
Abstract
Background
Poor psychological well-being, including depression, anxiety, and low self-esteem, is both prevalent among young South Africans living with HIV and associated with poor HIV clinical outcomes. By impacting food insecurity and employment, the COVID-19 pandemic may have influenced psychological well-being in this population. This analysis sought to examine whether food insecurity and unemployment mediated the relationship between study cohort (pre- versus during-pandemic) and psychological well-being in our sample of young South Africans living with HIV.
Methods
This was a secondary analysis comparing baseline data from two cohorts of young South Africans ages 18–24 from the Cape Town and East London metro areas who tested positive for HIV at clinics (or mobile clinics) either before or during the COVID-19 pandemic. Baseline sociodemographic, economic, and psychological outcomes were analyzed through a series of bivariate logistic regression and mediation analyses. All data were analyzed in 2023 and 2024.
Results
Reported food anxiety, insufficient food quality, and insufficient food quantity were lower in the cohort recruited during the COVID-19 pandemic than those recruited before the pandemic (p < 0.001). Higher levels of food insecurity predicted higher depressive and anxiety symptoms and lower self-esteem. Food anxiety, insufficient food quality, and insufficient food quantity, but not unemployment, mediated the relationship between study cohort and depressive symptoms, anxiety symptoms, and self-esteem.
Conclusion
Food insecurity may have decreased amongst our sample of young people during the COVID-19 pandemic. Our findings build on our understanding of how the psychological well-being of young people living with HIV was affected by the COVID-19 pandemic and may lend support to interventions targeting food insecurity to improve psychological well-being in this population.
Similar content being viewed by others


Introduction
With more than 150,000 new infections per year [1], South Africa is home to the world’s largest population of people living with HIV (PLWH) [2]. Compared to other age cohorts, adolescents and young adults (AYA) experience worse HIV clinical outcomes, including high mortality rates [3] and lower rates of antiretroviral therapy initiation [4], antiretroviral adherence [5, 6] and viral suppression [4, 6]. In addition to navigating an inherent set of challenges related to the transition from childhood into adulthood (i.e. becoming self-sufficient, engaging in identity formation) [7,8,9], AYA living with HIV face disproportionate socioeconomic (lack of economic independence, difficulty accessing clinics), and psychological (difficulty adapting to sustained medication, higher rates of stigma), barriers that may complicate HIV care initiation and antiretroviral therapy (ART) adherence [5, 10]. These barriers may not only contribute to poor HIV clinical outcomes but may also manifest in the high rates of poor psychological well-being observed among AYA living with HIV [11,12,13,14,15,16]. A particularly acute barrier recently faced by AYA was national lockdowns due to COVID-19, which may have further contributed to poor psychological outcomes in this population.
Indeed, the psychological well-being of AYA living with HIV may have been further impacted by the numerous disruptions related to the COVID-19 pandemic and subsequent infection control measures [17–18], which disrupted access to mental health care, social support networks, and employment opportunities [19,20,21,22,23]. These effects may have been particularly pronounced in South Africa, which in March 2020 instituted a stringent lockdown involving the banning of nonessential travel outside of the home, the closure of schools and businesses, and a prohibition on all public gatherings [24, 25]. The initial five-week lockdown was followed by the implementation of a staged system of social and economic restrictions that ended only in April 2022 and whose stringency depended on provincial rates of COVID-19 infection. The economic toll of the lockdown measures included the loss of an estimated 3 million jobs [26], predominantly affecting South Africans from key and vulnerable populations, including PLWH [27,28,29]. Given both AYA with HIV’s high pre-pandemic baseline levels of food insecurity and unemployment [30,31,32] and the disproportionate effect of COVID-19-related employment losses on young South Africans [33], there is therefore reason to believe that measures of socioeconomic vulnerability, such as food insecurity and unemployment, may have increased among young PLWH during the pandemic.
Social stress theory (SST) provides a useful framework for understanding how macrolevel economic processes occurring during the pandemic may have influenced stress processes at the individual level, thus promoting differential levels of psychological well-being across social groups [34]. According to the social stress framework, economic disturbances, such as those experienced during the COVID-19 pandemic, may lead to individually experienced life-events (unemployment, food insecurity) that in turn may promote psychological stress. These macrolevel processes are thought to provoke psychological stress primarily through social and structural factors, potentially through dependency on income for survival and the negative effects of disadvantaged social status [35]. However, social stress theory also holds that the degree to which these economic disruptions promote poor psychological and social functioning depends greatly on the distribution of social vulnerabilities; that is, the relationship between economic disruption and psychological distress is moderated greatly by one’s health, sociodemographic, and other personal characteristics (e.g., physical health, gender, and ability to cope). Based on social stress theory, our study sampled young South African adults who were newly diagnosed with HIV, who were posited to be at particular risk of poor psychological outcomes related to COVID-19 induced disturbances.
To our knowledge, there have been a dearth of studies evaluating the socioeconomic vulnerability of AYA living with HIV during the COVID-19 pandemic. While several studies have elucidated the effect of social distancing and isolation on depression and anxiety [36,37,38], few have evaluated the degree to which COVID-19-related economic disruptions affected psychological functioning in youth living with HIV. Considering that depression [39], anxiety [40], and self-esteem [41] have been found to be directly associated with worse HIV clinical outcomes, it is critical to understand the broader structural forces affecting psychological and social functioning in AYA living with HIV during the COVID-19 pandemic.
To determine the relationships among the COVID-19 pandemic, individual socioeconomic variables, and psychological well-being of AYA ages 18–24 living with HIV, this secondary analysis sought to (1) compare levels of food insecurity and unemployment between cohorts of AYAs newly diagnosed with HIV either before (2018–2019) or during the COVID-19 pandemic (2020–2022) ; (2) determine whether key baseline demographic factors are predictors of individual socioeconomic variables such as food insecurity and unemployment; and (3) determine whether food insecurity and unemployment mediated the relationship between time of diagnosis in relation to the COVID-19 pandemic and psychological well-being. In particular, we hypothesized that relative to AYA diagnosed with HIV before the pandemic, those diagnosed during the pandemic would exhibit higher levels of food insecurity and unemployment. In addition, based on SST’s premise that macrolevel economic disruptions can provoke psychological distress, we hypothesized that food insecurity and unemployment would significantly mediate the relationship between time of diagnosis and psychological well-being in this population.
Methods
Population
The data for this secondary analysis come from a sequential prospective cohort study conducted in 2018–2019 and a subsequent pilot randomized controlled trial conducted in 2020–2022, which was conducted as part of a larger study called Standing Tall (NIH 1R34MH114897-01A1). The first study was conducted in Cape Town in, and the second study was conducted in Cape Town and East London, South Africa. Both studies recruited 100 newly diagnosed HIV positive participants aged 18–24 years. The data for these analyses were drawn from baseline surveys, which were conducted at the time of enrollment in both studies.
Participants in the first study were recruited from community-based centers and well-established mobile clinics operating in and around several communities in Cape Town. The mobile clinics offered a variety of services including family planning, HIV testing and counseling, and STI testing and treatment. Participants in the second study were recruited from the same mobile clinics operating in and around Cape Town, in addition to three clinics in the East London area.
To be eligible for participation in the studies, individuals had to present to mobile testing clinics or physical clinics and be newly diagnosed with HIV, be ART naïve, speak English and/or isiXhosa, and reside in the Cape Town or East London (for the second study) metro areas. Individuals were eligible for participation in the first study if they resided in out of five communities in the Western Cape (Langa, Mfuleni, Philippi, Dunoon, and Joe Slovo) whereas participants in the second study were eligible if they resided in either one of these five communities or two in East London (Gompo, Duncan Village). Individuals who were currently pregnant or diagnosed with TB disease, and persons under the age of 18 years were excluded. AYAs unable to understand the informed consent process were also excluded. Individuals in the pre-COVID cohort were recruited between 2018 and 2019 and those in the during-COVID cohort were recruited between 2020 and 2022.
This study was approved by the Partners Healthcare Institutional Review Board at Brigham and Women’s Hospital and Massachusetts General Hospital, Harvard Medical School, Boston, MA and the Human Research Ethics Committee at the University of Cape Town, South Africa and was conducted in compliance with applicable laws and regulations. Informed consent was obtained from all participants engaging in both studies. Written informed consent was obtained in isiXhosa and/or English, To facilitate understanding among participants, all consent forms were read aloud to participants in the language of their choice.
Measures
Primary predictors
Time of diagnosis in relation to the pandemic was the primary predictor in our mediation analyses. Based on the trial in which they participated, study participants were categorized into dichotomous pre- (2018–2019) and during-COVID (2020–2022) groups. While our sample size was not powered for a longitudinal analysis of trends across the pre-pandemic and intra-pandemic cohorts, all participants recruited in the pre- and post-pandemic cohorts were recruited before and during South Africa’s COVID-19 era National State of Disaster [37] such that our dichotomization accurately reflects diagnosis before or after COVID-19 related economic and social restrictions were implemented. While there was a degree of heterogeneity in the exact COVID-19 related economic and social restrictions implemented across the 2020–2022 period [42–43], data from the period does suggest that the economic effects of the COVID-19 pandemic lingered throughout the study period, with employment levels only recovering to pre-pandemic levels in late 2023 [44].
Additional dichotomous baseline characteristics included as predictor variables in our analysis included: age (≥ 21 years vs. <21 years), gender (male vs. female), education level (did not complete high school vs. completed high school) and living status (alone vs. with others). All o these variables were used as dichotomous predictor variables in our bivariate logistic regression analysis.
Psychological outcomes
Three psychological measures were assessed in this analysis.
-
1.
Depressive symptoms. The 9-question Patient Health Questionnaire (PHQ-9) was utilized to measure the severity of depressive symptomsOnly baseline measures were used in this study. The 9 items assess symptoms associated with the diagnosis of clinical depression. The PHQ-9 has validity and reliability when used among PLWH in sub-Saharan Africa [45]. Responses on each item range from 0 (‘not at all’) to 3 (‘nearly every day’). Higher scores reflect greater degrees of depressive symptoms, with scores ≥ 10 indicating moderate-severe depressive symptoms. In this analysis, we used the continuous PHQ-9 total score. Cronbach’s alpha for the PHQ-9 questionnaire was ⍺ = 0.920.
-
2.
Generalized anxiety symptoms. The 7-item Generalized Anxiety Disorder (GAD-7) Scale was used to identify symptoms of generalized anxiety disorder (GAD) and determine the severity of symptoms known to be associated with GAD [46]. The GAD-7 has demonstrated construct validity and reliability when used in the South African context [47]. Responses to each item range from 0 (‘not at all’) to 3 (‘nearly every day’), with total scores ranging from 0 to 21. Higher scores reflect a greater degree of anxiety symptoms, with scores ≥ 10 reflecting moderate-severe anxiety symptoms. In our analyses, continuous GAD-7 total scores were used. Cronbach’s alpha for the GAD-7 questionnaire was ⍺ = 0.886.
-
3.
Self-esteem. The Rosenberg Self-Esteem Scale (RSES) was used to evaluate individual self-esteem [48]. The RSES scale has demonstrated psychometric validity within the South African context [49]. All items are answered using a 4-point Likert scale with scores ranging from 1 (‘strongly disagree’) to 4 (‘strongly agree’). Five of the items, reflecting negative feelings about the self, are reverse scored and totaled with the other items to create a composite score. Total RSES scores were utilized as a continuous outcome variable throughout the study. Lower scores indicate higher degrees of self-esteem/self-efficacy. Cronbach’s alpha for the RSES questionnaire was ⍺ = 0.724.
Economic variables
Two measures of socioeconomic vulnerability were assessed at baseline.
-
1.
Food insecurity was divided into three separate domains, including food anxiety, insufficient quality, and insufficient quantity. Each of the items representing these three domains were taken from the Household Food Insecurity Access Scale (HFIAS), which asks respondents to recall whether they have experienced different aspects of food insecurity, including feelings of anxiety over food and perceptions that food is of insufficient quantity and quality (including diversity or nutritional preference), within a recall period of 30 days (4 weeks) [50]. The validity and reliability of the scale has been demonstrated in several diverse contexts [51,52,53]. All items are answered using a 4-point Likert scale format with answers ranging from 1 (‘never,’ i.e., 0 times a month ) to 4 (‘often,’ i.e., 10x or more per month), with total scores ranging from 3 to 12. Answers to each domain were dichotomized to create a binary variable presenting high (‘often,’ ‘sometimes’) or low (‘rarely,’ ‘never’) levels of anxiety, insufficient quality, and insufficient intake. In our logistic regression analysis, total food insecurity was dichotomized into high food insecurity (scores ≥ 6, indicating that the participant experienced food insecurity more than 1-2x in the past month) and low food insecurity (scores ≤ 6, indicating that the participant experienced food insecurity on average less than 1-2x in the past month).
-
2.
Employment status was treated as a categorical variable based on responses to the question ‘are you currently employed’?. In this analysis, employment was treated both as binned dichotomous variable (employed vs. unemployed).
Covariates
Our directed acyclic graph (DAG) analysis did not identify any covariates that could reasonably act as confounders of the relationship between time of diagnosis and our psychological outcomes of interest. Covariates analyzed via the DAG method included age, gender, education level, and living status.
Statistical analysis
Descriptive statistics were used to describe study participants’ baseline demographic and economic characteristics. For dichotomous characteristics, chi-square tests of association were conducted to determine whether a statistically significant association existed between time of diagnosis (pre- vs. during-COVID-19) and each demographic and economic characteristic (age, gender, education level, living status, employment, and food insecurity). For continuous characteristics, a two-sided independent sample t-test was utilized to evaluate whether means were statistically different between the two cohorts.
Following aggregation of the two datasets, bivariate logistic regression analysis was performed in which four dichotomous socio-demographic predictor variables (e.g., age, gender, living status, and education level) were used to predict dichotomous levels of food insecurity (high/low) and unemployment (yes/no). Odds ratios (OR) were calculated to determine the constant effect of our predictors on the likelihood of an outcome (i.e. having food insecurity or unemployment). The Wald test was used to determine the statistical significance of each of the predictor variables.
Mediation analyses, informed by Baron and Kenny [54], were conducted to test the mediation effect of each of our economic variables on the association between time of diagnosis and our four continuous psychological outcomes (see Fig. 1). First, the direct effect of time of diagnosis on each psychological outcome was determined (path c). Next, we determined whether time of diagnosis significantly predicted our mediator of interest (path a). Then, we determined whether our mediator of interest predicted our psychological outcome (path b). Finally, we determined if time of diagnosis remained a significant predictor of each psychological outcome after controlling for our mediator of interest (path c’). Full mediation occurs when the association between predictor and outcome is no longer statistically significant, whereas partial mediation occurs if the strength of association is reduced but still significant. The Sobel test was used to determine whether the mediating effects of each economic variable was statistically significant [55]. All data analyses were completed in the year 2024.
All analyses were conducted using SPSS 29.0.1.1.

Diagram of proposed mediation model
Results
All 200 of our participants identified as Black African and identified English or isiXhosa as their preferred language. The median age of the pre- and during-COVID cohorts were 22 (IQR: 19–23) and 21 (IQR: 19–22), respectively. Mean ages were similar in each study cohort (21.17 years in the pre-COVID cohort vs. 20.68 years in the during-COVID cohort, p = 0.078). Gender breakdown (χ2 = 0.207, p > 0.05), education level (χ2 = 0.322, p = 0.570), and living status (χ2 = 3.269, p = 0.071) was not significantly associated with time of diagnosis (Table 1).
In terms of economic characteristics of our two cohorts, there was no statistically significant association between employment status and time of diagnosis (χ2 = 1.339, p = 0.247). However, being diagnosed during the pandemic was significantly associated with less reported food anxiety (χ2 = 78.95, p < 0.001), less reported insufficient food quality (χ2 = 46.07, p < 0.001), and less insufficient food quantity (χ2 = 52.35, p < 0.001).
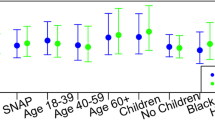
In bivariate regression analyses (Table 2), female participants had a 62.6% lower odds of reporting high food insecurity than male participants (OR 0.374, CI 0.156–0.899, p = 0.028). Female gender (OR 2.778, CI 1.088–7.095, p = 0.033) and living alone (OR 4.666, CI 1.793–12.138, p = 0.002) were associated with significantly greater odds of unemployment whereas completing high school was associated with significantly lower odds of unemployment (OR 0.333, CI 0.142, 0.784, p = 0.012).
Results from the mediation analyses evaluating the effect of our mediator on the relationship between our economic variables (food anxiety, insufficient food quality, and insufficient food quantity, and unemployment) and each of our three psychological outcomes are presented in Tables 3 and 4. Being diagnosed with HIV during the COVID-19 pandemic did not significantly predict depressive symptoms as measured by PHQ-9 scores (β = 0.214, p = 0.748) or anxiety symptoms as measured by GAD-7 scores (β = 0.325, p = 0.586). However, diagnosis during the COVID-19 pandemic did predict higher self-esteem, which was associated with lower RSES scores (β=-5.409, p = < 0.001) (Table 3).
Partial mediation of the relationship between time of diagnosis and PHQ-9 score was observed when food anxiety (Sobel z = -3.87, p < 0.001), insufficient food quality (Sobel z = -3.13, p = 0.0017), and insufficient food quality (Sobel z = -2.12, p = 0.034) were included in our regression model (Table 3). Similarly, food anxiety (z=-3.75, p < 0.001), insufficient food quality (-3.16, p = 0.0016), and insufficient food quantity (z=-2.61, p = 0.0091) all exhibited a partial mediation effect on the relationship between time of diagnosis and GAD-7 scores. In addition, partial mediation of the relationship between study cohort and self-esteem (RSES scores) were observed when food anxiety (Sobel z = -2.11, p = 0.035), insufficient food quality (Sobel z = -2.40, p = 0.017), and insufficient food quantity (Sobel z = -3.07, p = 0.002) were included in our model (Table 3).
Unemployment did not exhibit a significant mediation effect on the relationship between time of diagnosis and any of our psychological variables.
Discussion
The major aims of this analysis were to compare the socioeconomic vulnerability of a pre- and during-COVID-19 cohort of newly diagnosed AYA living with HIV and to determine whether measures of socioeconomic vulnerability mediated the relationship between time of diagnosis and psychological well-being. Although it was hypothesized that diagnosis during the COVID-19 pandemic would be associated with poorer socioeconomic vulnerability [20, 26], the results of our analyses of baseline food insecurity and unemployment demonstrated that diagnosis during the pandemic was associated with a significantly lower level of reported food anxiety, insufficient food quality, and insufficient food quantity. No association was found between time of diagnosis and unemployment.
Concordant with our predictions based on social stress theory, our mediation analyses revealed that higher levels of food insecurity significantly predicted higher levels of depressive symptoms, anxiety symptoms, and lower self-esteem. Although diagnosis during the pandemic predicted only higher self-esteem, lower levels of food insecurity were associated with better overall psychological functioning. On the other hand, unemployment was not a significant predictor of any of our psychological outcomes. Interestingly, our results thus suggest that food security may have a more profound impact on psychological outcomes than employment status in this population. On the whole, while our findings do not indicate a relationship between unemployment and poor psychological well-being in this population, they do lend support to a previously identified relationship between food insecurity and indicators of poor psychological well-being known to be related to HIV treatment outcomes [56–57].
Our results also add to our understanding of the understudied and likely complex relationships among the pandemic, macrolevel economic disruptions, and psychological outcomes among newly diagnosed young South Africans living with HIV. First, they suggest that at least among this population of urban youth newly diagnosed with HIV, reported food anxiety and insufficient food quality and quantity decreased during the COVID-19 pandemic, despite a background of increased unemployment [58, 59] and food insecurity in South Africa overall [28, 5860]. Though surprising, data collected by the South African government during the pre- and during-COVID-19 time periods does suggest some degree of heterogeneity in the effects of the pandemic on food insecurity, with some provinces experiencing greater food insecurity and others demonstrating declines during the pandemic [61].
Conceivably this lower food insecurity observed in our intra-pandemic cohort may be explained by the disproportionate insulating effect of pandemic-era government transfer payments on the income of poor, unemployed South Africans [59], who composed the majority of both of our cohorts. Indeed, in April 2020, South Africa’s government instituted both a series of existing grant top-ups in addition to a new Social Relief of Distress Grant of R350 ($21), which was offered to South Africans aged 18 and above who were already unemployed or who had lost employment due to the country’s lockdown [62]. Given that over 8 million economically vulnerable South Africans benefited from this 41 billion rand ($2.4 billion USD) social assistance package [63], it is plausible that the receipt of these grants had a particularly protective effect on our economically disadvantaged population of AYA. This increase in government support may have been complemented by both the efforts of local nongovernmental organizations, which engaged in extensive community outreach to alleviate intrapandemic food insecurity through the distribution of food and food vouchers [64–65], and a notable increase in household agricultural production during the COVID-19 pandemic [48]. Thus, while our results may point to the well-documented efficacy of South Africa’s robust system of unconditional cash transfer payments [58, 66,67,68,69] on hunger [70], nongovernmental and individual efforts may have also contributed to the decline observed within this population.
Our findings suggest that the decrease in food insecurity, whether through an expanded social safety net, nongovernmental support, or other means, may have had a protective effect on mental health outcomes during the COVID-19 pandemic. In doing so, our results not only align with a growing body of research suggesting an association between food insecurity and poor mental health outcomes [71,72,73], but also indicate that improvements in food security may have buffered against the psychological distress associated with the COVID-19 pandemic [74,75,76]. Put another way, whereas social stress theory predicts that limited economic resources may lead to increased distress and poor psychological health [34], our results suggest that the reverse may also be true: that lower levels of food insecurity may facilitate improved psychological functioning despite the presence of a globally significant macrolevel stressor. Interestingly, the mediating effect of declining food insecurity on psychological well-being was strongest for self-esteem, a psychological outcome for which an association with food insecurity has not been clearly established. While poverty in general has been shown to be negatively associated with self-esteem [77–78], further research is needed to identify the mechanism by which food security may affect one’s perception and confidence in oneself.
Overall, our results may lend further support for structural interventions, policies, and programs that improve access to quality food among people living with HIV. Although the impact of undernutrition and poor HIV clinical outcomes has been well-established [79,80,81], our results as well as those of a growing body of literature suggest that the benefits of improved food security may also extend to key indicators of mental health [72, 82,83,84]. Moreover, though there remains a dearth of best practice studies evaluating specific intervention strategies to address the HIV-food insecurity syndemic [85], initiatives that provide direct monetary or food assistance have demonstrated particular efficacy in improving food security in the sub-Saharan African context [86–87]. Thus, given the association of food insecurity with both poor physical and mental health outcomes in PLWH, such direct provision interventions may be especially potent in terms of their ability to improve multiple, overlapping domains of health.
Conclusion
Our results demonstrated that in our sample of newly diagnosed South African AYA living with HIV, time of diagnosis during the COVID-19 pandemic was significantly associated with lower levels of food anxiety and insufficient food quality and quantity. Moreover, the relationships between time of diagnosis and psychological outcomes such as depressive symptoms, anxiety symptoms, and self-esteem were significantly mediated by food insecurity. Our findings build on our understanding of how the psychological well-being of AYA living with HIV was affected by the COVID-19 pandemic and lend support to interventions targeting food insecurity as a means of improving psychological outcomes in this vulnerable population.
Strengths, limitations, and future directions
This study has several key strengths. For one, our study adds to our understanding of psychological well-being and socioeconomic vulnerability across the pandemic among AYA living with HIV. Indeed, the timing of our cross-sectional surveys, which were conducted among two demographically similar South African samples of AYA before and during the pandemic, allowed us to evaluate important trends in economic and psychological well-being across this important juncture in time. In this manner, our analyses focusing on AYA living with HIV permitted the identification of intrapandemic changes that may have been particular to this unique population, and that may not have been observed in samples taken from the general population of PLWH. Our study thus provides important insight into the ways in which the pandemic may have uniquely impacted psychological and economic correlates of well-being among this vulnerable, disproportionately HIV affected population.
Nevertheless, despite identifying a promising association between food security and mental health amongst AYA living with HIV, our study has several limitations. First, given our focus on young people from urban South Africa, our results may not be generalizable to all South African PLWH. In fact, our own results suggest that levels of food insecurity may have differed significantly among different sub-populations of AYA living with HIV, such as young HIV positive men. Moreover, our mediation analyses were conducted using data from two cross-sectional surveys, and therefore, the directionality of our proposed mediator to outcome pathway cannot be directly assessed. Additionally, the time of diagnosis was treated as a dichotomous variable based on the recruitment of our two cohorts, and our classification of groups into pre- and during-pandemic cohorts may have disguised trends in food insecurity and or unemployment that may have changed longitudinally throughout South Africa’s pandemic-era State of Disaster. Finally, while our cohorts were recruited using similar procedures and did not differ significantly in terms of key sociodemographic characteristics (gender, unemployment status, education level, etc.), it is possible that the during-COVID cohort may have differed on the basis of other unmeasured factors. Therefore, we cannot rule out the possibility it may be that these unique characteristics of the group recruited during the pandemic, rather than the pandemic itself, that explain the lower food insecurity observed.
While our study adds to the literature about recent trends in food insecurity in South Africa, additional retrospective analyses of the effects of pandemic-era policies are needed to determine to what degree, if any, mental health and HIV clinical outcomes were affected by the increased economic support provided to vulnerable South Africans during the country’s COVID-19 lockdown. Public policy analyses investigating the differential effects of South Africa’s COVID-19 social grant system on subpopulations of South African PLWH would also be helpful in elucidating why AYA living with HIV may have been particularly buffered from the economic effects of the COVID-19 pandemic in comparison with other populations. Finally, translational research is needed to better understand how interventions targeting food insecurity may impact psychological and HIV clinical outcomes among PLWH.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
UNAIDS. Country factsheets: South Africa. Geneva, Switzerland. https://www.unaids.org/en/regionscountries/countries/southafrica. Published 2024. Accessed January 31, 2024.
Statistics South Africa. Mid-year population estimates, 2022. Salvokop, Pretoria, South Africa. https://www.statssa.gov.za/?page_id=1854&PPN=P0302. Published 2022. Accessed January 31, 2024.
Zanoni BAM, Buchan S, Katz I, Haberer J. Systematic review and meta-analysis of the adolescent and young adult HIV continuum of care in South Africa: the cresting wave. BMJ Glob Health. 2016;1(3):e000004. https://doi.org/10.1136/bmjgh-2015-000004
Evans D, Menezes C, Mahomed K, Macdonald P, Untiedt S, Levin L, et al. Treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa. AIDS Res Hum Retrovir. 2013;29(6):892–900. https://doi.org/10.1089/AID.2012.0215
Adejumo OA, Malee KM, Ryscavage P, Hunter SJ, Taiwo BO. Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-saharan Africa: a narrative review. J Int AIDS Soc. 2015;18(1):20049. https://doi.org/10.7448/IAS.18.1.20049
Haas AD, Lienhard R, Didden C, Cornell M, Folb N, Boshomane TMG, et al. Mental health, ART adherence, and viral suppression among adolescents and adults living with HIV in South Africa: a cohort study. AIDS Behav. 2023;27(6):1849–61. https://doi.org/10.1007/s10461-022-03916-x
Mellins CA, Malee KM. Understanding the mental health of youth living with perinatal HIV infection: lessons learned and current challenges. J Int AIDS Soc. 2013;16(1):18593. https://doi.org/10.7448/IAS.16.1.18593
Hosek SG, Harper GW, Robinson WL. Identity development in adolescents living with HIV. J Adolesc. 2002;25(4):355–64. https://doi.org/10.1006/jado.2002.0480
Arain M, Haque M, Johal L, et al. Maturation of the adolescent brain. Neuropsych Dis Treat. 2013;9:449–61. https://doi.org/10.2147/NDT.S39776
Ammon N, Mason S, Corkery J. Factors impacting antiretroviral therapy adherence among human immunodeficiency virus–positive adolescents in sub-saharan Africa: a systematic review. Pub Health. 2018;157:20–31. https://doi.org/10.1016/j.puhe.2017.12.010
Vreeman RC, Scanlon ML, McHenry MS, Nyandiko WM. The physical and psychological effects of HIV infection and its treatment on perinatally HIV-infected children. J Int AIDS Soc. 2015;18(7 Suppl 6):20258. https://doi.org/10.7448/IAS.18.7.20258
Hoare J, Phillips N, Brittain K, Myer L, Zar HJ, Stein DJ. Mental health and functional competence in the Cape Town adolescent antiretroviral cohort. J Acquir Immune Defic Syndr. 2019;81(4):e109–16. https://doi.org/10.1097/QAI.0000000000002068
Mutumba M, Musiime V, Lepkwoski JM, et al. Examining the relationship between psychological distress and adherence to anti-retroviral therapy among Ugandan adolescents living with HIV. AIDS Care. 2016;28(7):807–15. https://doi.org/10.1080/09540121.2015.1131966
World Health Organization. Psychological well-being. Geneva, Switzerland. http://apps.who.int/adolescent/hiv-testing-treatment/page/Psychological_well_being. 2013. Accessed January 31, 2024.
Vranda MN, Mothi SN. Psychological issues of children infected with HIV/ AIDS. Indian J Psychol Med. 2013;35(1):19–22. https://doi.org/10.4103/0253-7176.112195
Ayano G, Demelash S, Abraha M, Tsegay L. The prevalence of depression among adolescent with HIV/AIDS: a systematic review and meta-analysis. AIDS Res Ther. 2021;18(1):23. https://doi.org/10.1186/s12981-021-00351-1
Dyer J, Wilson K, Badia J, Agot K, Neary J, Njuguna I, Kibugi J, Healy E, Beima-Sofie K, John-Stewart G, Kohler P. The psychological effects of the COVID-19 pandemic on youth living with HIV in Western Kenya. AIDS Behav. 2021;25(1):68–72. https://doi.org/10.1007/s10461-020-03005-x
Hong C, Queiroz A, Hoskin J. The impact of the COVID-19 pandemic on mental health, associated factors and coping strategies in people living with HIV: a scoping review. J Int AIDS Soc. 2023;26(3):e26060. https://doi.org/10.1002/jia2.26060
Kalichman SC, El-Krab R. Social and behavioral impacts of COVID-19 on people living with HIV: review of the first year of research. Curr HIV/AIDS Rep. 2022;19(1):54–75. https://doi.org/10.1007/s11904-021-00593-8
Langsi R, Osuagwu UL, Goson PC, Abu EK, Mashige KP, Ekpenyong B, et al. Prevalence and factors associated with mental and emotional health outcomes among Africans during the COVID-19 lockdown period-a web-based cross-sectional study. Int J Environ Res Public Health. 2021;18(3):899. https://doi.org/10.3390/ijerph18030899
Addae EA. COVID-19 pandemic and adolescent health and well-being in sub-saharan Africa. Who Cares? Int J Health Plann Manage. 2021;36(1):219–22. https://doi.org/10.1002/hpm.3059
Kola L, Kohrt BA, Hanlon C, Naslund JA, Sikander S, Balaji M, et al. COVID-19 mental health impact and responses in low-income and middle-income countries: reimagining global mental health. Lancet Psych. 2021;8(6):535–50. https://doi.org/10.1016/S2215-0366(21)00025-0
World Bank. Updated estimates of the impact of the COVID-19 on global poverty. Geneva, Switzerland. https://blogs.worldbank.org/opendata/updated-estimates-impact-covid-19-global-poverty-turning-corner-pandemic-2021. Published 2021. Accessed February 1, 2024.
Köhler T, Bhorat H, Hill R, Stanwix B. Lockdown stringency and employment formality: evidence from the COVID-19 pandemic in South Africa. J Labour Mark Res. 2023;57(3):3. https://doi.org/10.1186/s12651-022-00329-0
South African Government. Regulations and guidelines: Coronavirus COVID-19. Pretoria, South Africa. https://www.gov.za/covid-19/resources/regulations-and-guidelines-coronavirus-covid-19. Published 2020. Accessed February 1, 2024.
National Income Dynamics Study. NIDS-CRAM synthesis report. https://cramsurvey.org/wp-content/uploads/2020/07/Spaull-et-al.-NIDS-CRAM-Wave-1-Synthesis-Report-Overview-and-Findings-1.pdf. Published 2020. Accessed February 1, 2024.
De Wet-Billings N. Perpetuation of household food insecurity during COVID-19 in South Africa. J Health Popul Nutr. 2023;42(1):96. https://doi.org/10.1186/s41043-023-00441-y
Humphries H, Lewis L, Lamontagne E, Choonara S, Dikgale K, Yakusik A, et al. Impact of COVID-19 public health responses on income, food security and health services among key and vulnerable women in South Africa. Afr J AIDS Res. 2022;21:317–29.
Campbell LS, Masquillier C, Knight L, Delport A, Sematlane N, Dube LT, et al. Stay-at-home: the impact of the COVID-19 lockdown on household functioning and ART adherence for people living with HIV in three sub-districts of Cape Town, South Africa. AIDS Behav. 2022;26(6):1905–22. https://doi.org/10.1007/s10461-021-03541-0
Mabaso M, Makola L, Naidoo I, et al. HIV prevalence in South Africa through gender and racial lenses: results from the 2012 population-based national household survey. Int J Equity Health. 2019;18:167. https://doi.org/10.1186/s12939-019-1055-6
Nyirenda M, Street R, Reddy T, et al. Food insecurity, HIV status and prior testing at South African primary healthcare clinics. S Afr J Sci. 2018;114(9–10):1–6. https://doi.org/10.17159/sajs.2018/4407
Bernays S, Lanyon C, Dlmaini V, et al. Being young and on the move in South Africa: how ‘waithood’ exacerbates HIV risks and disrupts the success of HIV interventions. Vul Child Youth Stu. 2020;15(4):368–78. https://doi.org/10.1080/17450128.2020.1739359
Köhler T et al. COVID-19 and the labour market: estimating the effects of South Africa’s national lockdown. Development Policy Research Unit, School of Economics, University of Cape Town. 2021.
Aneshensel CS. Social stress: Theory and research. Ann Rev Sociology. 1992; 18: 15–38.https://doi.org/10.1146/annurev.so.18.080192.000311
Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, Ho RC. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. https://doi.org/10.3390/ijerph17051729
Xiao H, Yan Z, Desheng K, Shiyue L, Ningxi Y. The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February 2020 in China. Med Sci Monit. 2020;26:e923549–1. https://doi.org/10.12659/MSM.923549
Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, Rasoulpoor S, Khaledi-Paveh B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1):57. https://doi.org/10.1186/s12992-020-00589-w
Springer SA, Dushaj A, Azar MM. The impact of DSM-IV mental disorders on adherence to combination antiretroviral therapy among adult persons living with HIV/AIDS: a systematic review. AIDS Behav. 2012;16(8):2119–43. https://doi.org/10.1007/s10461-012-0212-3
Wykowski J, Kemp CG, Velloza J, Rao D, Drain PK. Associations between anxiety and adherence to antiretroviral medications in low- and middle-income countries: a systematic review and meta-analysis. AIDS Behav. 2019;23(8):2059–71. https://doi.org/10.1007/s10461-018-02390-8
Nyamaruze P, Govender K, Cowden RG. Self-esteem and antiretroviral therapy adherence among young people living with HIV: an exploratory serial mediation analysis. South Afr J Sci. 2021;117:1–7. https://doi.org/10.17159/sajs.2021/8354
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Schotte S, Zizzamia R. The livelihood impacts of COVID-19 in urban South Africa: a view from below. Soc Indic Res. 2023;165(1):1–30. https://doi.org/10.1007/s11204-022-02978-7
South African Government. Disaster Management Act: Declaration of National State of Disaster. 2020. https://www.gov.za/sites/default/files/gcis_document/202003/43096gon313.pdf
Statistics South Africa. Employment surpasses pre-COVID levels in SA. 2023. https://www.statssa.gov.za/?p=16809
Cholera R, et al. Validity of the patient health questionnaire-9 to screen for depression in a high-HIV burden primary healthcare clinic in Johannesburg, South Africa. J Aff Disorders. 2014;167:160–6. https://doi.org/10.1016/j.jad.2014.06.003
Kroenke K, Spitzer RL, Williams JB, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–25. https://doi.org/10.7326/0003-4819-146-5-200703060-00004
Marlow M, et al. Detecting depression and anxiety among adolescents in South Africa: validity of the isiXhosa patient health questionnaire-9 and generalized anxiety disorder-7. J Adolesc Health. 2023;72(1):52–60. https://doi.org/10.1016/j.jadohealth.2022.09.013
Rosenberg M. Rosenberg self-esteem scale. J Relig Health. 1965. https://doi.org/10.1037/t01038-000
Makhubela M, Mashegoane S. Psychological validation of the Rosenberg Self-Esteem Scale (RSES) in South Africa: method effects and dimensionality in Black African and White university students. J Psych Afr. 2017;27(3):277–81. https://doi.org/10.1080/14330237.2017.1294303
Salvador Castell G, Pérez Rodrigo C, Ngo de la Cruz J, Aranceta Bartrina J. Household food insecurity access scale (HFIAS). Nutr Hosp. 2015;31:272–8. https://doi.org/10.3305/nh.2015.31.sup3.8775
Desiere S, Marijke D, Niragira S. Assessing the cross-sectional and inter-temporal validity of the household food insecurity access scale (HFIAS) in Burundi. Pub Hel Nutr. 2015;18(15):2775–85. https://doi.org/10.1017/S13689800150000403
Knueppel D, Demment M, Kaiser L. Validation of the household food insecurity access scale in rural Tanzania. 2010;13(3):360–7. https://doi.org/10.1017/S1358980009991121
Coates J, Swindale A, Bilinsky P. Household food insecurity access scale (hfias) for measurement of food access: indicator guide, version 3. Washington, D.C.: Food and Nutrition Technical Assistance Project, Academy fo Educational Development. 2007. https://www.fao.org/fileadmin/user_upload/eufao-fsi4dm/doc-training/hfias.pdf
Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Pscyhol. 1986;51(6):1173. https://doi.org/10.1037/0022-3514.51.6.1173
Sobel ME. Asymptotic confidence intervals for indirect effects in structural equations models. Soc Method. 1982:290–312. https://doi.org/10.2307/270723
Whittle HJ, Sheira LA, Frongillo EA, et al. Longitudinal associations between food insecurity and substance use in a cohort of women with or at risk for HIV in the United States. Addiction. 2019;114:127–36. https://doi.org/10.1111/add.14418
Weiser SD, Young SL, Cohen CR, et al. Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am J Clin Nutr. 2011;94(6):S1729–39. https://doi.org/10.3945/ajcn.111.012070
Nwosu CO, Kollamparambil U, Oyenubi A. Food insecurity and health outcomes during the coronavirus pandemic in South Africa: a longitudinal study. Health Econ Rev. 2022;12(1):32. https://doi.org/10.1186/s13561-022-00375-x
Arndt C, Davies R, Gabriel S, Harris L, Makrelov K, Robinson S, Levy S, Simbanegavi W, van Seventer D, Anderson L. Covid-19 lockdowns, income distribution, and food security: an analysis for South Africa. Glob Food Sec. 2020;26:100410. https://doi.org/10.1016/j.gfs.2020.100410
Wills G, Patel L, Van der Berg S, Mpeta B. Household resource flows and food poverty during South Africa’s lockdown: short-term policy implications for three channels of social protection. NIDS-CRAM Working Paper 12. 2020. https://doi.org/10.2139/ssrn.4331504
Statistics South Africa. How COVID-19 affected food insecurity in South Africa. Pretoria, South Africa. https://www.statssa.gov.za/?p=15273. Published 2022. Accessed 8 May, 2024.
South African Government. Minister Tito Mboweni: 2020 Budget Speech. Pretoria, South Africa. https://www.gov.za/BudgetSpeech2020. Published 2020. Accessed February 6, 2024.
Moses E, Woolard I. The role of temporary social grants in mitigating the poverty impact of COVID-19 in South Africa. In: Fourie P, Lamb G, editors. The South African response to COVID-19: the early years. New York: Routledge; 2023. pp. 156–77.
Van Pinxteren M, Colvin C, How. May, COVID-19 changed community engagement in South Africa’s low-income areas. https://www.preventionweb.net/news/how-covid-19-changed-community-engagement-south-africas-low-income-areas. Published 2020. Accessed 3 2024.
Solidarity Fund. Solidary fund food relief programme summary report. https://solidarityfund.co.za/media/2020/06/SF_-_Food_Relief_Programme_Summary_Report_-_June_2020.pdf. Published 2020. Accessed 8 May, 2024.
Trudell JP, Burnet ML, Ziegler BR, Luginaah I. The impact of food insecurity on mental health in Africa: a systematic review. Social Sci Med. 2021;278. https://doi.org/10.1016/j.socscimed.2021.113953
Bhatia S, Johnston CD, Derry-Vick H, Brennan-Ing M, Burchett CO, Siegler EL, Glesby MJ. Food insecurity is associated with key functional limitations and depressive symptoms in older people living with HIV. AIDS Pat STDs. 2022;36(10):375–8. https://doi.org/10.1089/apc.2022.0118
von Fintel D, Pienaar L. Small-scale farming and food security: the enabling role of cash transfers in South Africa’s former homelands, IZA discussion papers. 2016, No. 10377.
Pourmotabbed A, Moradi S, Babaei A, Ghavami A, Mohammadi H, Jalili C, Symonds ME, Miraghajani M. Food insecurity and mental health: a systematic review and meta-analysis. Public Health Nutr. 2020;23(10):1778–90. https://doi.org/10.1017/S136898001900435X
Ferguson J. Give a man a fish: reflection on the new politics of distribution. Durham, North Carolina: Duke University Press; 2015.
Wolfson JA, Garcia T, Leung CW. Food insecurity is associated with depression, anxiety, and stress: evidence from the early days of the COVID-19 pandemic in the United States. Health Equity. 2021;5(1):64–71. https://doi.org/10.1089/heq.2020.0059
Jones AD. Food insecurity and mental health status: a global analysis of 149 countries. Am J Prev Med. 2017;53(2):264–73. https://doi.org/10.1016/j.amepre.2017.04.008
Martin MS, Maddocks E, Chen Y, et al. Food insecurity and mental illness: disproportionate impacts in the context of perceived stress and social isolation. Public Health. 2016;132:86–91. https://doi.org/10.1016/j.puhe.2015.11.014
Ohrnberger J, Fichera E, Sutton M, et al. The effect of cash transfers on mental health – new evidence from South Africa. BMC Pub Health. 2020;20(1):436. https://doi.org/10.1186/s12889-020-08596-7
Garman EC, Eyal K, Avendano M, Evans-Lacko S, Lund C. Cash transfers and the mental health of young people: evidence from South Africa’s child support grant. Soc Sci Med. 2022;292:114631. https://doi.org/10.1016/j.socscimed.2021.114631
Lee J, Seon J. Intergenerational transmission of maternal poverty to self-esteem among young adult children: the role of employment. Child Youth Serv Rev. 2019;106:104492. https://doi.org/10.1016/j.childyouth.2019.104492
Doi S, Fujiwara T, Isumi A, Ochi M. Pathway of the Association between child poverty and low self-esteem: results from a population-based study of adolescents in Japan. Front Psychol. 2019;10:937.
Ivers LC, Cullen KA, Freedberg KA, Block S, Coates J, Webb P. HIV/AIDS, undernutrition, and food insecurity. Clin Infect Dis. 2009;49:1096–102. https://doi.org/10.3389/fpsyg.2019.00937
Fuseini H, Gyan BA, Kyei GB, Heimburger DC, Koethe JR. Undernutrition and HIV infection in sub-saharan Africa: health outcomes and therapeutic interventions. Curr HIV/AIDS Rep. 2021;18(2):87–97. https://doi.org/10.1007/s11904-021-00541-6
Rawat R, McCoy SI, Kadiyala S. Poor diet quality is associated with low CD4 count and anemia and predicts mortality among antiretroviral therapy–naive HIV-positive adults in Uganda. J Acquir Immune Defic Syndr. 2013;62(2):246–53. https://doi.org/10.1097/QAI.0b013e3182797363
Weiser SD, Palar K, Frongillo EA, Tsai AC, Kumbakumba E, Depee S, et al. Longitudinal assessment of associations between food insecurity, antiretroviral adherence and HIV treatment outcomes in rural Uganda. AIDS. 2014;28(1):115–20. https://doi.org/10.1097/01.aids.0000433238.93986.35
Bärnighausen T, Chaiyachati K, Chimbindi N, Peoples A, Haberer J, Newell ML. Interventions to increase antiretroviral adherence in sub-saharan Africa: a systematic review of evaluation studies. Lancet Inf Dis. 2011;11(12):942–51. https://doi.org/10.1016/S1473-3099(11)70181-5
Palar K, Napoles T, Hufstedler LL, Seligman H, Hecht FM, Madsen K, et al. Comprehensive and medically appropriate food support is associated with improved HIV and diabetes health. J Urban Health. 2017;94(1):87–99. https://doi.org/10.1007/s11524-016-0129-7
Ojo T, Ruan C, Hameed T, Malburg C, Thunga S, Smith J, Vieira D, Snyder A, Tampubolon SJ, Gyamfi J, Ryan N, Lim S, Santacatterina M, Peprah E. HIV, tuberculosis, and food insecurity in Africa-a syndemics-based scoping review. Int J Environ Res Public Health. 2022;19(3):1101. https://doi.org/10.3390/ijerph19031101
Rawat R, Faust E, Maluccio JA, Kadiyala S. The impact of a food assistance program on nutritional status, disease progression, and food security among people living with HIV in Uganda. J Acq Immune Defic Syn. 2014;66(1):e15–22. https://doi.org/10.1097/QAI.0000000000000079
Maluccio JA, Palermo T, Kadiyala S, Rawat R. Improving health-related quality of life among people living with HIV: results from an impact evaluation of a food assistance program in Uganda. PLoS ONE. 2015;10(8):e0135879. https://doi.org/10.1371/journal.pone.0135879
Hatcher A, Hufstedler EL, Doria K, Shari L, Dworkin EW, Conroy A, et al. Mechanisms and perceived mental health changes after a livelihood intervention for HIV-positive kenyans: longitudinal, qualitative findings. Transcult Psychiatry. 2020;57(1):124–39. https://doi.org/10.1177/1363461519858446
Funding
This secondary analysis was conducted based on data from two studies funded with support from Principal Investigator’s NIH R34 Award (R34MH114897) and an administrative supplement (NIH R34 MH114897-02S1).
Author information
Authors and Affiliations
Contributions
CPB was involved in the conceptualization, formal analysis, investigation, methodology, and original draft preparation. TLL was involved in the investigation, formal analysis, and reviewing and editing of this manuscript. AM was involved in the investigation, formal analysis, reviewing and editing of this manuscript. ER was involved in the investigation, formal analysis, and reviewing and editing of this manuscript. SS was involved in the investigation, formal analysis, reviewing and editing of this manuscript. NS was involved in the investigation, formal analysis, reviewing and editing of this manuscript. LM was involved in the investigation, methodology, project administration, and reviewing and editing of this manuscript. LGB was involved in the supervision, investigation, formal analysis, and reviewing and editing of this manuscript. VAE was involved in the conceptualization, supervision, methodology, validation, and reviewing and editing of this manuscript. ITK was involved in the funding acquisition, conceptualization, supervision, methodology, validation, and reviewing and editing of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Partners Healthcare Institutional Review Board at Brigham and Women’s Hospital and Massachusetts General Hospital, Harvard Medical School, Boston, MA and the Human Research Ethics Committee at the University of Cape Town, South Africa. Informed consent was obtained from all participants engaging in both studies.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bondarchuk, C.P., Lemon, T., Medina-Marino, A. et al. Food insecurity and unemployment as mediators of the relationship between the COVID-19 pandemic and psychological well-being in young South Africans with HIV. BMC Public Health 24, 2622 (2024). https://doi.org/10.1186/s12889-024-19966-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19966-w