
Abstract
Background
Accumulating evidence indicates that abnormal foot posture are risk factors for knee osteoarthritis (OA). However, the relationship between foot posture and tibiofemoral contact force (CF) during habitual weight-bearing activities remains unclear. This study aimed to determine the association between tibiofemoral CF and foot posture while walking.
Methods
In total, 18 patients with knee OA and 18 healthy individuals participated in this cross-sectional study. Foot parameters were evaluated by Foot Posture Index (FPI), Staheli Arch Index (SAI), hallux valgus angle, calcaneus inverted angle relative to the floor as a static rearfoot posture, navicular height, and toe grip strength. In addition, all participants underwent kinetic and kinematic measurements during a self-selected speed gait. The measurement device used was the three-dimensional motion analysis system with a sampling rate of 120 Hz. The musculoskeletal model, which has 92 Hill-type muscle–tendon units with 23 degrees of freedom, was used to calculate tibiofemoral CF. Partial correlations was used to investigate the association between foot parameters and total, medial, and lateral tibiofemoral CF of the first and second peaks while controlling for gait speed.
Results
A significant negative correlation was observed between Walking SAI and first peak medial tibiofemoral CF in control participants (r = -0.505, p = 0.039). SAI was also significantly positively correlated with first peak medial tibiofemoral CF in patients with knee OA (r = 0.482, p = 0.042).
Conclusions
Our findings revealed a correlation between the medial first peak tibiofemoral CF and the SAI. This study indicates that people with knee OA and flatfoot have excessive first medial tibiofemoral CF during walking.
Similar content being viewed by others

Background
Knee osteoarthritis (KOA), a highly prevalent disease in older adults, leads to chronic pain, stiffness, and disability. Various factors contribute toward dynamic mechanical loading of the knee joint during walking that can lead to joint pain [1], cartilage damage [2], and bone deformities [3]. Further, the development and progression of KOA is affected by excessive rotational and/or contact loading [2, 3]. Although radiographic KOA is rare in Japanese people aged < 40 years, its prevalence among adults aged > 40 years has been demonstrated to be 42.6% in men and 62.4% in women [4].
Many studies have assessed the association between tibiofemoral joint (TFJ) contact loading by knee adduction moment (KAM) and knee function or alignment. For example, Winby et al. [5] demonstrated that KAM during walking was influenced by knee-spanning muscle contractions in healthy individuals, and Sharma et al. [6] found a negative association between KAM during walking and joint space width in KOA patients. However, limited studies have investigated the relationship between foot posture and function and mechanical loads on the knee joint. Increased rearfoot eversion, rearfoot internal rotation, forefoot inversion, and foot progression angle (FPA) are associated with reduced KAM during walking [7, 8], and accumulating evidence indicates that KOA patients have abnormal foot posture and foot function, such as hallux valgus [9], pronated foot [10], flatfoot [11], and decreased toe grip strength (TGS) [12]. Notably, Gross et al. [11] found a significant association between flatfoot measured by footprint data and cartilage damage of the TFJ.
In clinical practice, foot evaluation is difficult using a three-dimensional (3D) motion analysis device (e.g., the Oxford Foot Model) owing to the time and cost involved. Many patients prefer to undergo physiotherapy and insole insertion after static foot evaluation that can be easily performed in clinical practice; hence, its relationship with TFJ loads must be determined. Rearfoot angle (RFA), navicular drop, and footprint as a uniplanar assessment of foot posture are often used [13]. In contrast, the Foot Posture Index (FPI) is a multi-planar tool that has gained popularity recently. Akaltun et al. [10] reported that foot posture assessed by FPI shows abnormalities such as more pronation or supination in patients with knee OA than healthy controls.
Many studies have used KAM as a surrogate marker of TFJ contact loading during activities, such as walking [6]. KAM is based on inverse dynamics, which only accounts for external parameters, i.e., ground reaction forces (GRF) and joint angles. Musculoskeletal modeling enables the calculation of muscle forces (MF) and joint contact forces and gives insights into the internal loading of body [5]. Notably, Lerner et al. [14] developed a model in OpenSim to accurately assess medial and lateral tibiofemoral contact force (CF) in a tibiofemoral implant study. This model uses subject-specific knee joint medial and lateral compartment contact locations and joint alignment to more accurately estimate medial and lateral tibiofemoral CF (MCF, LCF). Moreover, a systematic review investigating the correlation between tibiofemoral CFs and external joint moments found that the MCF and total tibiofemoral CF (TCF) in the first half of stance can be predicted using external joint moments. However, worse correlations were found for the peak in the second half of stance and LCF [15]. Therefore, while investigating the second peak in the stance phase and lateral knee joint loading, it is better to calculate tibiofemoral CF using musculoskeletal models.
Despite these findings, the biomechanical relationship between foot posture and function and tibiofemoral CF remains unclear. Therefore, this study aimed to clarify the association between tibiofemoral CF and foot posture and function during walking in KOA patients. We hypothesized that participants with pronated foot posture and function, such as excessive flatfoot, hallux valgus, and lower TGS, have increased tibiofemoral CF during walking.
Methods
Participants
This cross-sectional study included outpatients with KOA diagnosed by their treating physician in orthopedics at Kashiba Asahigaoka Hospital and healthy adults from participants in a health promotion project conducted by Koryo Town, Nara, Japan, and from the staff members of Kashiba Asahigaoka Hospital. All participants were recruited between March 2019 and January 2020.
The inclusion criteria for the participants with medial KOA were as follows: Age > 45 years and radiographic changes with Kellgren-Lawrence (KL) grade of 2 or higher in the medial tibiofemoral compartment. The exclusion criteria for the participants with medial KOA were as follows: A history of any other orthopedic injury in the lower extremities, neurological injury, rheumatoid arthritis, joint surgery in lower extremities, lateral KOA, or use of an assistive device. For control participants, the inclusion criteria were as follows: age > 45 years, walking independently without any ambulatory assistive device, and no pain in the knee joint, and we excluded those with any previous surgical treatment for the lower limbs or trunk or known neuromuscular or musculoskeletal pathologies.
Gait analysis
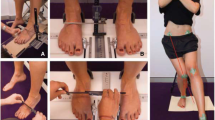
Six VICON MX-F20 cameras (Vicon Metrics, Oxford, UK) and four floor-embedded force platforms (2 × 9281B, Kistler Instrument Corporation, Switzerland; 2 × AMTI BP400600, Advanced Mechanical Technology Inc., USA) were used to measure 3D kinematics and GRF with a sampling rate of 120 Hz, respectively. The plug-in-gait full body 39 markers set was used [16]. These markers were attached to each participant’s skin at the following anatomical landmarks: forehead, back of the head, shoulder, 7th cervical vertebra (C7), 10th thoracic vertebra, upper arm, elbow, forearm, wrist, finger, right back, anterior superior iliac spines (ASIS), posterior superior iliac spines (PSIS), thigh, lateral knee, tibia, lateral ankles, heels, and second metatarsal heads.
Participants were asked to walk at a self-selected speed, barefoot, along a flat 8-m walkway. Three successful walking trials were recorded. Stance phases during gait were determined using vertical GRF data. GRFs were low-pass filtered using 10-Hz cut-off frequencies for walking. The threshold value for the stance phase was a GRF of 25 N or more in the vertical direction. The walking speed was calculated from the distance of the right and left second metatarsal head marker positions during 6 steps and the time taken.
Musculoskeletal model
A musculoskeletal model with 18 body segments and 92 muscle–tendon actuators in OpenSim was used to compute the tibiofemoral CF [14, 17]. The model can calculate accurate medial and lateral CFs, strictly reflecting the subject-specific knee joint alignment in the participant's lower extremity radiograph [14]. In this knee mechanism, the medial and lateral TFJs share all forces transmitted between the femur and tibia and resolve them as the medial and lateral tibiofemoral CFs required to balance the net reaction forces and frontal-plane moments across the TFJ. Correspondingly, the knee remains a single degree of freedom (DOF) joint with motion only in the sagittal plane. Therefore, the model includes a spline function on the knee axis, which takes into account the anterior–posterior translations [14, 17]. The model has only a single DOF for dorsi-/plantarflexion and a single axis for the ankle joint. For each participant, subject-specific models were created based on the approach reported by Lerner et al. [14]. In the KOA group, standing anatomical motion capture markers were supplemented with anteroposterior weight-bearing radiograph of the lower-extremity [14, 18]. The dimensions of each body segment in the model were scaled based on relative distances between pairs of markers obtained from a motion-capture system and the corresponding virtual marker locations in the model. Next, we modified each participant’s scaled model and created a subject-specific model by specifying their lower extremity alignment from the radiographs in KOA patients. An anteroposterior radiograph of the participant's lower-extremity was used to determine the subject-specific alignment for the musculoskeletal model. The tibiofemoral alignment was found by drawing lines connecting the hip, knee, and ankle joint centers, which were defined as the center of the femoral head, center of the femoral condyles, and midpoint of the medial and lateral margins of the ankle, respectively. The tibiofemoral alignment was adjusted only for the healthy adults using the marker information [19]. The model was then used to calculate joint angles and moments during walking trials using OpenSim inverse kinematics and inverse dynamics, respectively. MF were estimated using static optimization. Minimizing of activation squared was used as the static optimization criterion for the calculation of MF. These results were used to calculate the joint reaction force (JRF) in OpenSim.
Foot assessment
The Foot Posture Index (FPI) was calculated in a relaxed standing position to assess foot posture based on a six-item standard protocol [20]. The FPI included the following: 1) talar head palpation, 2) supra and infra lateral malleolar curvature, 3) calcaneal frontal plane position, 4) prominence in the region of the talonavicular joint, 5) congruence of the medial longitudinal arch, and 6) abduction/adduction of the forefoot on the rear foot. Each item was scored on a scale of –2, –1, 0, + 1, and + 2 (0 for neutral, –2 for clear signs of supination, and + 2 for clear signs of pronation) [20, 21]. The total score ranged from –12 to + 12, with a larger positive value indicating a more pronated foot. For foot type identification, normative values with scores of ≥ 6 represent a pronated foot type; those with scores of 0–5 represent a neutral foot; and those with scores of ≤ − 1 represent a supinated foot [20, 21]. The inter-rater reliability for measuring FPI was high (ICC > 0.8) [22].
A force platform (WinFDM; Zebris, Isny im Allgäu, Germany) was used to measure static and dynamic footprint data. Static footprint data were recorded for 10 s with a participant standing on the platform with double limb support. Dynamic footprint data were collected during walking at a self-selected speed on the platform. The Staheli Arch Index (SAI), the ratio of the smallest width of the midfoot to the greatest width of the rearfoot [23], was calculated from footprint data. The value of the SAI increases with increasingly planus foot morphology and takes on a value of zero with cavus foot morphology. The widths were measured by ImageJ software [24]. A previous validity study indicated a moderately significant correlation between SAI measurements of foot morphology and radiological measurements of total foot morphology [23]. The average value of two measurements was used in the analysis. The inter-rater and intra-rater reliability for measuring the SAI was excellent (ICC > 0.9, respectively) [25].
The hallux valgus angle (HVA) and calcaneus inverted angle relative to the floor (CIA) were measured using a goniometer. HVA was the angle formed by the first metatarsal bone and the proximal phalanx of the hallux [26]. Janssen et al. [26] investigated the reliability, and concurrent validity of universal goniometer measurements of the HVA compared to those of radiographs and found a good intraclass correlation coefficient. CIA was defined as the angle formed by the line joining the bottom of the calcaneal tuberosity with the enthesis of the Achilles tendon and a line perpendicular to floor [27]. The reliability of CIA measurements was calculated by 2 testers for 20 participants. The inter-rater and intra-rater reliability for measuring the CIA was good (ICC: 0.92 and 0.86, respectively).
Navicular height (NH)/foot length was measured as the length from the floor to the top of the navicular tuberosity [28]. The measure of NH in a standing or sitting position demonstrated good intra- and inter-rater reliability [28].
Navicular drop test (ND-t) was recorded as the difference in NH between relaxed standing and sitting position [27]. ND-t had moderate intra- and inter-rater reliability [28].
TGS was measured using a toe grip dynamometer (T.K.K.3362; Takei Scientific Instruments Co., Ltd., Niigata, Japan) with participants sitting upright [29]. Participants gripped the grip bar with maximal effort for about 3 s. The average value of two measurements was used in the analysis. In this measurement protocol, substantial to almost perfect inter- and intra-rater reliability was found in people aged 60–79 years [29].
Statistical analysis
Gait trial data were normalized by time to 0%–100% of the stance phase in the gait cycle. Each tibiofemoral CF, normalized by body weight (BW), was represented as a time series throughout the stance phase (SP). The first and second peaks of the TCF, MCF, and LCF were identified. The maximum tibiofemoral CF during 0%–50% of SP was defined as the first peak, and the maximum tibiofemoral CF during 51%–100% of SP was defined as the second peak.
Differences in demographic data, FPI, Standing SAI, Walking SAI, HVA, CIA, NH, ND-t, TGS, and gait speed between the groups were evaluated by a t-test. Sex differences were examined by chi-square test. Analysis of covariance (ANCOVA) was used to compare the tibiofemoral CFs between the KOA and Healthy groups adjusting for gait speed. For the relationship between foot posture or function and tibiofemoral CF, correlation coefficients of tibiofemoral CF with foot parameters that were significantly different between the groups were calculated. If a significant correlation between tibiofemoral CF and a foot parameter was found for the first peak, we then additionally performed a correlation between the MF at the peak and the foot parameter. The correlation between walking speed and tibiofemoral CF or foot parameters was further calculated. The Shapiro–Wilk test was used to determine the normal distributions. In normally distributed data, Pearson’s correlation tests were used. Partial correlations were used to assess relationship between tibiofemoral CFs and foot parameters while controlling for gait speed.
All statistical analyses were performed using SPSS Statistics for Windows, version 22.0 (IBM Corp, Tokyo, Japan). A p-value of < 0.05 was considered significant.
Results
Eighteen patients with medial KOA (4 men and 14 women; mean age: 60.17 ± 6.96 years) and 18 healthy adults (4 men and 14 women; mean age: 62.78 ± 8.58 years) were included in this study. Participant characteristics are shown in Table 1. There were no significant differences in age, height, and sex between KOA patients and controls. The participant weight was significantly higher in the KOA patient group than in the control group. KOA patients walked significantly slower than the controls. Foot assessment revealed no significant differences in the FPI, HVA, CIA, NH, and TGS between KOA patients and controls (Table 2). The Standing SAI, Walking SAI, and ND-t were significantly higher in KOA patients than in controls. Figure 1 shows the experimental results for the total tibiofemoral CF and medial and lateral tibiofemoral CF values. No differences were detected in the first and second peak medial, lateral, and total tibiofemoral CF values (Table 3). Figure 2 shows the experimental results for the MF of the knee-spanning muscle values. None of the parameters correlated with walking speed.

Force on the total, medial, and lateral tibiofemoral joint during the stance phase. Data are presented as mean ± standard deviation. Controls and patients with knee OA are presented as blue and red lines, respectively. CF, Tibiofemoral contact force

Muscle forces for knee-spanning muscles during the stance phase. Data are presented as mean ± standard deviation. Controls and patients with knee OA are presented as blue and red lines, respectively. Lh, long head. Sh, short head. Med, medialis. Lat, lateralis
According to Partial correlations coefficient, the first peak MCF was significantly negatively correlated with SAI during walking (r, -0.505; p, 0.039) in KOA patients. The negative correlation indicates that for a people with a lower arch there is greater contact force in KOA. However, in healthy adults, the first peak MCF was significantly positively correlated with SAI during walking (r, 0.482; p, 0.042) (Fig. 3).

Scatter plot with the best fit line (solid line) for Partial correlations. The correlation analysis was performed between first medial CF and SAI for controls (diamonds) and knee OA (squares). CF, Tibiofemoral contact force. SAI, Staheli Arch Index
No significant correlation was found between the first and second peak values of the CF and Standing SAI and ND-t. No significant correlation was found between MF and SAI.
Discussion
This cross-sectional study showed that flatfoot expressed as SAI during walking increases medial knee joint loading. To our knowledge, this study is the first to investigate the relationship between CF, calculated using the musculoskeletal model, and foot posture in patients with KOA. Many researchers have also reported a relationship between KOA and the foot parameters. Our research extends others’ work in this area.
Our results are consistent with those of previous musculoskeletal model-based studies [5, 30]. Figures 1 and 2 show the CF and MF values, respectively. These are similar to the waveforms in previous studies [5, 30]. The 12-month longitudinal observational study indicated that a medial knee joint loading was associated with an increased risk of medial knee OA structural progression [2]. Peak TCF of about 3–4 times BW was calculated. Tibiofemoral CFs showed no statistically significant differences between the groups in terms of first and second peaks. This result is consistent with that of a similar previous study [31]. Merireles et al. [31] reported that tibiofemoral CFs in patients with early KOA (KL ≤ 2) were not significantly different from those in healthy adults. Although the magnitudes of first and second peaks in the KOA group in this study have different trends compared to those in the study by Merireles et al. [31], the majority of patients had KL ≤ 2, and the relative peaks of tibiofemoral CFs between the groups were nonsignificant. In patients with KOA, strategies to reduce the loading on the knee joint during gait have been reported [32]. This may be due to the fact that the analysis in this study focused on static foot parameters and did not exclude the effects of other joints and other factors.
Our results showed that the correlations between the first peak MCF and Walking SAI were negative in KOA patients and positive in healthy controls. This means that the flatter the foot is in patients with KOA, the higher the MCF. In this study, of all of the tibiofemoral CFs, only the MCF was associated with Walking SAI, which are most affected by the moment arm length. KAM contributes to the tibiofemoral CFs. The moment arm is determined by the distance of GRF from the center of the knee joint. The position of the calcaneus during walking in healthy participants is different from that in patients with foot problems. The lateral shift of the calcaneus during walking in children with flatfoot results in a low first peak KAM because of the point of GRF application due to the calcaneal position [33]. In fact, shoe modifications produce a lateral shift in the point of GRF and reduce the first peak KAM in healthy adults [34]. Therefore, flat feet in healthy adults may bring the GRF closer to the center of the knee joint and have the potential to indirectly decrease tibiofemoral CF. KOA patients achieve a relatively flatter position of the foot while walking as compared to healthy adults. Further, previous research has shown that people with flatfoot show a high peak pressure for the medial foot area during walking [35]. In people with flatfoot, the center of pressure may be different during medial shift of the foot; as a result, the KAM moment arm is expected to increase. Moreover, the range of motion of the rearfoot is smaller in KOA patients than in healthy participants [36]. Therefore, the lateral shift of the calcaneus is unlikely to occur in KOA patients.
In healthy and KOA participants, only the MCF was associated with SAI, but the LCF was not significantly associated with SAI, probably due to the GRF and knee joint position.
MF showed no significant correlation with SAI during the first peak MCF. Muscles that do not pass through the ankle joint or foot are unlikely to be affected by SAI. The gastrocnemius is the only muscle that passes through the knee and ankle joints. However, previous studies showed no significant difference in muscle activity in the gastrocnemius during walking between people with flatfoot and healthy individuals [37]. These are similar to the results in the previous study [37], except for the gastrocnemius muscle, we could not draw a direct relationship as no muscle extends from the knee joint to the foot.
There was a significant difference in ND-t, Standing SAI, and Walking SAI between the healthy and KOA groups. During most weight-bearing activities, the posture and motion of the foot and knee are coupled within a closed kinematic chain, such as the movements in the horizontal plane and frontal plane [36]. However, despite the fact that Walking SAI is correlated, ND-t and Standing SAI had no correlation with tibiofemoral CF during walking. Controversies regarding static foot alignment reflecting a dynamic foot morphology exist [38, 39]. Additionally, the dynamic foot motion during walking in KOA patients differ from that in healthy adults [36]. Therefore, it is highly possible that the SAI evaluated during walking represented the tibiofemoral CF during walking. Furthermore, closed chain coupling may link excessively planus foot morphology to excessive internal rotation of the lower extremity [40]. However, in this study, only tibiofemoral CF was used, and foot, ankle, knee, or hip kinematics and rotational stress were not investigated.
This study had some limitations. First, the number of males was fewer than that of females. Future studies have to include an equal number of male and female participants. Additionally, the sample size used in this study was small, potentially leading to inconclusive or insignificant results. However, our results for the control and patients with KOA were comparable with those of previous studies. Second, the model had only a single DOF for flexion/extension and a single axis for the knee joint. Therefore, internal/external rotation and dynamic adduction/abduction movement during knee joint movement could not be considered. Third, the model of the ankle joint and midfoot motion used herein was for dorsiflexion and plantarflexion only. Therefore, this model did not accurately reflect the movement of the coronal plane motion in the subtalar and metatarsophalangeal joints. Along with them, the FPA has not been able to be considered. However, the GRF was actually assessed in this study; its relationship with the position of the center of gravity or knee joint was clarified using marker trajectory data. Fourth, we assumed the same 'normal' motor control/muscle recruitment strategy between healthy people and patients with OA in the musculoskeletal simulations. Unlike the EMG-informed model, it is likely that OA patient characteristics, including co-contraction, are not reflected by the model in this study. However, the use of an EMG-informed model in future studies may better characterize muscle contractions in healthy and OA patients. Furthermore, gait speed in patients with knee OA was much slower than that in controls. Thus, different results may be obtained in patients with knee OA who maintain gait speed. Finally, further studies are needed to investigate detailed relationships using more discriminating foot morphology indexes. Future studies directed toward investigating patients diagnosed with pathological foot positions or functions are warranted.
Conclusions
The first peak medial tibiofemoral CF was significantly correlated with the SAI. The findings reveal the relationship between cavus foot and tibiofemoral CF during walking in patients with knee OA. This study suggests that patients with knee OA and flatfoot have excessive first MCF during walking.
Availability of data and materials
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
Abbreviations
- 3D:
-
Three-dimensional
- ASIS:
-
Anterior superior iliac spines
- BW:
-
Body weight
- CF:
-
Contact force
- CIA:
-
Calcaneus inverted angle
- DOF:
-
Degree of freedom
- FPI:
-
Foot Posture Index
- GRF:
-
Ground reaction forces
- HVA:
-
Hallux valgus angle
- KAM:
-
Knee adduction moment
- KL:
-
Kellgren-Lawrence
- KOA:
-
Knee osteoarthritis
- MF:
-
Muscle forces
- NH:
-
Navicular height
- ND-t:
-
Navicular drop test
- PSIS:
-
Posterior superior iliac spines
- RFA:
-
Rearfoot angle
- SAJ:
-
Staheli Arch Index
- SP:
-
Stance phase
- TFI:
-
Tibiofemoral joint
- TGS:
-
Toe grip strength
References
Mohd Sharif NA, Usman J, Wan Safwani WKZ, Siew Li G, Abdul Karim S, Mohamed NA, et al. Effects of simple knee sleeves on pain and knee adduction moment in early unilateral knee osteoarthritis. Proc Inst Mech Eng H. 2019;233:1132–40. https://doi.org/10.1177/0954411919874614.
Bennell KL, Bowles KA, Wang Y, Cicuttini F, Davies-Tuck M, Hinman RS. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Ann Rheum Dis. 2011;70:1770–4. https://doi.org/10.1136/ard.2010.147082.
Kainz H, Killen BA, Campenhout AV, Desloovere K, Aznar JMG, Shefelbine S, et al. ESB Clinical Biomechanics Award 2020: pelvis and hip movement strategies discriminate typical and pathological femoral growth - insights gained from a multi-scale mechanobiological modelling framework. Clin Biomech (Bristol Avon). 2021;87:105405. https://doi.org/10.1016/j.clinbiomech.2021.105405.
Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab. 2009;27:620–8. https://doi.org/10.1007/s00774-009-0080-8.
Winby CR, Lloyd DG, Besier TF, Kirk TB. Muscle and external load contribution to knee joint contact loads during normal gait. J Biomech. 2009;42:2294–300. https://doi.org/10.1016/j.jbiomech.2009.06.019.
Sharma L, Hurwitz DE, Thonar EJ, Sum JA, Lenz ME, Dunlop DD, et al. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum. 1998;41:1233–40. https://doi.org/10.1002/1529-0131(199807)41:7%3c1233::AID-ART14%3e3.0.CO;2-L.
Levinger P, Menz HB, Morrow AD, Bartlett JR, Feller JA, Bergman NR. Relationship between foot function and medial knee joint loading in people with medial compartment knee osteoarthritis. J Foot Ankle Res. 2013;6:33. https://doi.org/10.1186/1757-1146-6-33.
Fong ICD, Li WSC, Tai WKJ, Tsang TWR, Zhang JH, Chen TLW, et al. Effect of foot progression angle adjustment on the knee adduction moment and knee joint contact force in runners with and without knee osteoarthritis. Gait Posture. 2018;61:34–9. https://doi.org/10.1016/j.gaitpost.2017.12.029.
Shih KS, Chien HL, Lu TW, Chang CF, Kuo CC. Gait changes in individuals with bilateral hallux valgus reduce first metatarsophalangeal loading but increase knee abductor moments. Gait Posture. 2014;40:38–42. https://doi.org/10.1016/j.gaitpost.2014.02.011.
Akaltun MS, Koçyiğit BF. Assessment of foot posture and related factors in patients with knee osteoarthritis. Arch Rheumatol. 2021;36:267–73. https://doi.org/10.46497/ArchRheumatol.2021.8354.
Gross KD, Felson DT, Niu J, Hunter DJ, Guermazi A, Roemer FW, et al. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res. 2011;63:937–44. https://doi.org/10.1002/acr.20431.
Uritani D, Fukumoto T, Myodo T, Fujikawa K, Usui M, Tatara D. The association between toe grip strength and osteoarthritis of the knee in Japanese women: a multicenter cross-sectional study. PLoS One. 2017;12:e0186454. https://doi.org/10.1371/journal.pone.0186454.
Langley B, Cramp M, Morrison SC. Clinical measures of static foot posture do not agree. J Foot Ankle Res. 2016;9:1–6. https://doi.org/10.1186/s13047-016-0180-3 (eCollection).
Lerner ZF, DeMers MS, Delp SL, Browning RC. How tibiofemoral alignment and contact locations affect predictions of medial and lateral tibiofemoral contact forces. J Biomech. 2015;48:644–50. https://doi.org/10.1016/j.jbiomech.2014.12.049.
Holder J, Trinler U, Meurer A, Stief F. A systematic review of the associations between inverse dynamics and musculoskeletal modeling to investigate joint loading in a clinical environment. Front Bioeng Biotechnol. 2020;8:603907. https://doi.org/10.3389/fbioe.2020.603907.
Davis RB, Õunpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Hum Mov Sci. 1991;10:575–87. https://doi.org/10.1016/0167-9457(91)90046-Z.
Delp SL, Loan JP, Hoy MG, Zajac FE, Topp EL, Rosen JM. An interactive graphics-based model of the lower extremity to study o surgical procedures. IEEE Trans Biomed Eng. 1990;37:757–67.
Lerner ZF, Board WJ, Browning RC. Pediatric obesity and walking duration increase medial tibiofemoral compartment contact forces. J Orthop Res. 2016;34:97–105. https://doi.org/10.1002/jor.23028.
Stief F, Feja Z, Holder J, van Drongelen S, Adolf S, Braun S, et al. Non-invasive determination of frontal plane lower limb alignment using motion capture technique - an alternative for full-length radiographs in young patients treated by a temporary hemiepiphysiodesis? Gait Posture. 2020;79:26–32. https://doi.org/10.1016/j.gaitpost.2020.04.011.
Redmond AC, Crosbie J, Ouvrier RA. Development and validation of a novel rating system for scoring standing foot posture: the Foot Posture Index. Clin Biomech (Bristol Avon). 2006;21:89–98. https://doi.org/10.1016/j.clinbiomech.2005.08.002.
Redmond AC, Crane YZ, Menz HB. Normative values for the Foot Posture Index. J Foot Ankle Res. 2008;1:6. https://doi.org/10.1186/1757-1146-1-6.
McLaughlin P, Vaughan B, Shanahan J, Martin J, Linger G. Inexperienced examiners and the Foot Posture Index: a reliability study. Report 26. Man Ther. 2016;26:238–40. https://doi.org/10.1016/j.math.2016.06.009.
Maes R, Dojcinovic S, Andrianne Y, Burny F. Study of the plantar arch: correlations between podometrical and radiological parameters. Results of a prospective study of 79 cases. Rev Med Brux. 2006;27:422–9.
Abramoff MD, Magelhaes PJ, Ram SJ. Image processing with ImageJ. Biophoton Int. 2004;11:36–42.
Zuil-Escobar JC, Martínez-Cepa CB, Martín-Urrialde JA, Gómez-Conesa A. Medial longitudinal arch: accuracy, reliability, and correlation Between navicular drop test and footprint parameters. J Manipulative Physiol Ther. 2018;41:672–9. https://doi.org/10.1016/j.jmpt.2018.04.001.
Janssen DM, Sanders AP, Guldemond NA, Hermus J, Walenkamp GH, Van Rhijn LW. A comparison of hallux valgus angles assessed with computerised plantar pressure measurements, clinical examination and radiography in patients with diabetes. J Foot Ankle Res. 2014;7:33. https://doi.org/10.1186/1757-1146-7-33.
Ohi H, Iijima H, Fukutani N, Aoyama T, Kaneda E, Ohi K, et al. Varus thrust visualized during gait was associated with inverted foot in patients with knee osteoarthritis: an exploratory study. Gait Posture. 2018;61:269–75. https://doi.org/10.1016/j.gaitpost.2018.01.020.
Deng J, Joseph R, Wong CK. Reliability and validity of the sit-to-stand navicular drop test: do static measures of navicular height relate to the dynamic navicular motion during gait? J Stud Phys Ther Res. 2010;2:21–8.
Uritani D, Fukumoto T, Matsumoto D. Intrarater and interrater reliabilities for a toe grip dynamometer. J Phys Ther Sci. 2012;24:639–43. https://doi.org/10.1589/jpts.24.639.
Gerus P, Sartori M, Besier TF, Fregly BJ, Delp SL, Banks SA, et al. Subject-specific knee joint geometry improves predictions of medial tibiofemoral contact forces. J Biomech. 2013;46:2778–86. https://www.sciencedirect.com/science/article/pii/S0021929013004144#f0020.
Meireles S, De Groote FD, Reeves ND, Verschueren S, Maganaris C, Luyten F, et al. Knee contact forces are not altered in early knee osteoarthritis. Gait Posture. 2016;45:115–20. https://www.sciencedirect.com/science/article/pii/S0966636216000175#fig0010.
Iijima H, Shimoura K, Ono T, Aoyama T, Takahashi M. Proximal gait adaptations in individuals with knee osteoarthritis: a systematic review and meta-analysis. J Biomech. 2019;87:127–41. https://doi.org/10.1016/j.jbiomech.2019.02.027.
Byrnes SK, Wearing S, Böhm H, Dussa CU, Horstmann T. Effects of idiopathic flatfoot deformity on knee adduction moments during walking. Gait Posture. 2021;84:280–6. https://doi.org/10.1016/j.gaitpost.2020.12.021.
Haim A, Rozen N, Dekel S, Halperin N, Wolf A. Control of knee coronal plane moment via modulation of center of pressure: a prospective gait analysis study. J Biomech. 2008;41:3010–6. https://doi.org/10.1016/j.jbiomech.2008.07.029.jbiomech.2008.07.029.
Buldt AK, Forghany S, Landorf KB, Levinger P, Murley GS, Menz HB. Foot posture is associated with plantar pressure during gait: A comparison of normal, planus and cavus feet. Gait Posture. 2018;62:235–40. https://doi.org/10.1016/j.gaitpost.2018.03.005.
Levinger P, Menz HB, Morrow AD, Feller JA, Bartlett JR, Bergman NR. Foot kinematics in people with medial compartment knee osteoarthritis. Rheumatology (Oxford). 2012;51:2191–8. https://doi.org/10.1093/rheumatology/kes222.
Murley GS, Menz HB, Landorf KB. Foot posture influences the electromyographic activity of selected lower limb muscles during gait. J Foot Ankle Res. 2009;2:35. https://doi.org/10.1186/1757-1146-2-35.
Sanchis-Sales E, Sancho-Bru JL, Roda-Sales A, Pascual-Huerta J. Effect of static foot posture on the dynamic stiffness of foot joints during walking. Gait Posture. 2018;62:241–6.
Behling AV, Nigg BM. Relationships between the foot posture Index and static as well as dynamic rear foot and arch variables. J Biomech. 2020. https://doi.org/10.1016/j.jbiomech.2019.109448;98:109448;98:109448.
Nester CJ, Hutchins S, Bowker P. Shank rotation: a measure of rearfoot motion during normal walking. Foot Ankle Int. 2000;21:578–83. https://doi.org/10.1177/107110070002100709.
Acknowledgements
We want to thank Associate Professor Yohei Okada for their assistance with statistical analysis and interpretation. We would like to thank Editage (www.editage.jp) for English language editing.
Funding
This study was supported by JSPS KAKENHI (Grant number, 19K11403; http://www.jsps.go.jp/j-grantsinaid/index.html).
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted. The specific contributions in this article of the authors are as following: (1) Conception and design of the study: TK, DU, SO, SK, TF, and HI. (2) Collection and assembly of data: TK, DU, TF, YI, TF. (3) Analysis and interpretation of the data: TK, DU, SO, SK, TF, TF, YI and YT. (4) Drafting of the article: TK, DU, SO, SK, TF, TF, YI, YT, and HI. (5) Critical revision of the article for important intellectual content: TK, DU, SO, SK, TF, and HI. (6) Final approval of the article: TK, DU, SO, SK, TF, TF, YI, YT, and HI. (7) Statistical expertise: TK, DU, SO, YT. (8) Obtaining financial support: DU, SO.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the institutional review boards of Kashiba Asahigaoka Hospital (201911001) and Kio University (H30-42). All participants provided written informed consent. This study was performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kubo, T., Uritani, D., Ogaya, S. et al. Association between foot posture and tibiofemoral contact forces during barefoot walking in patients with knee osteoarthritis. BMC Musculoskelet Disord 23, 660 (2022). https://doi.org/10.1186/s12891-022-05624-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05624-y