
Abstract
Background
With a series of clinical trials confirming the sensitivity of small cell lung cancer (SCLC) to immunotherapy, research on personalized treatment for SCLC has gained increasing attention. Currently, the most widely accepted subtype of SCLC is based on the expression levels of Achaete-Scute Family BHLH Transcription Factor 1 (ASCL1), neurogenic differentiation factor 1 (NEUROD1), and POU class 2 homeobox 3 (POU2F3). However, real-world studies on this classification remain limited.
Methods
We retrospectively collected biopsy specimens from patients who received immunotherapy at Shandong Provincial Hospital between January 2019 and July 2021. After determining the patient subtypes using immunohistochemistry, we analyzed the relationships between each subtype and survival as well as some clinical characteristics.
Results
In our study, we found that the subtype I achieved a significant survival advantage compared to the other groups. Additionally, the subtype A demonstrated a significant survival disadvantage. Among patients in the subtype I, there was a higher proportion of early brain metastasis and patients with a family history of tumors, while the subtype A had a lower proportion. Furthermore, the subtype A exhibited relatively poor immune infiltration.
Conclusion
In a diverse cohort of SCLC patients receiving immunotherapy, the subtype-I showed significant survival advantages while the subtype-A experienced a worse survival.
Similar content being viewed by others

Introduction
In the study of lung cancer, it is customary to categorize it into two major types: small cell lung cancer (SCLC), accounting for approximately 15% of cases, and non-small cell lung cancer (NSCLC), constituting the remaining 85% [1]. Meanwhile, advancements in therapeutic modalities for NSCLC have gradually led to an increasing number of cases in which lung adenocarcinoma transforms into SCLC [2]. This trend not only indicates the dynamic changes in lung cancer cells during treatment but also underscores the necessity of precise therapy for SCLC [2]. SCLC, characterized by early metastasis and high malignancy [3] as its predominant features, exhibits poor clinical outcomes with a two-year overall survival (OS) rate of approximately 3–13% [4, 5]. Apart from its aggressive nature, the poor prognosis of SCLC can also be attributed to the lack of specific treatment options [1]. In contrast to NSCLC, where patients without surgical opportunities can still achieve considerable survival benefits with targeted therapies and immunotherapies [2], SCLC remains challenging. The high mutational burden observed in SCLC suggests its potential immunogenicity and responsiveness to immune checkpoint inhibitors (ICIs) [1]. Building on this understanding, numerous clinical trials have been conducted, exploring the efficacy of monoclonal antibodies targeting programmed cell death protein 1 (PD-1), programmed death ligand 1 (PD-L1), and cytotoxic T-lymphocyte antigen 4 (CTLA-4) for SCLC [1, 5, 6]. However, not all trials have achieved satisfactory results [4]. For SCLC, despite being proved that adding immunotherapy to platinum-based chemotherapy can generate survival benefits, the improvement remains modest and the benefits vary among patients [7]. In the era of immunotherapy, gaining a clearer understanding of intratumoral and stromal heterogeneity in SCLC will undoubtedly help us devise a more targeted treatment for every patient. [8,9,10].
Recently, Gay et al. made some significant findings reference to previous work concerning some meaningful transcription factors of SCLC [9, 11]. By employing non-negative matrix factorization (NMF), Gay et al. classified SCLC into four distinct subtypes based on the expression levels of three genes: Achaete-Scute Family BHLH Transcription Factor 1 (ASCL1), neurogenic differentiation factor 1 (NEUROD1), and POU class 2 homeobox 3 (POU2F3) [12]. These subtypes were designated as SCLC-A (ASCL1-dominant), SCLC-N (NEUROD1-dominant), SCLC-P (POU2F3-dominant), and SCLC-I (triple-negative). This approach allows for a comprehensive characterization of SCLC heterogeneity, paving the way for further insights into the underlying molecular mechanisms and the development of potential targeted therapies [12]. Building upon previous research [11, 13, 14], the authors further investigated the differences among these subtypes in terms of prognosis, drug sensitivity, epithelial differentiation, tumor immune microenvironment(TIME), and resistance mechanisms [12]. This study undoubtedly provides new insights and directions for personalized treatment of SCLC, highlighting that each subtype exhibits unique vulnerabilities to different therapeutic approaches.
Despite evidence both supporting and opposing the role of tumor mutational burden (TMB) [15] and PD-L1 [16] expression, the standard therapeutic regimen for SCLC remains platinum-based chemotherapy in conjunction with ICIs, as supported by numberous clinical trials [5, 17]. Based on the aforementioned subtype analysis, it is evident that different subtypes possess distinct vulnerabilities, with no strict boundaries between them [1]. Subtype-specific intra-tumor heterogeneity (ITH) appears to be a dynamic process [18]. For instance, the SCLC-A subtype may exhibit relative sensitivity to platinum, but after a period of chemotherapy, new tumor cells could emerge as the SCLC-I subtype, characterized by immunosensitivity [12]. This expands the possibilities in clinical treatment, raising questions about how patients can derive maximum benefits from various combinations of immunotherapy, chemotherapy, and radiotherapy [1, 19]. Can distinct subtypes guide the selection of different treatment modalities and preventive interventions such as thoracic radiation therapy (TRT) and prophylactic cranial irradiation (PCI)? This article aims to contribute to this exploration.
Methods
Patients and tissue samples
We retrospectively collected data from patients diagnosed with extensive-stage small cell lung cancer (ES-SCLC) at Shandong provincial hospital between January 2019 and July 2021. A specific group of 93 SCLC patients was selected based on complete medical records, consistent follow-up data, and relevant radiological information. The follow-up data were obtained from clinical records and telephone interviews. Inclusion criteria included: (1) pathologically confirmed SCLC diagnosis, (2) immunotherapy administered alongside chemotherapy, and (3) sufficient pathological tissue for subtyping. All patients were between 18 and 75 years of age and had extensive-stage disease. Patients with limited-stage disease who experienced recurrence after chemotherapy were included, while those with postoperative recurrence were excluded. Additionally, referring to Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1), we ensured that each patient had at least one measurable lesion. Patients with more than two distant metastases were defined as having multiple metastases. According to the 9th edition of the American Joint Committee on Cancer (AJCC) staging for SCLC, we assessed the TNM (tumor, node and metastasis) stage information of each patient at the time of diagnosis and recorded detailed information regarding the sites of metastasis. Subsequently, we collected pathological specimens from the enrolled SCLC patients for further analysis.
The related definition of tumor response, toxicity and survival
Tumor response during chemotherapy/immunotherapy maintenance was evaluated every 2 cycles by experienced radiologists using imaging techniques such as CT scans. All radiologists had a minimum of 10 years of experience. Tumor response was categorized according to RECIST 1.1 criteria as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Patients with CR or PR were considered responders, while those with SD or PD were classified as non-responders. Objective response rate (ORR) was defined as the percentage of patients with PR and CR. Adverse events were assessed and graded according to the Common Terminology Criteria for Adverse Events version 4.0, with common events including severe myelosuppression, liver function impairment, nausea/vomiting, and neurotoxicity. OS was defined as the time from diagnosis of extensive-stage disease to death from any cause or last follow-up. Progression-free survival (PFS) was measured from the date of diagnosis to the date of recurrence, death without recurrence, or the last follow-up without recurrence. Survival status was obtained through regular medical records or telephone follow-up.
Immunohistochemistry (IHC)
We obtained formalin-fixed paraffin-embedded (FFPE) specimens from 58 patients prior to chemotherapy and immunotherapy, with each section having a thickness of 4µm. The sections were then deparaffinized through graded concentrations of xylene and ethanol solutions, followed by multiple washes with phosphate-buffered saline (PBS). For antigen retrieval, sections were placed in an antigen retrieval solution and subjected to pressure-induced antigen retrieval. After cooling, endogenous peroxidase was blocked by adding an inhibitor and incubating the sections for 30 min in the dark. After PBS washes, diluted antibodies ASCL1 (bs-1155R, from Bioss-biology; 1:200), NEUROD1 (ET-1703, from Huaan-biology; 1:100), POU2F3 (YT-6917, from Immunoway-biology; 1:100), and CD8α (ab101500, from ZSGB-biology; Working solution) were evenly applied to the sections and incubated overnight at 4°C. The next day, sections were incubated at room temperature for 1 h, washed with PBS, and then incubated with the appropriate secondary antibodies for 30 min. Finally, sections were developed with 3,3'-Diaminobenzidine (DAB) chromogen for 30 s and washed under running water to stop the reaction. Nuclei were counterstained with hematoxylin for 1 min and differentiated in hydrochloric ethanol for 30 s, followed by a 1-min water wash. The sections were then dehydrated through graded ethanol and xylene and finally mounted with neutral balsam [10, 20].
We employed two quantification methods, each independently performed by two blinded pathologists. After scanning, pathologists independently assessed slide expression intensity, scoring from 0 to 3 (0: Negative, 1: Weak, 2: Moderate, 3: Intense). An additional score, based on the percentage of positive cells (0: 0–5%, 1: 5–25%, 2: 25–50%, 3: > 50%), was assigned. The final score was the product of these two scores. Minor discrepancies were resolved through discussion, while major disagreements were reviewed by a third senior pathologist to reach consensus. For CD8 + T cells, two pathologists selected 2–3 representative areas (20X, 30 × 30µm2) from scanned slides, with two individuals jointly counting CD8 + T cells. The average CD8 + T cell density was calculated as the number of CD8 + T cells divided by the number of tumor cells per area, averaged over 5–6 areas per slide.
Statistical analysis
The differences in OS and PFS were calculated using the Kaplan–Meier (KM) method. Linear regression analysis examined the correlation between ASCL1, NEUROD1, and POU2F3 expression levels and their relationships with the IHC scores of CD8 + T cells. The chi-square test and Fisher's exact test were employed to compare baseline data, tumor response, and adverse events among the four groups. In regard to the score of ASCL1, NEUROD1, and POU2F3, we first treated them as quantitative data and assessed for normality using the Shapiro–Wilk method, confirming their non-normal distribution. The Mann–Whitney U test was then applied to compare these skewed data distributions. Univariate and multivariate Cox regression analyses were conducted to elucidate the associations between subtypes, prognosis, and clinical relevance. Patients were classified into four subtypes based on the relative IHC scores of ASCL1, NEUROD1, and POU2F3, and each subtype was included as a categorical variable in the Cox multivariable regression model. To validate the conclusions from the chi-square test, Cox multivariable models were repeatedly constructed for the A and I subtypes, which are potentially associated with prognosis. Factors with a P-value < 0.1 in the univariate analysis were included in the multivariate analysis. All tests were two-tailed, with a significance level of P < 0.05 considered statistically significant. The statistical software packages used in our study included SPSS version 25, GraphPad Prism 8.0, and MedCalc 20.0.4.
Results
Patient characteristics
This study enrolled 58 patients: 47 males (81.03%) and 11 females (18.97%), with 40 patients aged over 60 years. We examined smokers and non-smokers but found no direct relationship between smoking status and the four subtypes. T and N stage distributions did not differ significantly among subtypes. Baseline data comparisons are detailed in Table 1. Immune infiltration, represented by CD8, and metastatic sites were investigated across subtypes. Subtype I showed distinctive clinical features, including higher rates of family history of cancer and brain metastasis at diagnosis, as illustrated in Fig. 3E. Subtype A exhibited poorer CD8 immune infiltration. Of all patients, 43 (74.14%) responded positively to chemotherapy with partial response (PR), but no complete responses (CR) were observed. Grade 3 or higher adverse events were noted in 11 patients.
IHC reuslts and subtype
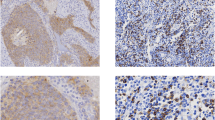
According to previous literature and The Human Protein Atlas database (THPA, www.proteinatlas.org), ASCL1 and NEUROD1 is primarily expressed in the nucleus of lung cancer cells, while POU2F3 tend to be expressed in the cytoplasm and cell membrane. In our study, we identified positive expression of ASCL1 in 38 patients, with 1 case showing strong positivity, positive expression of NEUROD1 in 25 patients, with 2 cases showing strong positivity, and positive expression of POU2F3 in 36 patients, with 1 case showing strong positivity. Among the 58 patients, there were a total of 24 cases of SCLC-A (24/58,41.4%), 12 cases of SCLC-N (12/58,20.7%), 11 cases of SCLC-P (11/58,18.9%), and 11 cases of SCLC-I (11/58,18.9%). Representative views of different levels of positive expression for each gene are presented in Fig. 1A, while the typical views of the expression levels of three different genes in 4 patients are shown in Fig. 2A. Regarding the percentage of CD8-positive cells, based on previous literature, a positivity threshold of > 30% was defined. In our study, a total of 8 patients (13.8%) exhibited high expression of CD8-positive cells [21], while representative views of CD8-negative and strongly positive expression were included in Fig. 1B.

Immunohistochemistry results and the survival of 4 different type. A Representative IHC images in different expression level of ASCL1, NEUROD1, POU2F3. B Representative immunohistochemistry images of CD8+ and CD8-tumor infiltrating lymphocytes (TILs). C Theoverall survival of 4 different type. D The progression-free survival of 4 different type

Immunohistochemistry results of 4 patients and their survival outcomes. A A glimpse into the characteristic immunohistochemistry results of three gene across four subtypes. B The survival outcomes of subtype-A and non-A. C The survival outcomes of subtype-N and non-N. D The survival outcomes of subtype-P and non-P. D The survival outcomes of subtype-I and non-I. B-D Overall survival (OS) outcomes on the left, progression-free survival (PFS) outcomes on the right
Survival analysis
The median OS for the four subtypes (ordered by ANPI) was 9.42 months, 13.34 months, 9.83 months, and 15.07 months, respectively. Median PFS for the subtypes was 4.83 months, 6.29 months, 5.70 months, and 12.17 months, respectively. Subtype I showed a significant survival advantage over other subtypes in both OS (p = 0.053) and PFS (p = 0.0119) (Figs. 1C-D). Survival curves plotted in Fig. 2 highlighted subtype A's notable disadvantage in OS and PFS. Cox regression analysis explored the.
addedassociation between subtypes and prognosis, incorporating gender, age, family tumor history, selected blood indicators, and treatment strategies impacting outcomes. Detailed regimen for all patients are presented in Table 2.
In our previous findings, subtype A initially showed a poorer prognosis. However, after adjusting for various potential prognostic factors (Fig. 3C), its impact on prognosis became non-significant, similar to subtype I. The prognostic effects of these subtypes may be influenced by factors such as liver metastases and immune infiltration. Adjusting for CD8 infiltration notably altered the prognosis associated with subtype A. Although subtype I initially showed a tendency towards protective effects on OS, this effect became non-significant after adjusting for all factors, although it persisted for PFS. Cox multivariable regression models consistently showed significant impacts of both A and I subtypes on PFS, presented in a forest plot (Fig. 3). Combining A and P subtypes versus the other two subtypes revealed distinct differences in both OS and PFS (Fig. 4A-B). Further investigation is needed to fully understand these findings.

Cox Univariable and Multivariable Analysis results. A-B Forest plot revealing there results of cox univariable. C-F Forest plot revealing the results of cox multivariable analysis. OS on the left, PFS on the right. The model of the A subtype is presented above, while the model for the I subtype is shown below

Survival outcomes and the correlations among genes and between CD8 and genes. A Overall survival of subtype A,P and subtype N,I. B Progression-free survival of subtype A,P and subtype N,I. C The average immunohistochemical (IHC) scores of ASCL1, NEUROD1, and POU2F3 in four subtypes represented by bar graphs. D Regression curves of Immunohistochemistry (IHC) scores for three genes, paired in two groups. E The interrelationship between the IHC scores of three genes and the percentage of CD8-positive T cells
The interplay of gene expression levels and CD8 cells
After identifying coexpression of three genes, we investigated their potential correlation. While significant, the associations among their expression levels was not strong (Fig. 4D). Average IHC scores for each gene across subtypes are depicted in Fig. 4C, showing non-binary, cross-interacting characteristics. Our study found no superior immune infiltration in subtype I or other subtypes, but observed poorer immune infiltration in subtype A. Figure 4E shows no statistically significant correlation between CD8 + T cell infiltration and the expression of the three genes. To clarify the relationship between CD8α + T cell levels, IHC scores, and prognosis, associations were visualized in bubble plots (Figs. 5A and 6A). Bubble size indicates relative OS and PFS, with yellow (0) representing patients yet to reach the follow-up endpoint and blue (1) indicating those who reached it during the study period.

The Relationship between Subgroup Distribution, Immunohistochemical (IHC) score and Adverse Events (AES). A The bubble plot elucidates the associations between IHC scores, CD8-positive cell percentage, and overall survival. B The pie chart reveals the distribution of AEs among two distinct groups: <Grade 3 AES and ≥ Grade 3 AEs. C Grapevine plot illustrating the relationship between IHC scores and the occurrence of grade 3 or higher AEs

The Relationship between Subgroup Distribution and Clinical Characteristics. A The bubble plot elucidates the associations between three gene IHC scores, CD8-positive cell percentage, and progression-five survival. B The pie chart reveals subgroup distribution among two distinct groups: Responder and non-responder. C Melodic violin plot unveiling the relationship between IHC Scores and immune response
Relationship between Clinical Characteristics and IHC Score
Adverse events recorded in this study mainly included hematological events (such as leukopenia, neutropenia, anemia, and thrombocytopenia), gastrointestinal reactions (such as liver function damage, vomiting, and diarrhea), and certain neurological and psychiatric symptoms (such as headache, dizziness, fatigue, and limb numbness or pain). We further analyzed the distribution of grade 3 or higher adverse events among the subtypes. Interestingly, in subtype P, although patients did not exhibit any additional survival advantages, none experienced adverse events of grade 3 or higher. Similarly, in subtype A, only a few patients experienced adverse events of grade 3 or higher, although these differences were not statistically significant (Fig. 5B, p = 0.158).
Furthermore, we also focused on the tumor response to chemotherapy drugs during immunotherapy. We conducted a detailed analysis of the distribution among responders and non-responders. Although there were subtle differences in distribution, we did not observe significant differences in subtype composition between them (Fig. 6B, p = 0.594). Regarding the IHC scores for each gene, we considered them as quantitative data and analyzed their relationship with tumor response and adverse events (AEs). The associations were demonstrated in Fig. 5C and Fig. 6C, respectively.
Discussion
Recent advancements in sequencing technologies have led to the classification of SCLC based on ASCL1, NEUROD1, POU2F3, and yes-associated protein (YAP). Numerous studies have proposed and validated classification approaches using transcriptomic sequencing, single-cell sequencing, and NMF methodologies. SCLC exhibits greater tumor heterogeneity compared to lung adenocarcinoma, featuring intermediate and mixed subtypes alongside classical patterns. Distinct drug vulnerabilities associated with these subtypes suggest potential for subtype-based precision treatments. Currently, the widely accepted classification system categorizes SCLC into four subtypes based on ASCL1, NEUROD1, and POU2F3 expression levels: SCLC-A, SCLC-N, SCLC-P, and SCLC-I. SCLC-I has shown immunosensitivity and survival advantages in studies like IMPOWER 133 using IHC, although real-world data remain limited [22].
ASCL1 and NEUROD1 are involved in deoxyribonucleic acid (DNA) and transcription factor binding, contrasting with POU2F3, which is exclusive to variant SCLC lacking neuroendocrine markers [23]. POU2F3, in conjunction with the Optic Atrophy 1 (OCA-T) complex, regulates cluster cell identity and susceptibility in cluster cell-like SCLC [24]. Previous studies (IMPOWER 133) reported subtype proportions as SCLC-A 51%, SCLC-N 23%, SCLC-I 18%, and SCLC-P 7%. Our study found proportions of SCLC-A 41.4%, SCLC-N 20.7%, SCLC-I 18.9%, and SCLC-P 18.9%, which are largely consistent with earlier findings.
Our study, being the first to explore SCLC subtype relationships in a real-world immune cohort, uncovered intriguing findings. Despite the established survival advantage of the I subtype in clinical trials, we unexpectedly found a significant survival disadvantage for the A subtype compared to the others. Analysis of clinical baseline data revealed that patients with a family history of cancer tended to exhibit the I subtype (6/11, 54.5%), which also correlated with higher rates of brain metastases at diagnosis (6/11, 54.5%). In contrast, the A subtype showed distinct characteristics but less favorable outcomes compared to other other subtypes, notably in family history (3/24, 12.5%) and brain metastases (3/24, 12.5%). These insights may inform future decisions on prophylactic cranial irradiation based on subtype. Regarding CD8-positive immune infiltration, no significant advantage was observed for the I subtype. Both P and I subtypes showed three patients with high infiltration, possibly due to our limited sample size. Despite this limitation, our study demonstrated stable standard errors, suggesting reliable findings [25].
Our study observed a poorer prognosis in the A subtype, initiated before the incorporation of ICIs into standard therapy, with over half of patients undergoing chemotherapy cycles before gradual inclusion of immunotherapy. Drawing from theories of subtype admixture and heterogeneity in prior literature, we speculate that initiating immunotherapy early may not maximize benefits for certain platinum-sensitive but immune-insensitive subtypes, like A. Instead, introducing immunotherapy after initial chemotherapy cycles might enhance survival advantages. Analyzing IHC scores of ASCL1, NEUROD1, and POU2F3 as quantitative variables yielded limited positive results, showing minimal correlation with prognosis, tumor response, and adverse events. However, significant differences emerged among subtypes based on these gene expression levels regarding prognosis, treatment response, and adverse events. Our hypothesis linking tumor subtype nature to cell subtype proportions was not supported, suggesting a lesser influence of positive gene expression levels on overall tumor characteristics. Alternatively, these cells might impact the tumor microenvironment via substance release, partially supported by CD8 + cell infiltration extents. Future large-scale clinical studies are essential to validate these hypotheses, potentially providing the most significant insights from our four-subtype SCLC classification. Additionally, subtype A displayed poorer immune infiltration, further explaining its inferior prognosis [19, 26].
Regarding subtype I, our research has revealed subtle distinctions in clinical features and prognosis compared to several other subtypes. Patients with a family history of tumors tend to exhibit subtype I, which seemingly confirms, from another perspective, that unlike other subtypes, subtype I may comprise a group of cells characterized by high drug resistance, plasticity, and certain stem cell-like traits. Furthermore, distinct from other subtypes, subtype I exhibits a higher epithelial-mesenchymal transition (EMT) score and a tendency to express mesenchymal features [27]. Consequently, due to these characteristics, subtype I is more prone to early systemic metastasis. In the prognostic study of IMPOWER133 by Gay [27], it was observed that SCLC-I achieved a significant survival advantage when treated with Etoposide plus Cisplatin (EP) plus atezolizumab compared to EP plus placebo, while in comparison to SCLC-A and SCLC-N, the administration of EP plus placebo did not exhibit any discernible disparities [17]. This suggests that subtype I may indicate a form of immune sensitivity rather than a prognostic determinant.
Regarding subtype N, previous studies considered NEUROD1 as a neuroendocrine gene similar to ASCL1, leading to the notion that these two subtypes might exhibit similar properties [11]. However, in our study, we observed a significant survival disadvantage in subtype A while we did not find a survival advantage in subtype N. Further research is needed to elucidate the subtype transition in N. Moreover, the standard deviation of OS in patients with subtype N was the lowest among the four groups, suggesting that subtype N may represent a relatively stable and well-established classification mechanism. Concerning subtype P, we did not observe a relatively poor prognosis in subtype P, and our investigation did not reveal any differences between smokers and non-smokers, which could be attributed to the limitation of not being able to further analyze the impact of secondhand smoke or the relatively small sample size. However, subtype P displayed the highest standard deviation in OS within our study, demonstrating apparent polarity. Some patients achieved long-term survival of up to 22 months, while over half of the patients had an OS of less than 9 months. Subtype P may require additional gene expression analysis to further refine its classification.
Our study also has its limitations. In addition to the inherent limitations of retrospective studies, our research faces several additional challenges. Based on previous literature, we believe there is no convincing evidence indicating that the status of PD-1 and PD-L1 affects the sensitivity of SCLC to immunotherapy. Consequently, we did not obtain the PD-1 and PD-L1 status of the patients in our cohort. Additionally, since most SCLC pathological specimens are obtained through biopsies and are therefore extremely valuable, obtaining additional sections could lead to the loss of these precious samples. Hence, we did not include these experiments in our study. We propose that future research should address this issue to further elucidate the relationship between PD-1 and PD-L1 status and the sensitivity of SCLC to immunotherapy.
On one hand, the number of patients who received immunotherapy and had available biopsy specimens was limited due to the recent integration of immunotherapy into standard care. On the other hand, the limited number of patients who underwent TRT and PCI hindered our ability to further classify and determine the potential benefits of TRT or PCI within the four subtypes. Furthermore, the conventional collaboration with pathologists in analyzing immunohistochemistry methods may somewhat limit the precision of the study. Regarding the further analysis of IHC, we attempted to use more standardized image processing methods, such as manual and automated counting with ImageJ software and measuring mean optical density. However, due to the rapid growth of SCLC, severe compression within the tumor, and the presence of inflammatory and stromal cells among the tumor cells, machine analysis yielded inaccurate results. After discussions with several pathologists, we opted to use the traditional H-score method for data analysis. The H-score method has inherent limitations, such as the subjectivity of visual scoring by pathologists. Despite employing three blinded pathologists for the analysis, we cannot guarantee complete objectivity.
Although investigating the relationship between radiation therapy and subtypes would hold significant clinical value, the conclusions drawn from such an analysis could be biased. Therefore, we did not explore the association between radiation therapy and subtypes. Overall, our study has yielded several intriguing findings. While some of these findings align with conclusions observed in our previous studies, there are also certain differences. Nonetheless, our article contributes valuable insights to the field and adds to the existing body of knowledge. Further research is warranted to delve into these possibilities in the future.
Conclusion
In a comprehensive cohort of ES-SCLC patients receiving immunotherapy, the I subtype achieved a significant survival advantage, while the A subtype exhibited a poorer prognosis compared to the other two subtypes. Furthermore, compared to the other two subtypes, the I subtype had a higher proportion of patients with early brain metastasis and a family history of tumors, while the A subtype had a lower proportion. Additionally, the A subtype was found to have relatively poorer immune infiltration.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AEs:
-
Adverse events
- AJCC:
-
American Joint Committee on Cancer
- ASCL1:
-
Achaete-scute family BHLH transcription factor 1
- CR:
-
Complete response
- CTLA-4:
-
Cytotoxic T-lymphocyte antigen 4
- DAB:
-
3,3'-Diaminobenzidine
- DNA:
-
Deoxyribonucleic acid
- dNLR:
-
Derived neutrophil-to-lymphocyte ratio
- EMT:
-
Epithelial-mesenchymal transition
- EP:
-
Etoposide plus Cisplatin
- ES-SCLC:
-
Extensive-stage small cell lung cancer
- FFPE :
-
Formalin-fixed paraffin-embedded
- ICIs:
-
Immune checkpoint inhibitors
- IHC:
-
Immunohistochemistry
- ITH:
-
Intra-tumor heterogeneity
- KM:
-
Kaplan-Meier
- KPS:
-
Karnofsky Performance Status Score
- NEUROD1:
-
Neurogenic differentiation factor 1
- NMF:
-
Non-negative matrix factorization
- OCA-T:
-
Optic Atrophy 1
- ORR:
-
Objective response rate
- OS:
-
Overall survival
- PBS:
-
Phosphate-buffered saline
- PCI:
-
Prophylactic cranial irradiation
- PD:
-
Progression disease
- PD-1:
-
Programmed cell death protein 1
- PD‑L1:
-
Programmed death ligand 1
- PFS:
-
Progression free survival
- POU2F3:
-
POU class 2 homeobox 3
- PR:
-
Partial response
- RECIST:
-
Response evaluation criteria in solid tumors
- SCLC:
-
Small cell lung cancer
- SD:
-
Stable disease
- THPA:
-
The Human Protein Atlas database (www.proteinatlas.org)
- TIME:
-
Tumor immune microenvironment
- TMB:
-
Tumor mutational burden
- TRT:
-
Thoracic radiation therapy
- YAP:
-
Yes-associated protein
References
Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3.
Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–54.
Remon J, Aldea M, Besse B, Planchard D, Reck M, Giaccone G, et al. Small cell lung cancer: a slightly less orphan disease after immunotherapy. Ann Oncol. 2021;32(6):698–709.
Rudin CM, Awad MM, Navarro A, Gottfried M, Peters S, Csőszi T, et al. Pembrolizumab or Placebo Plus Etoposide and Platinum as First-Line Therapy for Extensive-Stage Small-Cell Lung Cancer: Randomized, Double-Blind, Phase III KEYNOTE-604 Study. J Clin Oncol. 2020;38(21):2369–79.
Paz-Ares L, Dvorkin M, Chen Y, Reinmuth N, Hotta K, Trukhin D, et al. Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. The Lancet. 2019;394(10212):1929–39.
Ready NE, Ott PA, Hellmann MD, Zugazagoitia J, Hann CL, de Braud F, et al. Nivolumab Monotherapy and Nivolumab Plus Ipilimumab in Recurrent Small Cell Lung Cancer: Results From the CheckMate 032 Randomized Cohort. J Thorac Oncol. 2020;15(3):426–35
Hamilton G, Rath B. Immunotherapy for small cell lung cancer: mechanisms of resistance. Expert Opin Biol Ther. 2019;19(5):423–32.
Megyesfalvi Z, Barany N, Lantos A, Valko Z, Pipek O, Lang C, et al. Expression patterns and prognostic relevance of subtype-specific transcription factors in surgically resected small-cell lung cancer: an international multicenter study. J Pathol. 2022;257(5):674–86.
Baine MK, Hsieh MS, Lai WV, Egger JV, Jungbluth AA, Daneshbod Y, et al. SCLC Subtypes Defined by ASCL1, NEUROD1, POU2F3, and YAP1: A Comprehensive Immunohistochemical and Histopathologic Characterization. J Thorac Oncol. 2020;15(12):1823–35.
Denize T, Meador CB, Rider AB, Ganci ML, Barth JL, Kem M, et al. Concordance of ASCL1, NEUROD1 and POU2F3 transcription factor-based subtype assignment in paired tumour samples from small cell lung carcinoma. Histopathology. 2023;83(6):912–24.
Borromeo MD, Savage TK, Kollipara RK, He M, Augustyn A, Osborne JK, et al. ASCL1 and NEUROD1 Reveal Heterogeneity in Pulmonary Neuroendocrine Tumors and Regulate Distinct Genetic Programs. Cell Rep. 2016;16(5):1259–72.
Gay CM, Stewart CA, Park EM, Diao L, Groves SM, Heeke S, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell. 2021;39(3):346-60.e7.
Böttger F, Semenova EA, Song JY, Ferone G, van der Vliet J, Cozijnsen M, et al. Tumor Heterogeneity Underlies Differential Cisplatin Sensitivity in Mouse Models of Small-Cell Lung Cancer. Cell Rep. 2019;27(11):3345-58.e4.
Cardnell RJ, Li L, Sen T, Bara R, Tong P, Fujimoto J, et al. Protein expression of TTF1 and cMYC define distinct molecular subgroups of small cell lung cancer with unique vulnerabilities to aurora kinase inhibition, DLL3 targeting, and other targeted therapies. Oncotarget. 2017;8(43):73419–32.
Chung HC, Piha-Paul SA, Lopez-Martin J, Schellens JHM, Kao S, Miller WH Jr, et al. Pembrolizumab After Two or More Lines of Previous Therapy in Patients With Recurrent or Metastatic SCLC: Results From the KEYNOTE-028 and KEYNOTE-158 Studies. J Thorac Oncol. 2020;15(4):618–27.
Hellmann MD, Callahan MK, Awad MM, Calvo E, Ascierto PA, Atmaca A, et al. Tumor Mutational Burden and Efficacy of Nivolumab Monotherapy and in Combination with Ipilimumab in Small-Cell Lung Cancer. Cancer Cell. 2019;35(2):329.
Horn L, Mansfield AS, Szczęsna A, Havel L, Krzakowski M, Hochmair MJ, et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N Engl J Med. 2018;379(23):2220–9.
Chan JM, Quintanal-Villalonga Á, Gao VR, Xie Y, Allaj V, Chaudhary O, et al. Signatures of plasticity, metastasis, and immunosuppression in an atlas of human small cell lung cancer. Cancer Cell. 2021;39(11):1479-96.e18.
Sabari JK, Lok BH, Laird JH, Poirier JT, Rudin CM. Unravelling the biology of SCLC: implications for therapy. Nat Rev Clin Oncol. 2017;14(9):549–61.
Jimbo N, Ohbayashi C, Takeda M, Fujii T, Mitsui S, Tsukamoto R, et al. POU2F3-Expressing Small Cell Lung Carcinoma and Large Cell Neuroendocrine Carcinoma Show Morphologic and Phenotypic Overlap. Am J Surg Pathol. 2024;48(1):4–15.
Pantelidou C, Sonzogni O, De Oliveria TM, Mehta AK, Kothari A, Wang D, et al. PARP Inhibitor Efficacy Depends on CD8(+) T-cell Recruitment via Intratumoral STING Pathway Activation in BRCA-Deficient Models of Triple-Negative Breast Cancer. Cancer Discov. 2019;9(6):722–37.
George J, Lim JS, Jang SJ, Cun Y, Ozretić L, Kong G, et al. Comprehensive genomic profiles of small cell lung cancer. Nature. 2015;524(7563):47–53.
Huang YH, Klingbeil O, He XY, Wu XS, Arun G, Lu B, et al. POU2F3 is a master regulator of a tuft cell-like variant of small cell lung cancer. Genes Dev. 2018;32(13–14):915–28.
Wu XS, He XY, Ipsaro JJ, Huang YH, Preall JB, Ng D, et al. OCA-T1 and OCA-T2 are coactivators of POU2F3 in the tuft cell lineage. Nature. 2022;607(7917):169–75.
Acheampong E, Abed A, Morici M, Bowyer S, Amanuel B, Lin W, et al. Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cells. 2020;9(11):2393.
Park S, Noh JM, Choi YL, Chi SA, Kim K, Jung HA, et al. Durvalumab with chemoradiotherapy for limited-stage small-cell lung cancer. Eur J Cancer. 2022;169:42–53.
Gay CM, Stewart CA, Park EM, Diao L, Groves SM, Heeke S, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell. 2021;39(3):346–60 e7.
Acknowledgements
Not applicable
Funding
This work was supported by the Beijing Xisike Clinical Oncology Research Foundation (grant number Y-2019AZMS-0522) and the Xisike-2019 Qilu Oncology Research Fund Project (grant number Y-QL2019-0149).
Author information
Authors and Affiliations
Contributions
YZ, LJN, and ZFG conceived and designed the analysis. ZWT, LQ, LJN, and ZFG collected the data. NYL, LJN, ZY, and FAL contributed to the analysis. FAL, LJX, LJN, and ZWT performed the analysis. LJN and ZRY wrote the paper. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Our research performed in accordance with the performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shandong Provincial Hospital, with the ethics application number 2021–1017-1. Written informed consent was obtained from all subjects or their legal guardians.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Zhang, W., Zhao, Y. et al. Characteristics of molecular subtypes and cinical outcomes in the immunotherapy Queue of extensive-stage small cell lung cancer patients. BMC Pulm Med 24, 423 (2024). https://doi.org/10.1186/s12890-024-03221-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-024-03221-4