obtained from both the participants and their legal guardians.
Measurements
A comprehensive structured self-administered questionnaire was used for collecting information from the study subjects. The questionnaire contains multiple modules. The modules that used for analyses in this study were: general characteristics, suicidal risk indicators, CM, resilience, depression and anxiety.
General characteristics
This part was self-developed, only contains factual questions like demographics (sex, age, ethnicity, whether single child, whether left-behind children), family features (parental marital status, education levels of the parents), etc. Left-behind children (LBC) was defined as children who are under 18 years old, with one or both of the parents migrated to other places for work, and the separation exceeded a consecutive 6 months in the past year [28].
Suicidal risk indicators
One-year SI, SP, SA were measured by the Suicide Behaviors Questionnaire-Revised (SBQ-R) [29]. One-year SI, SP and SA were measured using the following three separate questions: “How often have you thought about killing yourself in the past year?”, “How often have you planned to end your life in the past year?”, and “How often have you attempted to suicide but failed in the past year?”. Respondents who answered “1 time” or more frequent were considered positive (the answers included: never, 1 time, 2 times, 3–4 times, 5 times and above). In this study, the Cronbach’s α of SBQ-R was 0.815 (Bootstrap 95% CI: 0.805–0.824).
CM
The 28-item Childhood Trauma Questionnaire (CTQ) was developed by Bernstein, which retrospectively accesses CM experiences [30]. This instrument contains five types of CM: physical and emotional abuse, physical and emotional neglect, sexual abuse. Each question of the CTQ is scored on a five-point Likert scale from “never true” (1 point) to “very often true” (5 points), with a higher combined score reflects severer exposure of CM. The Chinese version of the CTQ had demonstrated satisfactory internal consistency [31, 32]. In our study sample, the Cronbach’s α was 0.747 (Bootstrap 95% CI: 0.739–0.756).
Resilience
Resilience of study subjects was estimated by the Resilience Scale for Chinese Adolescents (RSCA) that had been previously validated [19]. The RSCA has 27 items that can be classified into five dimensions (goal concentration, emotion regulation, positive perception, family support, interpersonal assistance). All questions can be rated from ‘totally disagree” (1 point) to ‘‘totally agree’’ (5 points), with a higher total score indicates a higher level of resilience. When considering resilience as a dichotomous variable, we choose the median (RSCA score: 87) as the cut-off. The Cronbach’s α for RSCA in our analytical sample was 0.848 (Bootstrap 95% CI: 0.843–0.853).
Depression and anxiety
The Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder Assessment (GAD-7) were used for gauging two-week depressive and anxiety symptoms [33, 34]. Both instruments had been well-validated in children and adolescents [35, 36]. A cut-off of 10 was recommend for screening medium and above depression and anxiety of clinical diagnostic significance [33, 34]. The Cronbach’s α of PHQ-9 and GAD-7 were 0.867 (Bootstrap 95% CI: 0.862–0.873) and 0.888 (Bootstrap 95% CI: 0.883–0.893) in this study.
Statistical analysis
General characteristics of participates were presented by descriptive statistics. Associations between CM, resilience, and suicidal risk indicators were estimated by using univariate and the subsequent multivariate logistic regression models. In multivariate model, important demographics (age, sex, ethnicity, place of residence, etc.), family features (parental marital status, whether single child, whether left-behind children, etc.), depressive and anxiety symptoms were controlled for, considering that they might be prominent confounders [37, 38]. Dose-response trends between CM, resilience and the suicidal risk indicators were estimated and visualized by using restricted cubic splines (RCSs) with four knots. A series of path models were fitted to evaluate the mediating role of resilience in the associations between CM and suicidal risk indicators: when the two paths from CM to resilience and from resilience to a specific suicidal risk indicator are statistically significant, the mediation via resilience exists, and the proportion of mediation is measured by the indirect association (calculated as the multiplication of the two path coefficients) divided by the total association (the sum of direct and indirect association). The statistical significance was set as a two-tailed p < 0.05, except for p < 0.10 in univariate logistic regressions. All data management and statistical analysis were performed in R software (Version: 4.3.1, Vienna, Austria), mainly used “lavaan” and “rms” packages.
Results
General characteristics of study subjects
For all the 9969 eligible subjects that initially included and approached, 131 refused to participate in the survey, 115 were further deleted because of missing information in key analytical variables, in the end 9723 eligible students with complete data were included into the final analysis, with a valid response rate of 97.53%. As shown in Table 1, for demographic characteristics, 4792 (49.29%) were boys, the mean of age was 14.02 years, 9151 (94.12%) were ethnical majority (Han), 6926 (71.23%) were from rural areas, and more than a half (53.84%) of the respondents were LBCs. Among all suicidal risk indicators, the highest prevalence was observed for one-year SI at 32.86% (95% CI: 31.93–33.80%), followed by one-year SP at 19.36% (95% CI: 18.57–20.16%), and one-year SA at 9.07% (95% CI: 8.51–9.66%). Students who were at any kind of suicidal risk had a higher score of CM and a lower score of resilience.
Associated factors of suicidal risk indicators
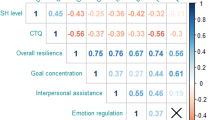
Univariate and multivariable binary logistic regression models were used to identify associated factors of the three suicidal risk indicators, and the results were jointly displayed in Table 2. Among all controlled covariates, sex, depression and anxiety showed consistent prominent association with SI, SA and SP, girls and subjects with higher PHQ-9 or GAD-7 score were observed higher suicidal risk. After controlled for covariates, children and adolescents with severer CM experience, as measured by CTQ scores, were observed increased suicidal risk: the ORs for one-year SI, SP, and SA were 2.13 (95% CI: 1.91–2.37), 2.45 (95% CI: 2.13–2.81), and 3.61 (95% CI: 2.90–4.52), respectively. On the contrary, resilience was inversely associated with suicidal risk indicators: the ORs for one-year SI, SP, and SA were 0.47 (95% CI: 0.42–0.52), 0.40 (95% CI: 0.35–0.46;), and 0.36 (95% CI: 0.29–0.45) in children and adolescents with higher resilience level.
We further estimated dose-response trend in their associations with suicidal risk indicators for CM and resilience by using the RCS curves: both CM and resilience showed significant dose-response associations with all three suicidal risk indicators (p for all non-linearity < 0.05) with a distinct “seesaw” pattern, along with the increase of resilience, the OR of suicidal risk consistently decreased, whereas exactly the opposite for CM associated suicidal risk (Fig. 1).

Dose-response association for childhood maltreatment, resilience and suicidal risk indicators illustrating by restricted cubic spline, adjusted for sex, age, place of residence, depression, and anxiety
Mediation of resilience in CM associated suicidal risk
Based on the above analytical results, together with additional analysis which identified statistically significant association between resilience and suicidal risk indicators (see in supplementary material, Table S1), it is reasonable to suspect mediation via resilience in the associations between CM and suicidal risk indicators. Hence, we fitted a series of path models to test this hypothesis. The analytical results showed that, resilience accounted for 33.91% of the total association between CM and one-year SI, 22.55% of the total association between CM and one-year SP, 9.72% of the total association between CM and one-year SA (Fig. 2). As to the five dimensions of resilience, family support played the most prominent mediation, accounted for 24.03% of CM associated one-year SI, 16.75% of CM associated one-year SP, and 7.12% of CM associated one-year SA, followed by emotion regulation and interpersonal assistance (Fig. 3).

Path analysis results for mediation of resilience. Standardized path coefficients were provided. Analyses were adjusted for sex, age, place of residence, depression, and anxiety

Mediation proportions by dimensions of resilience in the associations between childhood maltreatment and suicidal ideation (A), suicidal plan (B) and suicidal attempt (C)
Discussion
In this population-based cross-sectional study, we further corroborated the relationship between CM and suicidal risk among Chinese children and adolescents, more importantly, we revealed significant mediation by resilience in CM associated SI, SP and SA. Among all dimensions of resilience, family support consistently presented the strongest mediation. These major findings may suggest intervention measures which aiming at enhancing resilience, especially those concentrating on repairing or boosting family support, could be effective in reducing suicidal risk for youths who are victims of child abuse.
In our analytical sample, we observed the prevalence rates of one-year SI, SP, and SA were 32.86%, 19.36%, and 9.07%, moderately higher than some previous studies, probably can be ascribed to different measurement tools, study populations, and timeframes [39,40,41,42]. Among all controlled covariates, we found that girls, study subjects with higher depression or anxiety level were at increased suicidal risk, and the above findings are similar to previous publications [25, 37, 38, 43]. Meanwhile, the positive association between CM and suicidal risk that we identified in the present study is also consistent with existing literatures [16, 44]. Some mechanisms might be involved in explaining CM associated suicidal risk. For instance, the diathesis-stress model suggests that individuals with CM experiences can be more vulnerable to suicidal behaviors [45]. From the perspective of neurobiological mechanisms, CM may reduce serotonin function [46], or decrease oxytocin [47, 48], or adversely affect the hypothalamic-pituitary-adrenal axis and cortisol levels [49], leading to emotional dysregulation and suicidal behaviors.
Path analysis revealed that resilience significantly mediated the relationship between CM and the three suicidal risk indicators. Some published studies have already suggested prominent mediation by resilience in the association between CM and SI, for instance, Chen et al. demonstrated that resilience mediated 39.8% of the CM-lifetime SI association [25], Yang et al. found school connectedness and resilience as chain mediators partly mediated the link between CM and one-week SI [24]. The current study further suggest this mediation by resilience in CM associated SA and SP. Our findings highlight the promising role of resilience-centered intervention in reducing future suicidal risk for children and adolescents who suffered from CM, given the fact that feasible and effective program in enhancing resilience for children and adolescents are already available. For instance, school-based group intervention that emphasizing on emotional, cognitive and behavioral skills revealed a significant increase in resilience of adolescents [50]. Seven sessions of cognitive therapy for young people proved a long-term improvement in resilience when compared with controls [51]. Nevertheless, the effectiveness of these interventions to foster resilience among children and adolescents who are victims of CM requires further validation.
Another important finding was that among all dimensions of resilience, family support presented as the strongest mediator in CM associated suicidal risk. In our previous studies, emotion regulation, another dimension of resilience, has been identified the leading mediator for self-harm associated suicidal risk, and CM associated self-harm among Chinese children and adolescents [21, 52]. As to the reason why CM victims who reported comparatively higher level of family support were seen lower suicidal risk invites further investigation. Under any circumstance, this finding probably suggests that resilience intervention measures which focusing on cultivating family support could be of particular help in preventing CM associated suicide, such as the FOCUS program, or parent education plan [53, 54].
Among other dimensions of resilience, significant mediation has also been found for emotion regulation and interpersonal assistance. A longitudinal association between CM experience and lower adaptive emotion regulation in children and adolescents has been validated [55], researchers also found that maltreatment during childhood negatively affected interpersonal relationships, especially peer relationship [56, 57]. It has been recognized that both emotional dysregulation and malfunctional peer relationship can contribute to increased suicidal risk in youths [58, 59]. Therefore, targeted intervention measures which concentrating on improving emotional regulation ability or repairing peer relationship, such as mindfulness training and peer support program, might also be effective in reducing CM related suicidal risk in children and adolescents [60, 61].
There are several strengths of our study. First, population-based sampling design consolidates the representativeness of study subjects. Second, elaborate analytical strategy elucidates the robustness of our results. However, the following limitations should be noticed: the cross-sectional nature of this study undoubtedly hinders causal inference; information bias is unavoidable due to report and recall bias; generalization to the entire Chinese child and adolescent population should be prudent, as our study subjects were chosen from a single province in China; meanwhile, our analytical sample did not exclude individuals with any mental disorders diagnosed in phase 2 interview, although the proportion is very small (441/9723), it may also bring bias into our results. Future longitudinal studies with more representative sample and considering psychiatric disorders diagnosis are needed to further validate our findings.
Conclusions
In the current population-based cross-sectional study, we further corroborated the association between CM experiences and increased suicidal risk in Chinese children and adolescents, more importantly, we identified a significant mediation by resilience in this association, particularly the dimension of family support. Our findings probably suggest that intervention measures which targeting at enhancing resilience could be effective in reducing suicidal risk for children and adolescents who are victims of CM. Future studies of prospective design and contain more representative child and adolescent populations are needed for validation of our major findings.
Data availability
The datasets analyzed for the current study are available from the corresponding author under reasonable request.
References
Fadel SA, Boschi-Pinto C, Yu S, Reynales-Shigematsu LM, Menon GR, Newcombe L, et al. Trends in cause-specific mortality among children aged 5–14 years from 2005 to 2016 in India, China, Brazil, and Mexico: an analysis of nationally representative mortality studies. Lancet. 2019;393(10176):1119–27. https://doi.org/10.1016/S0140-6736(19)30220-X.
WHO, Suicide. https://www.who.int/news-room/fact-sheets/detail/suicide. Accessed 23 July 2023.
Dervic K, Brent DA, Oquendo MA. Completed suicide in childhood. Psychiatr Clin North Am. 2008;31(2):271–. https://doi.org/10.1016/j.psc.2008.01.006. 91.
Glenn CR, Kleiman EM, Kellerman J, Pollak O, Cha CB, Esposito EC, et al. Annual Research Review: a meta-analytic review of worldwide suicide rates in adolescents. J Child Psychol Psychiatry. 2020;61(3):294–308. https://doi.org/10.1186/s12889-021-12153-110.1111/jcpp.13106.
Klonsky ED, May AM. Differentiating suicide attempters from suicide ideators: a critical frontier for suicidology research. Suicide Life Threat Behav. 2014;44(1):1–5. https://doi.org/10.1186/s12889-021-12153-110.1111/sltb.12068.
Klonsky ED, May AM, Saffer BY, Suicide. Suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. 2016;12:307–30. https://doi.org/10.1186/s12889-021-12153-110.1146/annurev-clinpsy-021815-093204.
Zhong BL, Chan SSM, Liu TB, Chiu HF. Nonfatal suicidal behaviors of Chinese Rural-to-urban migrant workers: attitude toward suicide matters. Suicide Life Threat Behav. 2019;49(5):1199–208. https://doi.org/10.1111/sltb.12519.
Zhong BL, Ruan YF, Xu YM, Chen WC, Liu LF. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: a multi-center cross-sectional study. J Affect Disord. 2020;260:26–31. https://doi.org/10.1016/j.jad.2019.09.011.
Grundsøe TL, Pedersen ML. Risk factors observed in health care system 6 months prior completed suicide. Int J Circumpolar Health. 2019;78(1):1617019. https://doi.org/10.1186/s12889-021-12153-110.1080/22423982.2019.1617019.
Zhong BL, Xie WX, Zhu JH, Lu J, Chen H. Prevalence and correlates of suicide attempt among Chinese individuals receiving methadone maintenance treatment for heroin dependence. Sci Rep. 2019;9(1):15859. https://doi.org/10.1038/s41598-019-52440-x.
Sahle BW, Reavley NJ, Li W, Morgan AJ, Yap MBH, Reupert A, et al. The association between adverse childhood experiences and common mental disorders and suicidality: an umbrella review of systematic reviews and meta-analyses. Eur Child Adolesc Psychiatry. 2022;31(10):1489–99. https://doi.org/10.1186/s12889-021-12153-110.1007/s00787-021-01745-2.
Dai J, Zhong BL, Xiang YT, et al. Internal migration, mental health, and suicidal behaviors in young rural Chinese. Soc Psychiatry Psychiatr Epidemiol. 2015;50(4):621–31. https://doi.org/10.1007/s00127-014-0985-y.
Duprey EB, Oshri A, Liu S. Developmental pathways from child maltreatment to adolescent suicide-related behaviors: the internalizing and externalizing comorbidity hypothesis. Dev Psychopathol. 2020;32(3):945–59. https://doi.org/10.1186/s12889-021-12153-110.1017/S0954579419000919.
Angelakis I, Austin JL, Gooding P. Association of Childhood Maltreatment with suicide behaviors among Young people: a systematic review and Meta-analysis. JAMA Netw Open. 2020;3(8):e2012563. https://doi.org/10.1186/s12889-021-12153-110.1001/jamanetworkopen.2020.12563.
van der Put CE, Assink M, Gubbels J, Boekhout van Solinge NF. Identifying Effective Components of Child Maltreatment interventions: a Meta-analysis. Clin Child Fam Psychol Rev. 2018;21(2):171–202. https://doi.org/10.1186/s12889-021-12153-110.1007/s10567-017-0250-5.
Weisenmuller C, Hilton D. Barriers to access, implementation, and utilization of parenting interventions: considerations for research and clinical applications. Am Psychol. 2021;76(1):104–15. https://doi.org/10.1186/s12889-021-12153-110.1037/amp0000613.
Chen M, Wang GY, Zhao HF, Wang CC, Zhou Y, Zhong BL. Psychological resilience and related factors among primary care workers in Wuhan, China: a cross-sectional study. Heliyon. 2024;10(11):e31918. https://doi.org/10.1016/j.heliyon.2024.e31918.
American Psychological Association. The road to resilience. https://www.apa.org/monitor/oct02/pp. Accessed 23 July 2023.
Hu Y, Gan Y. Development and psychometric validity of the resilience scale for Chinese adolescents. Acta Physiol Sinica. 2008;40(8):902–12. In Chinese.
Mirkovic B, Delvenne V, Robin M, Pham-Scottez A, Corcos M, Speranza M. Borderline personality disorder and adolescent suicide attempt: the mediating role of emotional dysregulation. BMC Psychiatry. 2021;21(1):393. https://doi.org/10.1186/s12888-021-03377-x.
Xiao Y, Liu F, Ran H, Deng W, Che Y, Fang D, et al. Resilience mediates the association between self-harm and suicidal ideation in Chinese left-behind children. BMC Public Health. 2021;21(1):2055. https://doi.org/10.1186/s12889-021-12153-1.
Peng C, Wang M, Cheng J, Tan Y, Huang Y, Rong F, et al. Association between internet addiction and suicidal ideation, suicide plans, and suicide attempts among Chinese adolescents with and without parental migration. Comput Hum Behav. 2021;125:106949. https://doi.org/10.1016/j.chb.2021.106949.
Topitzes J, Mersky JP, Dezen KA, Reynolds AJ. Adult resilience among Maltreated children: a prospective investigation of Main Effect and Mediating models. Child Youth Serv Rev. 2013;35(6):937–49. https://doi.org/10.1016/j.childyouth.2013.03.004.
Yang Y, Liu M, Cao N, Li X, Chen Z, Kelifa MO. School connectedness and psychological resilience as mediators in the relationship between childhood abuse and suicidal ideation among Chinese adolescents. Eur J Psychotraumatol. 2023;14(1):2172650. https://doi.org/10.1080/20008066.2023.2172650.
Chen X, Jiang L, Liu Y, Ran H, Yang R, Xu X, et al. Childhood maltreatment and suicidal ideation in Chinese children and adolescents: the mediation of resilience. PeerJ. 2021;9:e11758. https://doi.org/10.7717/peerj.11758.
Mishara BL. Conceptions of death and suicide in children ages 6–12 and their implications for suicide prevention. Suicide Life Threat Behav. 1999;29(2):105–18.
Xiao Y, Ran H, Fang D, Che Y, Peng J, Sun H, et al. Childhood maltreatment and depressive disorders in Chinese children and adolescents: a population-based case-control study. Asian J Psychiatr. 2022;78:103312. https://doi.org/10.1016/j.ajp.2022.103312.
Zhou F, Duan C. A review on left-behind children research. Population J. 2006;157(03):60 – 5. In Chinese. https://doi.org/10.16405/j.cnki.1004-129x.2006.03.012
Osman A, Bagge CL, Gutierrez PM, Konick LC, Kopper BA, Barrios FX. The suicidal behaviors Questionnaire-revised (SBQ-R): validation with clinical and nonclinical samples. Assessment. 2001;8(4):443–54. https://doi.org/10.1177/107319110100800409.
Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. 1994;151(8):1132–6. https://doi.org/10.1176/ajp.151.8.1132.
Zhao X, Zhang Y, Li L, Zhou Y. Evaluation on reliability and validity of Chinese version of childhood trauma questionnaire. Chin J Cli Rehabilitation. 2005;9(16):209–11. In Chinese.
Jiang WJ, Zhong BL, Liu LZ, Zhou YJ, Hu XH, Li Y. Reliability and validity of the Chinese version of the Childhood Trauma Questionnaire-Short Form for inpatients with schizophrenia. PLoS ONE. 2018;13(12):e0208779. https://doi.org/10.1371/journal.pone.0208779.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Mossman SA, Luft MJ, Schroeder HK, Varney ST, Fleck DE, Barzman DH, et al. The generalized anxiety disorder 7-item scale in adolescents with generalized anxiety disorder: Signal detection and validation. Ann Clin Psychiatry. 2017;29(4):227–A234.
Richardson LP, McCauley E, Grossman DC, McCarty CA, Richards J, Russo JE, et al. Evaluation of the Patient Health Questionnaire-9 item for detecting major depression among adolescents. Pediatrics. 2010;126(6):1117–23. https://doi.org/10.1542/peds.2010-0852.
Liang X, Chang W, Ran H, et al. Childhood maltreatment and suicidal ideation in Chinese children and adolescents: the mediating role of mindfulness. BMC Psychiatry. 2022;22(1):680. https://doi.org/10.1186/s12888-022-04336-w.
Xiao Y, Ran H, Fang D, Che Y, Donald AR, Wang S, et al. School bullying associated suicidal risk in children and adolescents from Yunnan, China: the mediation of social support. J Affect Disord. 2022;300:392–9. https://doi.org/10.1016/j.jad.2022.01.032.
Bete T, Birhanu A, Negash A, Yadeta E, Lemi M, Balcha T, et al. Suicidal ideation, attempt and associated factor among secondary school students in Harari regional state, Eastern Ethiopia. A multi-center cross-sectional study. Front Psychiatry. 2023;14:1069910. https://doi.org/10.3389/fpsyt.2023.1069910.
McCallum SM, Batterham PJ, Christensen H, Werner-Seidler A, Nicolopoulos A, Newton N, et al. Personality factors associated with suicidal ideation, plans and attempts in adolescents. J Affect Disord. 2022;310:135–41. https://doi.org/10.1016/j.jad.2022.05.010.
Uddin R, Burton NW, Maple M, Khan SR, Khan A. Suicidal ideation, suicide planning, and suicide attempts among adolescents in 59 low-income and middle-income countries: a population-based study. Lancet Child Adolesc Health. 2019;3(4):223–33. https://doi.org/10.1016/S2352-4642(18)30403-6.
Zhong BL, Ding J, Chen HH, et al. Depressive disorders among children in the transforming China: an epidemiological survey of prevalence, correlates, and service use. Depress Anxiety. 2013;30(9):881–92. https://doi.org/10.1002/da.22109.
Goldman-Mellor S, Allen K, Kaplan MS. Rural/Urban disparities in adolescent nonfatal suicidal ideation and suicide attempt: a Population-based study. Suicide Life Threat Behav. 2018;48(6):709–19. https://doi.org/10.1111/sltb.12390.
Gong M, Zhang S, Li W, Wang W, Wu R, Guo L, et al. Association between Childhood Maltreatment and suicidal ideation and suicide attempts among Chinese adolescents: the moderating role of depressive symptoms. Int J Environ Res Public Health. 2020;17(17):6025. https://doi.org/10.3390/ijerph17176025.
Brodsky BS. Early Childhood Environment and genetic interactions: the diathesis for suicidal behavior. Curr Psychiatry Rep. 2016;18(9):86. https://doi.org/10.1007/s11920-016-0716-z.
Roy A, Hu XZ, Janal MN, Goldman D. Interaction between childhood trauma and serotonin transporter gene variation in suicide. Neuropsychopharmacology. 2007;32(9):2046–52. https://doi.org/10.1038/sj.npp.1301331.
Jokinen J, Chatzittofis A, Hellström C, Nordström P, Uvnäs-Moberg K, Asberg M. Low CSF oxytocin reflects high intent in suicide attempters. Psychoneuroendocrinology. 2012;37(4):482–90. https://doi.org/10.1016/j.psyneuen.2011.07.016.
Pierrehumbert B, Torrisi R, Laufer D, Halfon O, Ansermet F, Beck Popovic M. Oxytocin response to an experimental psychosocial challenge in adults exposed to traumatic experiences during childhood or adolescence. Neuroscience. 2010;166(1):168–77. https://doi.org/10.1016/j.neuroscience.2009.12.016.
De Bellis MD. The psychobiology of neglect. Child Maltreat. 2005;10(2):150–72. https://doi.org/10.1177/1077559505275116.
Hatamizadeh N, Adibsereshki N, Kazemnejad A, Sajedi F. Randomized trial of a resilience intervention on resilience, behavioral strengths and difficulties of mainstreamed adolescent students with hearing loss. Int J Pediatr Otorhinolaryngol. 2020;128:109722. https://doi.org/10.1016/j.ijporl.2019.109722.
Konradt CE, Cardoso TA, Mondin TC, Souza LDM, Kapczinski F, da Silva RA, et al. Impact of resilience on the improvement of depressive symptoms after cognitive therapies for depression in a sample of young adults. Trends Psychiatry Psychother. 2018;40(3):226–31. https://doi.org/10.1590/2237-6089-2017-0047.
Tian X, Lu J, Che Y, Fang D, Ran H, He X, et al. Childhood maltreatment and self-harm in Chinese adolescents: moderation and mediation via resilience. BMC Public Health. 2021;21(1):1561. https://doi.org/10.1186/s12889-021-11605-y.
Saltzman WR. The FOCUS Family Resilience Program: an innovative family intervention for trauma and loss. Fam Process. 2016;55(4):647–59. https://doi.org/10.1111/famp.12250.
To SM, Kwok CM, So YY, Yan MW. Parent education for migrant mothers of left-behind children in China: a pilot randomized controlled trial. Fam Process. 2019;58(2):318–33. https://doi.org/10.1111/famp.12369.
Kim SG, Weissman DG, Sheridan MA, McLaughlin KA. Child abuse and automatic emotion regulation in children and adolescents. Dev Psychopathol. 2023;35(1):157–67. https://doi.org/10.1017/S0954579421000663.
Lin X, Li L, Chi P, Wang Z, Heath MA, Du H, et al. Child maltreatment and interpersonal relationship among Chinese children with oppositional defiant disorder. Child Abuse Negl. 2016;51:192–202. https://doi.org/10.1016/j.chiabu.2015.10.013.
Yoon D. Peer-relationship patterns and their association with types of child abuse and adolescent risk behaviors among youth at-risk of maltreatment. J Adolesc. 2020;80:125–35. https://doi.org/10.1016/j.adolescence.2020.02.008.
Colmenero-Navarrete L, García-Sancho E, Salguero JM. Relationship between emotion regulation and suicide ideation and attempt in adults and adolescents: a systematic review. Arch Suicide Res. 2022;26(4):1702–35. https://doi.org/10.1080/13811118.2021.1999872.
Sultana M, Gow J, Mosharaf P, Rahman H, Koly KN, Rahman MA, et al. Parental role and peer support in adolescent suicidal behavior in eight South-East Asian countries. J Affect Disord. 2023;332:221–30. https://doi.org/10.1016/j.jad.2023.03.092.
García-Rubio C, Herrero M, Luna-Jarillo T, Albert J, Rodríguez-Carvajal R. Effectiveness and mechanisms of change of a mindfulness-based intervention on elementary school children: a cluster-randomized control trial. J Sch Psychol. 2023;99:101211. https://doi.org/10.1016/j.jsp.2023.04.001.
van der Meulen K, Granizo L, Del Barrio C. Emotional peer support interventions for students with SEND: a systematic review. Front Psychol. 2021;12:797913. https://doi.org/10.3389/fpsyg.2021.797913.
Acknowledgements
Not applicable.
Funding
This study was support by the Union Project of Yunnan Science and Technology Bureau and Kunming Medical University (202401AY070001-001), National Natural Science Foundation of China (82360670, 72264019, 82060601).
Author information
Authors and Affiliations
Contributions
YX (Yuanyuan Xiao) conceptualized the study. HR, DF, YC, YH, SL and GZ collected carried out data collection. JP, JL and YX (Yi Xiang) performed data analysis and visualization. JP and WC prepared the draft manuscript. YX (Yuanyuan Xiao) and JL critically revised the manuscript. All authors had read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its subsequent revisions or similar ethical standards. The study protocol was reviewed and approved by the Ethics Review Committee of Kunming Medical University. Informed consent was provided by the participants and their legal guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, J., Chang, W., Ran, H. et al. Childhood maltreatment associated suicidal risk in Chinese children and adolescents: a mediation of resilience. BMC Public Health 24, 2114 (2024). https://doi.org/10.1186/s12889-024-19629-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19629-w