
Abstract
Background
Although periodontitis has previously been reported to be linked with multiple sclerosis (MS), but the molecular mechanisms and pathological interactions between the two remain unclear. This study aims to explore potential crosstalk genes and pathways between periodontitis and MS.
Methods
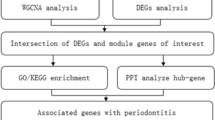
Periodontitis and MS data were obtained from the Gene Expression Omnibus (GEO) database. Shared genes were identified by differential expression analysis and weighted gene co-expression network analysis (WGCNA). Then, enrichment analysis for the shared genes was carried out by multiple methods. The least absolute shrinkage and selection operator (LASSO) regression was used to obtain potential shared diagnostic genes. Furthermore, the expression profile of 28 immune cells in periodontitis and MS was examined using single-sample GSEA (ssGSEA). Finally, real-time quantitative fluorescent PCR (qRT-PCR) and immune histochemical staining were employed to validate Hub gene expressions in periodontitis and MS samples.
Results
FAM46C, SLC7A7, LY96, CFI, DDIT4L, CD14, C5AR1, and IGJ genes were the shared genes between periodontitis, and MS. GO analysis revealed that the shared genes exhibited the greatest enrichment in response to molecules of bacterial origin. LASSO analysis indicated that CFI, DDIT4L, and FAM46C were the most effective shared diagnostic biomarkers for periodontitis and MS, which were further validated by qPCR and immunohistochemical staining. ssGSEA analysis revealed that T and B cells significantly influence the development of MS and periodontitis.
Conclusions
FAM46C, SLC7A7, LY96, CFI, DDIT4L, CD14, C5AR1, and IGJ were the most important crosstalk genes between periodontitis, and MS. Further studies found that CFI, DDIT4L, and FAM46C were potential biomarkers in periodontitis and MS.
Similar content being viewed by others

Introduction
Periodontitis is a common chronic infectious and inflammatory disease affecting people worldwide. Its etiology mainly includes the direct damage of the periodontal tissues by bacteria and the immune disorder of the host caused by bacteria [1]. Periodontitis is distinguished by enduring inflammation of the tissues that support the teeth, destruction of the periodontal ligaments, and progressive loss of alveolar bone around the teeth [2]. Recently, it has been shown that periodontitis can lead to several systemic illnesses. This may be due to the pro-inflammatory cytokines or bacteria in the mouth through the blood or triggering the body’s immune response and other related mechanisms [3].
Multiple sclerosis (MS) is an autoimmune disease that causes inflammatory demyelinating lesions of white matter in the central nervous system [4]. Even though the cause of MS is unclear, current findings suggest that environmental and genetic variables contribute to the disease’s development [5]. Several environmental factors, such as infection, latitude, vitamin D deficiency, and smoking, contribute to the development of MS [6]. Research has shown that bacterial infection may be a crucial factor in the etiology of MS. They were found to be pathogenic environmental factors in the pathogenesis of MS [13]. In addition, some pathogenic or symbiotic bacteria can mediate MS by activating Th17 cells to produce inflammatory factors. Studies have shown that Porphyromonas gingivalis (P. gingivalis) is significantly elevated in patients with MS, and P. gingivalis is also one of the main causative agents of periodontitis [7]. Also, people with periodontitis are more susceptible to MS, and periodontal infections may worsen MS symptoms [8]. These findings suggest that there could be links between periodontitis and MS. However, the molecular mechanisms and pathological interactions between the two remain unclear.
As microarray and high-throughput sequencing technologies continue to advance quickly, bioinformatics techniques are frequently used to investigate the crosstalk between diseases in order to reveal the connections between the cellular and molecular mechanisms of diseases. In this study, we explored potential crosstalk genes between periodontitis and MS through bioinformatics methods. We analyzed the interactions between these genes and immune cells to acquire a greater comprehension of potential mechanisms of interaction between periodontitis and MS. Additionally, three candidate biomarkers for periodontitis and MS were identified by using bioinformatics tools, which were further validated by qPCR and immunohistochemical staining techniques, suggesting that they may be biomarkers for predicting the occurrence of periodontitis and MS.
Materials and methods
Data download
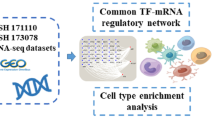
Gene expression data for periodontitis and MS were downloaded from the Gene Expression Omnibus (GEO) database (https://www.ncbi.nlm.nih.gov/geo/). In the periodontitis dataset, GSE16134 (based on the GPL570 platform) was used as a test cohort with 310 gingival papillae (241 “diseased” and 69 “healthy”), and GSE1334 as a validation cohort with 247 gingival papillae with 183 “diseased” and 64 “healthy.” The MS dataset contains GSE108000 (based on the GPL13497 platform) and GSE135511 (based on the GPL6883 platform), and we combined GSE108000 and GSE135511 into a new dataset by using the “SVA” R package to remove batches. The combined dataset includes 20 healthy controls and 70 MS samples. In addition, to assess the effectiveness of the diagnostic process, we downloaded the GSE38010 dataset (based on the GPL570 platform), which contains 2 healthy controls and 5 MS samples.
Identification of DEGs
To normalize the datasets, R (4.2.3) software was used. Afterward, we identified differentially expressed genes (DEGs) from the GSE16134 and a combined dataset of the GSE108000 and GSE135511 by using the R package “limma” with adjusted P values < 0.05 and |log FC|≥0.8.
WGCNA network construction and module identification
The co-expression network of periodontitis (GSE16134) and MS (a merged dataset of GSE108000 and GSE135511) was constructed using the WGCNA package in R. The network is ensured to be a scale-free network by using a soft threshold, which is advantageous for subsequent network generation. Gene modules were identified using hierarchical clustering trees, while gene modules with strong connections were constructed using hierarchical clustering based on topological overlap matrix (TOM). Pearson’s correlation coefficient was calculated to analyze relationships between the various modules and diseases. The module showing the highest correlation with the disease was selected, and the genes within this module were obtained.
Identification of shared genes and pathway enrichment
By drawing Venn diagrams, the shared genes identified by WGCNA and DEG were obtained. Then, we explored functions and pathways associated with these genes through Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) using “clusterProfiler” and “org.Hs.eg.db” packages [9,10,11,12].
Feature selection by the least absolute shrinkage and selection operator
To discover hub genes with the best diagnostic efficacy among the shared genes identified above between periodontitis and MS, we utilized the “glmnet” package in R to conduct the least absolute shrinkage and selection operator (LASSO) regression.
Candidate biomarker expression levels and diagnostic value
We utilized the “ggplot2” package in R software to test expression levels of the hub genes in periodontitis and MS samples. To assess the diagnostic efficacy of potential biomarkers on periodontitis (GSE16134) and MS (a merged dataset of GSE108000 and GSE135511) datasets, we used receiver operating characteristic curves (ROCs) using the “pROC” package in R. Furthermore, we verify the diagnostic efficiency of potential biomarkers using two external datasets including GSE10334 and GSE38010.
ssGSEA
We analyzed the infiltration of immune cells in diseased and healthy samples through ssGSEA using the “GSVA” R package. Then, we explored links between potential biomarkers and infiltrating immune cells through the Spearman method.
Gingival biopsy and peripheral blood collection
10 human gingival tissues, including 5 cases and 5 controls, were obtained from healthy volunteers and patients with periodontitis. In addition, our study also included individuals with 5 MS samples and 10 healthy volunteers, and we obtained peripheral blood from multiple sclerosis patients and healthy people, respectively, for the extraction of peripheral blood mononuclear cells (PBMCs). Inclusion criteria included patients diagnosed and treated for the first time, patients with complete medical records, and patients without systemic disorders. All studies were approved by the Ethics Committee of the Affiliated Stomatology Hospital of Anhui Medical University and the First Affiliated Hospital of Anhui Medical University.
RNA collection and qRT-PCR
A Ficoll (Histopaque; Sigma–Aldrich, Zwijndrecht, The Netherlands) density gradient was used to extract PBMCs through centrifugation. RNA from gingival tissue and PBMCs was extracted using TRIzol reagent (Invitrogen). cDNAs was synthesized from 2 µg total RNA according to instructions of cDNA Reverse Transcription Kit (Takara, Tokyo, Japan). Subsequently, qRT-PCR was performed using the Stratagene Mx3000P system (Agilent Technologies, USA) and SYBR Green Master Mix (11,701, Accurate Biology). GAPDH was used to normalize the gene’s expression levels, and the comparative Ct method with Formula 2−ΔCt was used to compute the expression value. All experiments were repeated more than three times. Supplementary Table S1 contains a list of primers.
Immunohistochemical staining of gingival tissue
The collected gingival tissues were preserved using 4% paraformaldehyde and then embedded in paraffin. The paraffin-embedded tissue was sliced into serial Sect. 4 micrometers thick and then deparaffinized for antigen extraction. Subsequently, these slides were treated with goat serum and then incubated with antibodies. After that, 3,3’-diaminobenzidine tetrahydrochloride (DAB) and hematoxylin were used to stain the sections. Microscope images were captured and processed using image-processing software (ImageJ v 1.48).
Statistical analysis
We utilized GraphPad Prism 8.0 for both conducting statistical analysis and creating visual representations. All results are expressed as mean ± standard deviation. The method chosen for statistical analysis was the unpaired t-test (P < 0.05).
Results
Identification of DEGs
In GSE16134, a total of 315 DEGs with 217 upregulated and 98 downregulated, were found, while the combined dataset of GSE108000 and GSE135511 showed 227 DEGs, 150 of which were upregulated and 77 downregulated. The top 100 DEGs of these two diseases were shown in heatmaps (Fig. 1a, b), and expression patterns of the DEGs in these diseases were displayed in volcano maps (Fig. 1c, d). Ten genes (FAM46C, COL4A1, SLC7A7, LY96, CFI, DDIT4L, CD14, C5AR1, IGJ, NEFL) differently expressed in both MS and periodontitis were revealed by combining the upregulated and downregulated genes (Fig. 1e).

identification of genes with variable expression. The periodontitis database GSE16134’s top 100 DEGs are depicted in a heatmap in Figure (a). (b) In a combined dataset of GSE108000 and GSE135511 in MS, a heatmap of the top 100 DEGs. (c) A DEG volcano graphic from the GSE16134 periodontitis database. (d) A volcano plot of DEGs in the MS dataset created by merging GSE108000 and GSE135511. (e) A Venn diagram showing an overlap of 10 DEGs between periodontitis and MS. Control is a negative; MS is multiple sclerosis. Differentially expressed genes, or DEGs
WGCNA network construction and module identification
By clustering samples to check the outliers, neither GSE16134 nor a combined dataset of GSE108000 and GSE135511 deleted the samples (Fig. 2a, b). To ensure the creation of a scale-free network, a power of β = 12 was used for GSE16134, while the β value was 3 for the combined GSE108000 and GSE135511 datasets. The co-expression network generated by periodontitis samples consisted of 7 modules, whereas the network constructed using MS samples contained 9 modules (Fig. 2c, d). The Pearson correlation coefficient was applied to calculate the associations of modules with disease. In GSE16134, the turquoise module had the largest positive correlation with periodontitis (r = 0.67), while the blue module showed the most significant negative correlation (r = -0.41). In a combined dataset of GSE108000 and GSE135511, the blue module had the largest positive association for MS (r = 0.51), whereas the pink module had the most significant negative correlation (r = -0.45). There were 151 overlapping genes obtained by intersecting genes in the most obvious positive correlation and negative correlation modules (Fig. 2e).

Analysis of coexpression for genes with differential expression. (a) Sample dendrogram and trait heatmap in the periodontitis database GSE16134. (b) Sample dendrogram and trait heatmap in a merged dataset of GSE108000 and GSE135511 in MS. (c) Heatmap of the module-trait relationships in the periodontitis database GSE16134. (d) Heatmap of the module-trait connections in the combined GSE108000 and GSE135511 dataset in MS. (e) Venn diagram shows that 151 genes overlap in MS and periodontitis modules. MS: Multiple sclerosis
Identification of shared genes and pathway enrichment
Venn diagrams revealed that there were eight shared genes (FAM46C, SLC7A7, LY96, CFI, DDIT4L, CD14, C5AR1, and IGJ) that overlapped between periodontitis and MS which were screened by WGCNA and DEGs (Fig. 3a). The GO analysis indicated that these shared genes were most significantly associated with response to molecule of bacterial origin, positive regulation of response to external stimulus, and positive regulation of cytokine production (Fig. 3b). According to the KEGG analysis, these genes were primarily enriched in alcoholic liver disease (ALD), pertussis, complement and coagulation cascades, staphylococcus aureus infection, NF-κB signaling pathway, Toll-like receptor signaling pathway, lipid and atherosclerosis, and salmonella infection (Fig. 3c).

Identification of the shared genes and their KEGG pathway analysis and GO functional enrichment analysis. (a) Venn diagram showing that 8 genes were elected from the union set between DEGs and trait-module key genes in WGCNA. (b) GO analysis of the shared genes. (c) KEGG pathway enrichment analysis of the shared genes. DEG: differentially expressed gene; WGCNA: weighted gene co-expression network analysis
Identification of potential shared diagnostic genes by least absolute shrinkage and selection operator
A LASSO regression method was utilized to identify the diagnostic gene common to both disorders. Four core cross-genes were found in the periodontitis dataset GSE16134 (Fig. 4a, b), and four core cross-genes were found in the MS dataset merged in GSE108000 and GSE135511 (Fig. 4c, d). Three overlapping genes (FAM46C, CFI, and DDIT4L) were identified as the most effective diagnostic biomarkers for both periodontitis and MS by using a Venn diagram (Fig. 4e).

Identification of potential shared diagnostic genes by the LASSO regression model. (a) Tenfold cross-validation to select the optimal tuning parameter log (lambda) in the the periodontitis database GSE16134 database. (b) LASSO coefficient profiles of diagnostic genes in the the periodontitis database GSE16134 database. (c) Tenfold cross-validation to select the optimal tuning parameter log (lambda) in a merged dataset of GSE108000 and GSE135511 in MS. (d) LASSO coefficient profiles of diagnostic genes in a merged dataset of GSE108000 and GSE135511 in MS. (e) Venn diagram showing the optimal diagnostic biomarkers
Candidate biomarker expression levels and diagnostic value
Further studies found that three candidate biomarkers (FAM46C, CFI, and DDIT4L) expression levels were all upregulated in both periodontitis and MS samples (Fig. 5a, b). ROC curves were employed to evaluate the diagnostic efficacy of these potential biomarkers. In GSE16134 (Fig. 5c), the diagnostic value of these three biomarkers was high: FAM46C (AUC = 0.896), CFI (AUC = 0.830), and DDIT4L (AUC = 0.795). In a dataset merged from GSE108000 and GSE135511 (Fig. 5d), CFI (AUC = 0.775) and DDIT4L (AUC = 0.820) exhibited greater diagnostic utility for MS, while FAM46C demonstrated an almost flawless diagnostic value (AUC = 0.946). Then, two external datasets (GSE10034 and GSE38010) were further used to verify the prediction accuracy of CFI, DDIT4L, and FAM46C. All three showed strong predictive performance (Supplementary Fig. S1).

Expression pattern validation and diagnostic value. (a) Expression of CFI, DDIT4L and FAM46C in the periodontitis database GSE16134. (b) Expression of CFI, DDIT4L and FAM46C in a merged dataset of GSE108000 and GSE135511 in MS. (c) ROC curve of the shared diagnostic genes in the periodontitis database GSE16134. (d) ROC curve of the shared diagnostic genes in a merged dataset of GSE108000 and GSE135511 in MS. Con: control; MS: Multiple sclerosis. *P < 0.05; **P < 0.01; ***P < 0.001
Immune infiltration analysis
Furthermore, we explored the infiltration of immune cells in different samples. Both results of heatmaps (Fig. 6a, b) and violin plots (Fig. 6c, d) showed significant changes in a variety of immune cells in the periodontitis dataset GSE16134 and the MS dataset merged by GSE108000 and GSE135511, especially T cells and B cells. Additionally, analysis of the correlation between immune cells and candidate biomarkers revealed a positive association between regulatory T cells, natural killer cells, mast cells, immature dendritic cells and gamma delta T cells with CFI in both periodontitis samples and MS samples. In MS and periodontitis samples, there was a positive correlation between immature dendritic cells and DDIT4L. In samples with periodontitis and MS, type 1 T helper cells, T follicular helper cells, regulatory T cells plasmacytoid dendritic cells, natural killer T cells, natural killer cells, MDSCs, mast cells, macrophage, immature B cells, gamma delta T cells, activated B cells, activated dendritic cells, activated CD4 T cells and activated CD8 T cells showed a positive correlation with FAM46C (Fig. 6e, f).

Analysis of immune infiltration associated with periodontitis and MS. (a) A heatmap of the distribution of 28 immune cells in normal samples and periodontitis samples. (b) A heatmap of the distribution of 28 immune cells in normal samples and MS samples. (c) A violin plot of the distribution of 28 immune cells in normal samples and periodontitis samples. (d) A violin plot of the distribution of 28 immune cells in normal samples and MS samples. (e) The relationship between diagnostic genes and immune cell infiltration in the periodontitis dataset GSE16134. (f) The relationship between diagnostic genes and immune cell infiltration in the MS dataset merged by GSE108000 and GSE135511. Con, control; MS: Multiple sclerosis
CFI, DDIT4L and F4AM6C were upregulated in patients with periodontitis and MS compared with healthy controls
To further validate the diagnostic values of three candidate markers, qPCR and immunohistochemical staining were used to verify their expressions in periodontitis and MS samples. qRT-PCR results indicated that mRNA levels of the pro-inflammatory cytokines (IL-1, IL-6, and IL-8) (Fig. 7a) and also CFI, DDIT4L, F4AM6C (Fig. 7b) were upregulated in patients with periodontitis compared with healthy controls. Similarly, qRT-PCR results (Fig. 7c) indicated that the mRNA levels of the CFI, DDIT4L, and F4AM6C were upregulated in patients with MS compared with healthy controls. Results of immunohistochemical staining revealed that CFI, DDIT4L, and FAM46C were upregulated in periodontitis samples compared with healthy controls (Fig. 7d).

CFI, DDIT4L and FAM46C was upregulated in patients with periodontitis and MS compared with healthy controls. (a) qRT-PCR results show the mRNA expression of IL-1β, IL-6 and IL-8 in the gingivae of healthy and periodontitis (ncon=5, ncase=5). GAPDH was used for normalization relative to the control group. (b) qRT-PCR results show the mRNA expression of CFI, DDIT4L and FAM46C in the gingivae of healthy and periodontitis (ncon=5, ncase=5). GAPDH was used for normalization relative to the control group. (c) qRT-PCR results show the mRNA expression of CFI, DDIT4L and FAM46C in the peripheral blood of healthy and MS (ncon=10, ncase=5). GAPDH was used for normalization relative to the control group. (d) Immunohistochemistry staining of CFI, DDIT4L and FAM46C in the gingivae of healthy and periodontitis. Con, control; MS: Multiple sclerosis
Discussion
Periodontitis, a chronic inflammatory disease, causes systemic inflammation and contributes to the development of several neurodegenerative diseases, such as MS [8, 13]. However, the mechanisms remain to be revealed. Additionally, the lack of sufficient knowledge regarding the pathogenesis of MS has impeded the progress of treatment options. Through the use of large-scale data, bioinformatics techniques offer a thorough knowledge of numerous illnesses at the molecular level [14, 15]. Moreover, it is also particularly important for identifying potential biomarkers for the diagnosis and prognosis of human diseases [16, 17]. Nevertheless, there were few reports on their utilization for screening potential biomarkers in patients with periodontitis combined with MS.
In this study, we used WGCNA to look into the common pathways by combining the transcriptomes of MS and periodontitis. Meanwhile, we uncovered possible intersecting genes, common pathways, and infiltration of immune cells between periodontitis and MS through multiple methods. Results of our study discovered that the most significant crosstalk genes between periodontitis and MS were FAM46C, SLC7A7, LY96, CFI, DDIT4L, CD14, and IGJ, which may be associated with response to molecules of bacterial origin. Then, it was discovered that CFI, DDIT4L, and FAM46C are useful diagnostic markers for periodontitis and MS. T cells and B cells are essential in developing MS and periodontitis, according to the results of immune infiltration.
The findings of this research imply that the primary genes involved in the cross-talk between MS and periodontitis are linked to a bacterial molecular response. As we all know, periodontitis is an inflammatory disease, and bacteria play an important role in its pathogenesis [18]. Studies have demonstrated that the pathogens of periodontitis include a variety of bacteria, such as Actinomyces aggregator, P. gingivalis, Forsetana, Treponema dentalis, and Clostridium nucleatus. These bacteria can cause gingival cell death and periodontal tissue damage by secreting lipopolysaccharide (LPS) and a variety of toxic substances, producing a variety of inflammatory factors. These cytokines can also spread through the blood, causing a systemic inflammatory response that triggers MS [8]. In addition to being transmitted through the blood, some bacteria can directly stimulate nerve immune cells to activate an inflammatory response. For instance, glial cells, the main immune cells in the nervous system, have been discovered to be stimulated by P. gingivalis and its products lipopolysaccharide to produce pro-inflammatory mediators such as nitric oxide (NO) and prostaglandin E2 (PGE2), leading to demyelination and aggravating MS [19]. These results imply that bacterial factors are critical in developing MS and periodontitis and may account for part of the greater incidence of MS in patients with periodontitis. The KEGG enrichment analysis revealed that these crosstalk genes are involved in ALD, the complement and clotting cascade, NF-κB signaling pathway, and Toll-like receptor signaling pathways. Studies have indicated that P. gingivalis can worsen ALD by changing the composition of intestinal microbiota and the immune response of the host [20]. Moreover, ALD has an increased risk of MS development [21]. Meanwhile, the involvement of complement and coagulation cascade in the mechanisms of periodontitis and MS has been demonstrated [22,23,24]. NF-κB is a signaling pathway that plays a crucial role in regulating immune and inflammatory responses. Activation of NF-κB signaling pathway can enhance osteoclast differentiation and exacerbate periodontitis by increasing the expression of IL-1β and various inflammatory factors [25, 26]. Furthermore, activation of NF-κB signaling pathway can also impact MS by stimulating peripheral immunity and inflammatory responses in the central nervous system [27]. Additionally, Toll-like receptor signaling pathways have also been shown to mediate the development of periodontitis and MS by regulating immune responses [28, 29].
This study explored the potential immunological connection between MS and periodontitis in the preliminary stages. According to our findings, the immunological patterns of the MS and periodontitis groups were considerably different from those of the control group, with the increase in B cells and T cells being particularly noticeable. Multiple infections invading the host and setting off an immune response cause periodontitis. P. gingivalis, the main pathogenic bacterium responsible for periodontitis, has been identified to release a variety of virulence factors, which in turn trigger the production of pro-inflammatory molecules, leading to an increase in the number of local B cells and T cells. Peripherally activated T-cell and B-cell interactions additionally trigger MS. It is generally known that B cells play important roles in the development of MS. For instance, B cells in MS patients may emit not only antibodies but also soluble toxic substances that, by their proliferation, harm oligodendrocytes and neurons [30]. Meanwhile, many B-cell subtypes, including memory B-cells and plasma mother cells, have been observed in the cerebrospinal fluid (CSF) of MS patients, especially memory B-cells and plasma mother cells [31]. More importantly, the success of treating MS by depleting B cells using anti-CD20 antibodies strongly highlights the importance of B cells in MS [30]. Moreover, studies have shown that CD4 T lymphocytes, particularly helper T cells 1 (Th1) and 17 (Th17), can pass the blood-brain barrier in response to myelin antigens, infiltrate the central nervous system, and trigger inflammation. Among them, Th1 and Th17 can aggravate MS by secreting IFN-γ and IL-17 [32]. It’s interesting to note that one study discovered that P. gingivalis infection can boost the impact of T lymphocytes on CNS autoantigens [19]. Therefore, periodontal disease may exacerbate MS by increasing the sensitivity of T and B cells to autoimmune antigens.
To improve the accuracy of testing biomarkers, we choose datasets with large sample sizes as much as possible. In our research, the periodontitis dataset GSE16134 contained 310 samples of gingival tissue, while the MS dataset, which was created by merging GSE108000 and GSE135511, contained 90 samples of brain tissue. The receiver operator curve (AUC) is employed to evaluate the diagnostic efficacy of biomarkers. ROC curve showed that the AUC values of CFI, DDIT4L, and FAM46C in the diagnosis of periodontitis were 0.830, 0.795, and 0.896, while the AUC values in the diagnosis of MS were 0.775, 0.820, and 0.946. These results suggest that CFI, DDIT4L, and FAM46C have a high capacity to predict periodontitis and MS.
Family with sequence similarity 46 member C (FAM46C), a non-standard poly(A) polymerase, was found to be a significant crosstalk gene between periodontitis and MS. Previous evidence has shown that FAM46C can inhibit tumor growth through a variety of pathways [33]. In addition, emerging evidence has shown that FAM46C can regulate immune responses. M1/M2 imbalance is one of the manifestations of periodontitis and MS [34, 35]. Studies have found that FAM46C can promote the polarization of M2 and alleviate the immune response [36]. This may be one of the mechanisms by which FAM46C participates in periodontitis and MS. The results of the ssGSEA study showed that FAM46C was significantly positively associated with macrophages in periodontitis and MS samples, which also jointly emphasized the involvement of FAM46C in these two diseases of pathology through a mediated immune response.
DNA-damage-inducible transcript 4 (DDIT4L) was found to be a gene that regulates autophagy and promotes autophagy by inhibiting the mTOR signaling pathway [37]. As we know, autophagy plays a significant part in innate immunity and has been linked to many inflammatory diseases [38]. In the pathogenesis of periodontitis, autophagy has been discovered to activate and regulate inflammation by promoting or inhibiting cytokines and lead to bone loss by disrupting the balance between osteogenesis and osteolysis [39, 40]. In addition, studies have shown that autophagy has a dual function in MS. On the one hand, myelin antigen presentation by CD4 T cells can be enhanced by enhancing the process of autophagy, thus aggravating MS. On the other hand, defective autophagy leads to abnormal clearance of inflammatory bodies and myelin debris in microglia and promotes pro-inflammatory phenotypes [31]. The above evidence indicates that DDIT4L may play a role in periodontitis-mediated MS by regulating autophagy. However, further experiments are needed to confirm this speculation.
Complement Factor I (CFI), a family of soluble serine proteases, can regulate the complement system by inactivating C3b and C4b [41]. However, less research has been reported on CFI in periodontitis and MS, and the evidence below suggests that CFI may participate in both diseases by regulating the complement system. Accumulated evidence has demonstrated that the complement system is implicated in multiple neurodegenerative diseases. It has been shown that the complement system is activated at the onset of MS, and the expression levels of C3 and C4 are increased [42]. In addition, the accumulation of C3b can cause damage to neurons through the activation of C5a [43]. The expression of C3, C3b, and C4b was also discovered to be elevated in the gingival tissue of individuals with periodontitis, and its expression was found to be positively connected with the severity of the condition. Meanwhile, using C3b/C4b inhibitors can alleviate alveolar bone loss in periodontitis [44]. These findings suggest that CFI may influence periodontitis-mediated MS by regulating the transformation of C3b and C4b.
In summary, our study revealed a correlation between periodontitis and MS using bioinformatic analyses, suggesting that MS can be prevented by improving oral hygiene and treating periodontitis, and providing guidance for the treatment of patients with periodontitis combined with MS. More importantly, FAM46C, SLC7A7, LY96, CFI, DDIT4L, CD14, C5AR1 and IGJ were the most significant crosstalk genes between periodontitis and MS, and CFI, DDIT4L, FAM46C can be used as potential biomarkers for the diagnosis of periodontitis and MS. Immune responses driven by B cells and T cells are crucial in the pathogenesis of periodontitis and MS.
Data availability
Publicly available datasets were analyzed in this study. This data can be found at GEO data repository (https://www.ncbi.nlm.nih.gov/geo/) and include the accession numbers: GSE16134, GSE108000, GSE135511, GSE1334 and GSE38010.
References
Gao X, Guo Z, Wang P, Liu Z, Wang Z. Transcriptomic analysis reveals the potential crosstalk genes and immune relationship between IgA nephropathy and periodontitis. Front Immunol. 2023;14:1062590. https://doi.org/10.3389/fimmu.2023.1062590.
Sheu JJ, Lin HC. Association between multiple sclerosis and chronic periodontitis: a population-based pilot study. Eur J Neurol. 2013;20(7):1053–9. https://doi.org/10.1111/ene.12103.
Alvarenga MOP, Frazão DR, de Matos IG, Bittencourt LO, Fagundes NCF, Rösing CK, Maia LC, Lima RR. Is there any Association between neurodegenerative diseases and periodontitis? A systematic review. Front Aging Neurosci. 2021;13:651437. https://doi.org/10.3389/fnagi.2021.651437.
Li H, Sun Y, Chen R. Constructing and validating a diagnostic nomogram for multiple sclerosis via bioinformatic analysis. 3 Biotech. 2021;11(3):127. https://doi.org/10.1007/s13205-021-02675-1.
Zhang X, Song Y, Chen X, Zhuang X, Wei Z, Yi L. Integration of genetic and Immune Infiltration insights into Data Mining of multiple sclerosis pathogenesis. Comput Intell Neurosci. 2022;2022:1661334. https://doi.org/10.1155/2022/1661334.
Marrodan M, Alessandro L, Farez MF, Correale J. The role of infections in multiple sclerosis. Mult Scler. 2019;25(7):891–901. https://doi.org/10.1177/1352458518823940.
Zangeneh Z, Abdi-Ali A, Khamooshian K, Alvandi A, Abiri R. Bacterial variation in the oral microbiota in multiple sclerosis patients. PLoS ONE. 2021;16(11):e0260384. https://doi.org/10.1371/journal.pone.0260384.
Li X, Kiprowska M, Kansara T, Kansara P, Li P. Neuroinflammation: a distal consequence of Periodontitis. J Dent Res. 2022;101(12):1441–9. https://doi.org/10.1177/00220345221102084.
Harris MA, Clark J, Ireland A, Lomax J, Ashburner M, Foulger R, Eilbeck K, Lewis S, Marshall B, Mungall C, et al. The Gene Ontology (GO) database and informatics resource. Nucleic Acids Res. 2004;32(Database issue):D258–261. https://doi.org/10.1093/nar/gkh036.
Kanehisa M, Goto S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 2000;28(1):27–30. https://doi.org/10.1093/nar/28.1.27.
Kanehisa M, Furumichi M, Sato Y, Kawashima M, Ishiguro-Watanabe M. KEGG for taxonomy-based analysis of pathways and genomes. Nucleic Acids Res. 2023;51(D1):D587–d592. https://doi.org/10.1093/nar/gkac963.
Kanehisa M. Toward understanding the origin and evolution of cellular organisms. Protein Science: A Publication of the Protein Society. 2019;28(11):1947–51. https://doi.org/10.1002/pro.3715.
Botelho J, Machado V, Mendes JJ, Mascarenhas P. Causal Association between Periodontitis and Parkinson’s Disease: A Bidirectional Mendelian Randomization Study. Genes. 2021;12(5). https://doi.org/10.3390/genes12050772.
Liang S, Artificial Intelligence on High Throughput Data for Biomedical Research. Comb Chem High Throughput Screen. 2021;24(7):891–2. https://doi.org/10.2174/138620732407210504084747.
Gao M, Ling M, Tang X, Wang S, Xiao X, Qiao Y, Yang W, Yu R. Comparison of high-throughput single-cell RNA sequencing data processing pipelines. Brief Bioinform. 2021;22(3). https://doi.org/10.1093/bib/bbaa116.
Yu YD, Xue YT, Li Y. Identification and verification of feature biomarkers associated in heart failure by bioinformatics analysis. Sci Rep. 2023;13(1):3488. https://doi.org/10.1038/s41598-023-30666-0.
Liang Y, Lin F, Huang Y. Identification of biomarkers Associated with diagnosis of Osteoarthritis patients based on Bioinformatics and Machine Learning. J Immunol Res. 2022;2022:5600190. https://doi.org/10.1155/2022/5600190.
Mombelli A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontol 2000. 2018;76(1):85–96. https://doi.org/10.1111/prd.12147.
Shapira L, Ayalon S, Brenner T. Effects of Porphyromonas gingivalis on the central nervous system: activation of glial cells and exacerbation of experimental autoimmune encephalomyelitis. J Periodontol. 2002;73(5):511–6. https://doi.org/10.1902/jop.2002.73.5.511.
Gao Y, Zhang P, Wei Y, Ye C, Mao D, Xia D, Luo Y. Porphyromonas gingivalis exacerbates alcoholic liver disease by altering gut microbiota composition and host immune response in mice. J Clin Periodontol. 2023;50(9):1253–63. https://doi.org/10.1111/jcpe.13833.
Pakpoor J, Goldacre R, Disanto G, Giovannoni G, Goldacre MJ. Alcohol misuse disorders and multiple sclerosis risk. JAMA Neurol. 2014;71(9):1188–9. https://doi.org/10.1001/jamaneurol.2014.1795.
Potempa J, Banbula A, Travis J. Role of bacterial proteinases in matrix destruction and modulation of host responses. Periodontol 2000. 2000;24:153–92. https://doi.org/10.1034/j.1600-0757.2000.2240108.x.
Hajishengallis G. Complement and periodontitis. Biochem Pharmacol. 2010;80(12):1992–2001. https://doi.org/10.1016/j.bcp.2010.06.017.
Magliozzi R, Hametner S, Facchiano F, Marastoni D, Rossi S, Castellaro M, Poli A, Lattanzi F, Visconti A, Nicholas R, et al. Iron homeostasis, complement, and coagulation cascade as CSF signature of cortical lesions in early multiple sclerosis. Ann Clin Transl Neurol. 2019;6(11):2150–63. https://doi.org/10.1002/acn3.50893.
Sun X, Gao J, Meng X, Lu X, Zhang L, Chen R. Polarized macrophages in Periodontitis: characteristics, function, and Molecular Signaling. Front Immunol. 2021;12:763334. https://doi.org/10.3389/fimmu.2021.763334.
Guan X, He Y, Li Y, Shi C, Wei Z, Zhao R, Han Y, Pan L, Yang J, Hou T. Gremlin aggravates periodontitis via activation of the nuclear factor-kappa B signaling pathway. J Periodontol. 2022;93(10):1589–602. https://doi.org/10.1002/jper.21-0474.
Mc Guire C, Prinz M, Beyaert R, van Loo G. Nuclear factor kappa B (NF-κB) in multiple sclerosis pathology. Trends Mol Med. 2013;19(10):604–13. https://doi.org/10.1016/j.molmed.2013.08.001.
Gu Y, Han X. Toll-like Receptor Signaling and Immune Regulatory Lymphocytes in Periodontal Disease. Int J Mol Sci. 2020;21(9). https://doi.org/10.3390/ijms21093329.
Song B, Zhang YL, Chen LJ, Zhou T, Huang WK, Zhou X, Shao LQ. The role of toll-like receptors in periodontitis. Oral Dis. 2017;23(2):168–80. https://doi.org/10.1111/odi.12468.
Comi G, Bar-Or A, Lassmann H, Uccelli A, Hartung HP, Montalban X, Sørensen PS, Hohlfeld R, Hauser SL. Role of B cells in multiple sclerosis and related disorders. Ann Neurol. 2021;89(1):13–23. https://doi.org/10.1002/ana.25927.
Vakrakou AG, Alexaki A, Brinia ME, Anagnostouli M, Stefanis L, Stathopoulos P. The mTOR Signaling Pathway in multiple sclerosis; from animal models to Human Data. Int J Mol Sci. 2022;23(15). https://doi.org/10.3390/ijms23158077.
Fletcher JM, Lalor SJ, Sweeney CM, Tubridy N, Mills KH. T cells in multiple sclerosis and experimental autoimmune encephalomyelitis. Clin Exp Immunol. 2010;162(1):1–11. https://doi.org/10.1111/j.1365-2249.2010.04143.x.
Zhuang X, Lu M. The potential functions of FAM46C in oral squamous cell carcinoma. OncoTargets and Therapy. 2018;11:8915–23. https://doi.org/10.2147/ott.S185244.
Yang J, Zhu Y, Duan D, Wang P, Xin Y, Bai L, Liu Y, Xu Y. Enhanced activity of macrophage M1/M2 phenotypes in periodontitis. Arch Oral Biol. 2018;96:234–42. https://doi.org/10.1016/j.archoralbio.2017.03.006.
Kuntzel T, Bagnard D. Manipulating Macrophage/Microglia polarization to Treat Glioblastoma or multiple sclerosis. Pharmaceutics. 2022;14(2). https://doi.org/10.3390/pharmaceutics14020344.
Yang C, Ni B, Li C, Sun W, Wang Z, Wang H, Hou X, Yan S, Wang X, Xu D. circRNA_17725 Promotes Macrophage Polarization towards M2 by Targeting FAM46C to Alleviate Arthritis. Mediators of inflammation 2023; 2023:6818524. https://doi.org/10.1155/2023/6818524.
Simonson B, Subramanya V, Chan MC, Zhang A, Franchino H, Ottaviano F, Mishra MK, Knight AC, Hunt D, Ghiran I, et al. DDiT4L promotes autophagy and inhibits pathological cardiac hypertrophy in response to stress. Sci Signal. 2017;10(468). https://doi.org/10.1126/scisignal.aaf5967.
Deretic V, Saitoh T, Akira S. Autophagy in infection, inflammation and immunity. Nat Rev Immunol. 2013;13(10):722–37. https://doi.org/10.1038/nri3532.
Kim WJ, Park SY, Kim OS, Park HS, Jung JY. Autophagy upregulates inflammatory cytokines in gingival tissue of patients with periodontitis and lipopolysaccharide-stimulated human gingival fibroblasts. J Periodontol. 2022;93(3):380–91. https://doi.org/10.1002/jper.21-0178.
Zheng J, Zhu X, He Y, Hou S, Liu T, Zhi K, Hou T, Gao L. CircCDK8 regulates osteogenic differentiation and apoptosis of PDLSCs by inducing ER stress/autophagy during hypoxia. Ann N Y Acad Sci. 2021;1485(1):56–70. https://doi.org/10.1111/nyas.14483.
Lv W, Ma A, Chi X, Li Q, Pang Y, Su P. A novel complement factor I involving in the complement system immune response from Lampetra Morii. Fish Shellfish Immunol. 2020;98:988–94. https://doi.org/10.1016/j.fsi.2019.11.017.
Finehout EJ, Franck Z, Lee KH. Complement protein isoforms in CSF as possible biomarkers for neurodegenerative disease. Dis Markers. 2005;21(2):93–101. https://doi.org/10.1155/2005/806573.
Watkins LM, Neal JW, Loveless S, Michailidou I, Ramaglia V, Rees MI, Reynolds R, Robertson NP, Morgan BP, Howell OW. Complement is activated in progressive multiple sclerosis cortical grey matter lesions. J Neuroinflamm. 2016;13(1):161. https://doi.org/10.1186/s12974-016-0611-x.
Huang RY, Tseng FY, You JJ, Van Dyke TE, Cheng CD, Sung CE, Weng PW, Shieh YS, Cheng WC. Targeting therapeutic agent against C3b/C4b, SB002, on the inflammation-induced bone loss in experimental periodontitis. J Clin Periodontol. 2023;50(5):657–70. https://doi.org/10.1111/jcpe.13772.
Funding
This work was supported by the National Natural Science Foundation of China (82071770); Research Level Improvement Project of Anhui Medical University (2021xkjT001); Anhui Provincial Natural Science Foundation (2008085QH371); Scientific Research of BSKY in Anhui Medical University (XJ201601); Research and practical innovation projects of AHMU (YJS20230039); 2022 Disciplinary Construction Project in School of Dentistry, Anhui Medical University (2022xkfyhz02); and the Anhui Province Health Research Project (AHWJ2022b055).
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the conception and design of the study. E.W. and M.C. designed the project and wrote the manuscript. X.Z., T.W., S.S., M.S., and L.W. performed collection and/or assembly of data, data analysis, and interpretation. L.Z. and W.S. gave final approval of manuscript and financial support. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Affiliated Stomatology Hospital of Anhui Medical University and the First Affiliated Hospital of Anhui Medical University. All methods were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, E., Cheng, M., Zhang, X. et al. Exploration of potential shared gene signatures between periodontitis and multiple sclerosis. BMC Oral Health 24, 75 (2024). https://doi.org/10.1186/s12903-023-03846-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03846-7