
Abstract
Purpose/Aim
To investigate the relationship between brachial-ankle pulse wave velocity (baPWV) and microvascular complications in type 2 diabetes mellitus (T2DM).
Materials and methods
From 2019 to 2021, our hospital enrolled 322 patients with T2DM. Clinical information and biochemical indicators of patients were collected from the inpatient electronic medical record system and analyzed retrospectively. Fundus photography, nerve conduction testing, and sensory threshold measurement were all conducted on the subjects. We measured the pulse wave velocity on both sides of the arm and ankle, then averaged the results. The enrolled cases were divided into two groups based on the baPWV: Group 1 (<the reference cutoff value, n = 160) and Group 2 (≥ the reference cutoff value, n = 162). The association between associated factors and baPWV abnormalities was investigated using a logistic regression model.
Results
Group 2 had higher Systolic Blood Pressure(SBP), Diastolic Blood Pressure (DBP), duration of diabetes, Fasting Plasma Glucose (FPG), Blood Urea Nitrogen (BUN) and Serum Uric Acid (SUA) than group 1 (all p < 0.05). The prevalence of diabetic retinopathy, peripheral neuropathy and nephropathy in group 2 was higher compared to group 1 (p < 0.05). After classifying subjects according to the presence or absence of diabetic complications, we found that the baPWV of the Diabetic Peripheral Neuropathy (DPN) group and Diabetic Nephropathy (DN) group was noticeably higher than that of non-DPN group and non-DN group, respectively (both p < 0.05). The baPWV increased with the aggravation of Diabetic Retinopathy (DR) (p < 0.05). Multivariate logistic regression analysis showed that DBP (OR 1.039, 95%CI 1.010–1.068 p = 0.008), duration of diabetes (OR 1.059, 95%CI 1.017–1.103 p = 0.006), FPG (OR 1.104, 95%CI 1.025–1.188 p = 0.009) and BUN (OR 1.128, 95%CI 1.001–1.270 p = 0.048) were all independently and positively associated with baPWV.
Conclusions
The baPWV is strongly associated with microvascular complications of T2DM. The DBP, duration of diabetes, FPG, and BUN were all independent associated factors of baPWV.
Similar content being viewed by others


Introduction
Diabetes has become a major global public health concern, with Type 2 Diabetes Mellitus (T2DM) accounting for about 90% of all diabetes [1]. The T2DM is dangerous because its complications endanger the health and life of patients, with Cardiovascular Disease (CVD), Diabetic Nephropathy (DN), diabetic eye disease, and other vascular complications being the leading causes of death and disability of patients [2]. Pulse Wave Velocity (PWV) is a simple, non-invasive and repeatable method for measuring arterial stiffness [3], with brachial-ankle PWV (baPWV) being the most commonly used [4].
The baPWV was found to be a convenient and reliable early indicator for evaluating arterial stiffness, with important clinical significance for predicting cardiovascular and cerebrovascular risk and prognosis in diabetic patients [5]. The higher the PWV, the more severe the arteriosclerosis and the greater the risk of cardiovascular disease. The PWV was also found to be significantly associated with lacunar cerebral infarction [6] and ischemic stroke [7]. Extensive studies have confirmed the relationship between baPWV and macrovascular in T2DM. However, the correlation between baPWV and microvascular complications is rarely discussed. Hence, the objective of the study was to investigate the association between baPWV and microvascular complications in T2DM (Diabetic Peripheral Neuropathy (DPN), Diabetic Nephropathy (DN), Diabetic Retinopathy (DR)) and its risk factors.
Methods
Subjects
Between 2019 and 2021, patients with T2DM were enrolled in our Inpatient Department of Endocrinology and Metabolism at the Third Affiliated Hospital of Nanchang University. The inclusion criteria for the subjects were:(1) Age, from 18 to 75 years; (2) T2DM was diagnosed using the 1999 World Health Organization (WHO) diagnostic criteria; (3) Patients volunteered to participate. Participants’ exclusion criteria were (1) severe liver or kidney dysfunction; (2) acute DM complications; (3 ) bilateral lower extremity edema, severe cardiac dysfunction; (4) malignant tumor or pregnancy; (4) cannot cooperate with the examination. In the end, 322 T2DM patients were enrolled. The reference mean values of baPWV in the Central Asian population were used as cut-off values [8]. Both mean and reference values increased with age and blood pressure category. The enrolled cases were divided into two groups: Group 1 (<the reference cutoff value, n = 160) and Group 2 (≥ the reference cutoff value, n = 162). Subjects whose age and blood pressure were classified according to the criteria in the table were assigned to group 2 if their baPWV was higher than the reference mean value to which they belonged, and to group 1 if they were not.(Table 1).
The collection of data
We obtained basic clinical information from those subjects, such as their name, ages, duration of diabetes, past medical history, and personal history. Furthermore, general vital signs such as blood pressure, weight, and height were routinely measured in patients. The Body Mass Index (BMI) was calculated as weight (kg)/height(m2).
Each subject had 3 ml of peripheral venous blood collected and anticoagulated with EDTA. All blood samples were obtained after 8 h of fasting, then analyzed for Fasting Plasma Glucose (FPG), 2-hour Blood Glucose (2 h-BG), glycosylated Hemoglobin (HbA1c), Fasting C-Peptide (FCP), Total Cholesterol (TC), Triglycerides (TG), High-Density Lipoprotein Cholesterol (HDL-C), Low-Density Lipoprotein Cholesterol (LDL-C), Serum creatinine (Scr), Serum Uric Acid (SUA), Blood Urea Nitrogen (BUN), among others.
Measurement of baPWV
Subjects rested in a quiet room for at least 15 min in a supine position without pillows before baPWV was measured by a professional using an automated atherosclerosis detector (BP-203RPCE, OMRON, Japan). The subject’s hands were placed at the sides of the body, with both upper arms and ankles cuffed. An electrocardiogram sensor was placed in the precordial region, after which the device automatically recorded and analyzed the data. The mean value of baPWV measured on either side of each patient was used for analysis.
Examination and diagnosis of microvascular complications of T2DM
We used the appropriate methods to diagnose DR, DPN and DN.
According to the International Clinical Grading Criteria for DR, professionals classified patients’ fundus photographic findings as mild, moderate, severe non-proliferate and proliferate [9].
Diagnosis of DPN is made according to the diagnostic basis and diagnostic stratification [10]. Subject history, sensory testing (ankle reflex, temperature sensation, pinprick sensation, pressure sensation), and nerve conduction measurements with the electromyography/evoked potential detection system instrument(CADWELL LABORATORIES, INC), are all part of the DPN examination.
The urinary microprotein and creatinine levels in subjects’ fasting morning urine were determined using dry chemistry, then the urine microprotein to creatinine ratio was calculated. These biochemical indicators are used to identify and classify DN [10]. Moreover, other causes of chronic kidney disease were excluded.
Statistical analysis
Subjects were divided into two groups based on their baPWV (One group was above the reference cutoff value and the other was below it). Continuous variables have a normal or nearly normal distribution, which is expressed as mean ± standard deviation. For continuous variables, the difference between the two groups was tested using unpaired Student’s test, while X²test was used for categorical variables. Additionally, participants were divided into two groups each time based on the presence of DR, DN or DPN. The two groups were compared by unpaired Student’s test, while one-way ANOVA was used for multiple group measurement data. After entering statistically significant variables data from the t-test into multivariate linear regression analysis, independent risk factors were screened. The Statistical Package for the Social Sciences version 25 (SPSS 25.0) was used for all statistical analyses at p < 0.05 or p < 0.01.
Result
Basic data
A total of 322 T2DM patients were enrolled, with approximately 60% being male(n = 192) and 40% female(n = 130), the mean age was 56.70 ± 12.45 years and the mean baPWV was 15.80 ± 3.24 m/s. After dividing the two groups based on the reference cut-off values, the mean baPWV was 14.21 ± 2.31 m/s in group 1(n = 160) and 17.45 ± 3.18 m/s in group 2(n = 162). There were no statistically significant difference between the two groups (P > 0.05) regarding age, sex, smoking, BMI, and alcohol use.There were statistically significant differences between the two groups(P<0.05) in anthropometric indices such as FPG, BUN, SUA, systolic blood pressure and diastolic blood pressure (SBP, DBP) (Table 2).
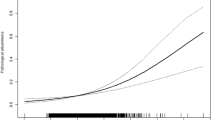
The prevalence of DR, DPN and DN in group 2 were 53.7%, 49.4%, and 47.5%, respectively, which were higher than 41.8%, 35.6%, and 33.8% in group 1. The differences were statistically significant (Table 2; Fig. 1).

Comparison of the prevalence of the three complications. Legend: Group1(below the reference cutoff value), Group2(above the reference cutoff value). * P < 0.05
Relationship between baPWV and type 2 diabetic microangiopathy
Each time, the subjects were grouped based on the presence of DR, DN, or DPN, then the differences in baPWV between the groups were compared. The baPWV was significantly higher in the DPN than in the no DPN group, with the difference being statistically significant (P = 0.003<0.05) (Table 3a). When grouped by the presence or absence of DN, there was a significant increase in baPWV in the group with DN compared to no DN (P = 0.000 < 0.001) (Table 3a). Grouping of subjects according to the stage of DR showed that baPWV in the severe non-proliferative phase group was significantly higher than that in the moderate non-proliferative phase group, baPWV in the moderate non-proliferative phase group was significantly higher than that in the mild non-proliferative phase group, and baPWV in the mild non-proliferative phase group was significantly higher than that in the no DR group (P = 0.000 < 0.001). The DR severity increased with the baPWV (Table 3b).
Multivariate logistic regression analysis of baPWV and related indexes
Multivariate logistic regression analysis was performed with SBP, DBP, duration of diabetes, FPG, BUN and SUA as independent variables, baPWV (group 1 and group 2) as dependent variables, and group 1 as the reference group. The results showed that DBP{OR = 1.039(1.010–1.068) P = 0.008}, duration of diabetes {OR = 1.059 (1.017–1.103) P = 0.006}, FPG{OR = 1.104 (1.025–1.188) P = 0.009}, and BUN{OR = 1.128(1.001–1.270) P = 0.048}were all independently associated with baPWV (Table 4).
Discussion
In this study we found that a measure of diabetic macrovascular disease - baPWV - was associated with measures of diabetic microvascular disease - eye, kidney, nerve - on cross sectional analysis. These results suggest that the same factors that are associated with macrovascular disease are associated with microvascular disease.
Traditionally, the complications of chronic diabetes mellitus have been primarily considered attributed to vascular injury. However, many researchers have investigated the relationship between arterial stiffness and the occurrence and development of T2DM. BaPWV is a measure of arterial elasticity [11], so we reviewed a large number of articles to analyze the relationship between bapwv and T2DM. In recent years, international studies have found that baPWV is inextricably linked to the development of T2DM as well as the chronic complications that result from it. After adjusting for related influencing factors, baPWV, smoking, and a high LDL-C level were found to be associated with microalbuminuria in T2DM patients [12], implying a possible link between the pathogenesis of atherosclerosis and DN. Arteriosclerosis is a major contributor to the progression of chronic kidney disease [13]. Therefore, some researchers have proposed baPWV as a potential early detection method for DN [14]. Moreover, Siasos et al. found that aortic stiffness determined by carotid-femoral PWV(cfPWV) was significantly associated with DPN [15] in a cross-sectional study. Furthermore, cfPWV is an index of atherosclerosis that is associated with cardiovascular disease risk factors and clinical events to a similar degree as baPWV [16]. After adjustment for several traditional risk factors for DPN development including HbA1c, duration of diabetes, arterial hypertension, dyslipidemia, height, and other microvascular complications like retinopathy and nephropathy, this association remained significant. Concerning DR, An et al. investigated the relationship between atherosclerosis and the progression of DR and concluded that baseline baPWV may be an independent predictor of new onset/progression of DR [17]. According to Liu et al., high PWV (> 19.6 m/s) was strongly associated with the risk of severe DR, particularly PDR [18]. The severity of DR was positively correlated with increasing degree of PWV, generally consistent with the findings of this study.
Moreover, Yiming et al. measured baPWV in a Chinese Xinjiang population of varying age and blood type, the first study of baPWV in a Chinese population [8]. Therefore, the baPWV grouping in this study refers to the reference mean value as the Cut-off value. Subjects were grouped based on whether they had microvascular complications from T2DM. The results also revealed that the baPWV was significantly higher in the affected group, implying that baPWV was associated with microangiopathy in T2DM. These findings are consistent with those of several other researchers.
We investigated the factors that influence baPWV, and discovered that SBP, DBP, duration of diabetes, duration of hypertension, FPG, BUN, and SUA were all positively correlated with baPWV, consistent with the findings of many other researchers. Age and blood pressure are important factors influencing baPWV [19]. Sougawa et al. concluded that the main factors associated with baPWV in both men and women were age, BMI, and blood pressure [20]. Kim found that baPWV increased with age, disease duration, SBP as well as the prevalence of diabetic microvascular complications (DR and DN)[21]. On the contrary, during the baPWV grouping, our study adjusted for two factors, age and blood pressure, increasing the comparability between the two groups.
This study has some limitations and deficiencies. First, because our study was a cross-sectional study, we were unable to judge causality longitudinally. We were also not able to determine the sequence of effects of baPWV, blood pressure, and blood glucose. Second, when collecting clinical data, we did not record a complete medication situation of patients, and hence the statistical results may have been influenced by antihypertensive drugs, hypoglycemic drugs and lipid-lowering drugs.
In conclusion, the baPWV measurement is known to be simple and reliable for determining arterial stiffness [22]. Our findings are consistent with previous studies, implying that baPWV may be a simple and effective indicator to assist in the diagnosis of microvascular diseases in early T2DM.
Data Availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- T2DM:
-
type 2 diabetes mellitus
- baPWV:
-
brachial-ankle pulse wave velocity
- SBP:
-
Systolic Blood Pressure
- DBP:
-
Diastolic Blood Pressure
- FPG:
-
Fasting Plasma Glucose
- BUN:
-
Blood Urea Nitrogen
- SUA:
-
Serum Uric Acid
- DPN:
-
Diabetic Peripheral Neuropathy
- DN:
-
Diabetic Nephropathy
- DR:
-
Diabetic Retinopathy
- CVD:
-
Cardiovascular Disease
- PWV:
-
Pulse Wave Velocity
- WHO:
-
World Health Organization
- BMI:
-
Body Mass Index
- 2h-BG:
-
2-hour Blood Glucose
- HbA1c:
-
glycosylated Hemoglobin
- FCP:
-
Fasting C-Peptide
- 2h-CP:
-
2-hour C-peptide
- TC:
-
Total Cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-Density Lipoprotein Cholesterol
- LDL-C:
-
Low-Density Lipoprotein Cholesterol
- Scr:
-
Serum creatinine
- NPDR:
-
nonproliferative diabetic retinopathy
- PDR:
-
proliferative diabetic retinopathy
References
Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, Colagiuri S, Guariguata L, Motala AA, Ogurtsova K et al: Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract 2019, 157:107843.
Mauricio D, Alonso N, Gratacòs M: Chronic diabetes complications: the need to move beyond classical concepts. Trends Endocrinol Metab 2020, 31(4):287–295.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H: Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006, 27(21):2588–2605.
Obeid H, Soulat G, Mousseaux E, Laurent S, Stergiopulos N, Boutouyrie P, Segers P: Numerical assessment and comparison of pulse wave velocity methods aiming at measuring aortic stiffness. Physiol Meas 2017, 38(11):1953–1967.
Tomiyama H: Arterial stiffness: is this a marker for the current status or future? J Atheroscler Thromb 2016, 23(9):1026–1027.
Li T, Wu XJ, Chen XM, Wang SB, Liu KD, Xing YQ: Ankle-brachial index and brachial-ankle pulse wave velocity are risk factors for ischemic stroke in patients with type 2 diabetes. Neural Regen Res 2017, 12(11):1853–1859.
Shan Y, Lin J, Xu P, Zeng M, Lin H, Yan H: Association of Aortic Compliance and Brachial Endothelial Function with Cerebral Small Vessel Disease in Type 2 Diabetes Mellitus Patients: Assessment with High-Resolution MRI. Biomed Res Int 2016, 2016:1609317.
Yiming G, Zhou X, Lv W, Peng Y, Zhang W, Cheng X, Li Y, Xing Q, Zhang J, Zhou Q et al: Reference values of brachial-ankle pulse wave velocity according to age and blood pressure in a central Asia population. PLoS One 2017, 12(4):e0171737.
Flaxel C, Adelman R, Bailey S, Fawzi A, Lim J, Vemulakonda G, Ying G: Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology 2020, 127(1):P66-P145.
Jia W, Weng J, Zhu D, Ji L, Lu J, Zhou Z, Zou D, Guo L, Ji Q, Chen L et al: Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev 2019, 35(6):e3158.
Lu YC, Lyu P, Zhu HY, Xu DX, Tahir S, Zhang HF, Zhou F, Yao WM, Gong L, Zhou YL et al: Brachial-ankle pulse wave velocity compared with mean arterial pressure and pulse pressure in risk stratification in a chinese population. J Hypertens 2018, 36(3):528–536.
Kim BK, Acharya D, Nah DY, Rhee MY, Yoo SJ, Lee K: Association between Brachial-Ankle pulse Wave Velocity and Microalbuminuria and to predict the risk for the development of Microalbuminuria using brachial-ankle pulse Wave Velocity Measurement in type 2 diabetes Mellitus Patients. Healthcare (Basel) 2019, 7(4).
Townsend RR, Anderson AH, Chirinos JA, Feldman HI, Grunwald JE, Nessel L, Roy J, Weir MR, Wright JT, Jr., Bansal N et al: Association of Pulse Wave Velocity with chronic kidney Disease Progression and Mortality: findings from the CRIC Study (chronic renal insufficiency cohort). Hypertension 2018, 71(6):1101–1107.
Zhang X, Bai R, Zou L, Zong J, Qin Y, Wang Y: Brachial-Ankle Pulse Wave Velocity as a Novel Modality for Detecting Early Diabetic Nephropathy in Type 2 Diabetes Patients. J Diabetes Res 2021, 2021:8862573.
Tentolouris A, Eleftheriadou I, Grigoropoulou P, Kokkinos A, Siasos G, Ntanasis-Stathopoulos I, Tentolouris N: The association between pulse wave velocity and peripheral neuropathy in patients with type 2 diabetes mellitus. J Diabetes Complications 2017, 31(11):1624–1629.
Tanaka H, Munakata M, Kawano Y, Ohishi M, Shoji T, Sugawara J, Tomiyama H, Yamashina A, Yasuda H, Sawayama T et al: Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness. J Hypertens 2009, 27(10):2022–2027.
An Y, Yang Y, Cao B, Dong H, Li A, Zhao W, Ke J, Zhao D: Increased Arterial Stiffness as a Predictor for Onset and Progression of Diabetic Retinopathy in Type 2 Diabetes Mellitus. J Diabetes Res 2021, 2021:9124656.
Liu SC, Chuang SM, Shih HM, Wang CH, Tsai MC, Lee CC: High pulse wave velocity is associated with the severity of diabetic retinopathy in patients with type 2 diabetes. J Investig Med 2020, 68(6):1159–1165.
Ohkuma T, Ninomiya T, Tomiyama H, Kario K, Hoshide S, Kita Y, Inoguchi T, Maeda Y, Kohara K, Tabara Y et al: Brachial-ankle pulse Wave Velocity and the risk prediction of Cardiovascular Disease: an individual Participant Data Meta-Analysis. Hypertension 2017, 69(6):1045–1052.
Sougawa Y, Miyai N, Utsumi M, Miyashita K, Takeda S, Arita M: Brachial-ankle pulse wave velocity in healthy japanese adolescents: reference values for the assessment of arterial stiffness and cardiovascular risk profiles. Hypertens Res 2020, 43(4):331–341.
Kim JM, Kim SS, Kim IJ, Kim JH, Kim BH, Kim MK, Lee SH, Lee CW, Kim MC, Ahn JH et al: Arterial stiffness is an independent predictor for risk of mortality in patients with type 2 diabetes mellitus: the REBOUND study. Cardiovasc Diabetol 2020, 19(1):143.
He D, Gao L, Yang Y, Jia J, Jiang Y, Sun P, Liu B, Li J, Fan F, Zhang Y et al: Brachial-ankle pulse wave velocity as a measurement for increased carotid intima-media thickness: a comparison with carotid-femoral pulse wave velocity in a chinese community-based cohort. Journal of clinical hypertension (Greenwich, Conn) 2022, 24(4):409–417.
Acknowledgements
The authors are grateful to the researchers and participants who helped throughout the study.
Funding
The study was funded by Science and Technology Program of Jiangxi Provincial Health and Health Commission(202311215, 20187003).
Author information
Authors and Affiliations
Contributions
YP drafted the manuscript. BD designed the study and revised the manuscript. YS, YL performed the statistical analysis and assisted with data acquisition. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of Third Affiliated Hospital of Nanchang University. Written informed consent of the subject and oral informed consent of the illiterate subject approved by the Ethics Committee of the Third Affiliated Hospital of Nanchang University were obtained after the study was explained to the subject in detail. All experiments and methods were carried out in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pei, Y., Shu, Y., Deng, B. et al. Association between brachial-ankle pulse wave velocity and microvascular complications in type 2 diabetes mellitus. BMC Endocr Disord 23, 98 (2023). https://doi.org/10.1186/s12902-023-01355-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01355-w