
Abstract
Background
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among women. Dyslipidemia is a prevalent metabolic abnormality in individuals with PCOS. Moreover, vitamin D deficiency is widespread across all societal strata, with a particularly heightened prevalence observed in patients afflicted with PCOS. The present study aimed to investigate the level of vitamin D and its correlation with lipid profiles in Iranian women diagnosed with PCOS.
Methods
This cross-sectional study was carried out at the PCOS and infertility clinic of Arash Women’s Hospital in Tehran. The study encompassed the medical records of PCOS patients who attended the clinic from March 2021 to December 2023. All patients underwent blood tests, which included assessments of fasting blood sugar levels, lipid profiles, and 25-hydroxyvitamin D (25(OH)D) levels. The investigation focused on evaluating the relationship between vitamin D levels and lipid profiles. Statistical analyses, including the chi-square test and Spearman’s correlation coefficient, were employed to analyze the data.
Results
A total of 1004 women diagnosed with PCOS were included in the study. The age range of the participants was 14 to 46 years. The majority of the participants had a body mass index (BMI) within the normal range (n = 555, 55.3%). The median vitamin D level among the participants was 26.00 (IQR: 19.00–34.00). The relationship between vitamin D levels and lipid profile parameters was assessed, revealing no significant correlation between vitamin D levels and low-density lipoprotein (LDL) (r = 0.021, p = 0.505), high-density lipoprotein (HDL) (r = 0.011, p = 0.719), or triglyceride (TG) (r = -0.026, p = 0.417) levels, both in non-adjusted and age-adjusted analyses.
Conclusion
According to the present study, there was no significant correlation between serum 25(OH)D deficiency and elevated TG or LDL levels or decreased HDL levels in PCOS patients. Nevertheless, further prospective studies are needed to determine whether there is a causal relationship between vitamin D deficiency and lipid profile alterations, specifically among PCOS patients.
Similar content being viewed by others

Background
Polycystic ovary syndrome (PCOS) is a complicated condition that affects 6–26% of women around the world [1]. this condition is characterized by various clinical symptoms, such as irregular menstrual cycles, infertility, and high levels of androgen hormones. Additionally, PCOS may also cause metabolic disturbances, including obesity, hypertension, dyslipidemia, and hyperinsulinemia [2]. Dyslipidemia, a prevalent metabolic anomaly in this demographic, has a prevalence rate of 70% [3] and is associated with reduced levels of high-density lipoprotein-cholesterol (HDL-c) and apolipoprotein A-I (apo A-I), as well as elevated levels of triglyceride (TG), ApoB, low-density lipoprotein cholesterol (LDL-c) and very low-density lipoprotein cholesterol (VLDL-c) [4,5,6,7]. Vitamin D deficiency is known to be more frequent in individuals with PCOS, and it can worsen metabolic and endocrine dysregulations, potentially increasing the risk of dyslipidemia [8, 9]. The relationship between 25-hydroxyvitamin D (25(OH)D) concentration and lipid profiles has been explored in several studies, but the findings have been inconsistent across different populations [10,11,12,13]. While some studies have shown a strong association between vitamin D deficiency and elevated lipid levels, as well as an increased risk of cardiovascular diseases [14,15,16], there is a need for further research to validate these claims [17]. Notably, a study conducted in Iran found no effect of vitamin D deficiency on the lipid profile [18]. However, Atasayan demonstrated an inverse correlation between vitamin D levels and cardiovascular disease risk in women with PCOS [19]. Considering the importance of managing lipid levels to prevent cardiovascular disease in women with PCOS [20,21,22,23], screening and intervention strategies are crucial. By examining the correlation between vitamin D levels and lipid profiles in this cross-sectional study, we aim to contribute to the understanding of this relationship. The findings of our research may have implications for improving management strategies for women with PCOS, ultimately reducing their cardiovascular risk.
Methods & materials
This cross-sectional study is approved by the Ethics Committee of the Research Vice-Chancellor of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1402.582) and is conducted at Arash Hospital in Tehran between March 2021 and December 2023. The study population consisted of women diagnosed with PCOS who had been referred to the PCOS and infertility clinic at Arash Hospital as outpatients with common complaints related to this syndrome. The diagnosis of PCOS was based on the Rotterdam diagnostic criteria, which require the presence of at least two out of three indicators: lack of ovulation or oligo-ovulation, clinical or laboratory evidence of increased androgen levels, and polycystic ovary appearance on ultrasound [24]. According to WHO definition of infertility, we defined infertility as an inability to conceive after 12 months or more of regular unprotected sexual contact.
The exclusion criteria for this study were hereditary adrenal hyperplasia, Cushing’s syndrome, a history of autoimmune disease, diabetes, liver or kidney organ failure, hyperprolactinemia, hypothyroidism, androgens secreting tumors, and the use of immunosuppressive medications or vitamin D supplementation within the past three months.
Patient demographic details, medical history, and reproductive history information were obtained from their medical records. According to the criteria outlined in the article by Hirschler et al., weight, height, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were measured and recorded [21].
Laboratory measurement
The participants were sampled following a minimum of 10 h of fasting, between 8 and 10 am. Serum levels of anti-Müllerian hormone (AMH) were determined using two-site enzyme immunoassay (EIA). Lipid profiles, including, TG, LDL and HDL levels, were measured using standard enzymatic method (Pars Azmoon kits, Tehran, Iran). Fasting blood sugar (FBS) was concurrently measured in the same hospital laboratory using same kits. The body mass index (BMI) was calculated by dividing weight (in kilograms) by height (in meters) squared. The serum level of 25(OH)D was measured using the Enzyme-linked immunosorbent assay method (ELISA) and the BXE0111kit manufactured in Iran. Vitamin D levels were classified according to the criteria established by the Endocrine Society, with levels below 29 ng/mL considered deficient and levels of 30 ng/mL or higher considered normal. A normal lipid profile was defined as LDL < 130 mg/dL, HDL > 30 mg/dL, or TG < 150 mg/dL [25].
Sample size calculation
We conducted a sample size estimation using the correlation bivariate normal model in G*Power 3.1.9.4. The parameters used were as follows: Correlation Coefficient (ρ): 0.1; Significance Level (α): 0.05; and Power (1 - β): 0.88. Based on these inputs, the calculated sample size required for our study reached 1004 samples.
Statistical analyses
Statistical analysis was performed using SPSS (version 21; SPSS, Inc., Chicago, IL, USA), with a significance level set at P < 0.05. The Mann‒Whitney U test was used to compare quantitative variables between the groups. The chi-square test was used to compare qualitative variables among the groups. Given the aim of investigating the relationship between vitamin D levels and lipid profiles rather than establishing causality or association, Spearman’s correlation method was employed. This method is suitable for analyzing non-normally distributed variables. By using this method, we can assess the strength and direction of the relationship between vitamin D status and lipid profiles, providing insights into the potential relationship between these variables in women with PCOS.
Ethical considerations
This cross-sectional study was approved by the Ethics Committee of the Research Vice-Chancellor of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1402.582) and was conducted at Arash Hospital in Tehran, Iran. Informed consent was obtained from each participant before the survey began, and all data collection forms were anonymized.
This cross-sectional study was approved by the Ethics Committee of the Research Vice-Chancellor of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1402.582) and was conducted at Arash Hospital in Tehran, Iran. Informed consent was obtained from each participant before the survey began, and all data collection forms were anonymized. Our study adhered to the principles outlined in the Helsinki Declaration.
Results
Participant characteristics
A total of 1004 women diagnosed with PCOS were included in the study. The age range of the participants was 14 to 46 years. The majority of participants had a BMI within the normal range (n = 555, 55.3%). The median vitamin D level among the participants was 26.00 (IQR: 19.00–34.00). The baseline characteristics of the participants are summarized in Table 1.
Participants with vitamin D deficiency exhibited significantly higher rates of infertility compared to those with normal vitamin D levels, as indicated in Table 2.
Vitamin D levels and lipid profile
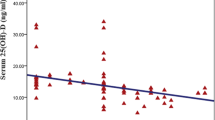
We utilized Spearman correlation analysis to assess the relationship between vitamin D levels and lipid profile parameters due to the non-normal distribution of the variables. Our findings revealed no significant correlation between vitamin D levels and LDL (r = 0.021, p = 0.505), HDL (r = 0.011, p = 0.719), or TG (r = -0.026, p = 0.417) (Figs. 1, 2 and 3). Furthermore, when controlling for age as a confounding factor, no significant correlation between vitamin D levels and lipid profiles was observed. However, we did find a significant correlation between vitamin D levels and AMH amounts (r = -0.070, p = 0.026), this correlation was not significant after adjusting for age (r = 0.008, p = 0.794) (Tables 3 and 4).

Comparison of the Medians of TG, LDL, and HDL levels between the vitamin D deficient and normal vitamin D levels groups. Triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL)

Comparison of the maximum TG, LDL, and HDL levels between the vitamin D-deficient and normal vitamin D-level groups. Triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL)

Comparison of the minimum TG, LDL, and HDL levels between the vitamin D-deficient and normal vitamin D-level groups. Triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL)
Subgroup analysis
Subgroup analysis was performed based on BMI categories to further explore the relationship between vitamin D levels and lipid profiles. Among the overweight or obese subgroup (BMI ≥ 25), a significant correlation was found between vitamin D levels and HDL cholesterol (r = 0.101, p = 0.042). However, the correlation was not found to be significant for LDL (r = -0.063, p = 0.209) or TG levels (r = -0.082, p = 0.099). In contrast, no significant correlation was observed between any of the lipid profile parameters and vitamin D status within normal BMI.
Discussion
This cross-sectional study aimed to evaluate the relationship between vitamin D levels and lipid profiles in women with PCOS using Spearman correlation analysis. The findings indicated no significant correlation between vitamin D levels and LDL-C, HDL, or TG levels. However, subgroup analysis revealed a significant correlation between vitamin D levels and HDL among the overweight or obese subgroup. These results suggest that higher vitamin D levels may not be associated with improved lipid profiles in PCOS patients. Furthermore, our analysis demonstrated a significant association between vitamin D levels and AMH levels but this relationship was not significant after adjusting for age suggesting the original correlation was merely a result of age-related effects.
This study unveiled a significant deficiency in vitamin D among PCOS patients, with a striking 61% registering vitamin D levels below 29 ng/dl. This concern transcends the geographic scope of the study’s origin and mirrors a global issue, with Li et al. finding that 72% of PCOS women are either deficient or insufficient [26]. Multiple studies have highlighted the correlation between vitamin D deficiency and the development of PCOS [27, 28]. In contrast to our findings, Wang et al. reported a negative correlation between serum 25(OH)D concentrations and total cholesterol and LDL-C in women with PCOS, alongside a positive correlation with HDL-C [28]. However, our results align with those of Li et al., who reported no significant correlation between serum 25(OH) D concentrations and TG levels. These findings suggest that maintaining adequate vitamin D levels may not impact TG levels in PCOS patients [29]. Huang et al. observed that vitamin D-deficient overweight or obese individuals display elevated levels of TG, total cholesterol, and LDL, as well as decreased HDL [30].
Three studies have reported an inverse relationship between serum 25(OH)D3 concentrations and triglyceride (TG) levels in patients with PCOS [31,32,33]. Conversely, seven studies have shown no clear link between lipid profiles and 25(OH)D serum levels [34,35,36,37,38,39,40]. the discrepancies may stem from various factors, including sample size, population characteristics, participant habits, and racial disparities. Addressing these variations, multicenter two-group studies have been proposed to explore the correlation between serum vitamin D concentration and lipid profile in women with PCOS.
The relationship between vitamin D status and lipid profiles is not fully understood, but there are several possible explanations [41]. One theory suggests that higher levels of vitamin D can increase the activity of the lipoprotein lipase enzyme in adipose tissue. This could explain the inverse relationship between the serum 25- hydroxyvitamin D concentration and TG levels [42]. Additionally, vitamin D may indirectly influence the lipid profile by modulating parathormone activity, and in vitro studies have indicated that parathormone can reduce lipolysis [43].
It is well established that vitamin D plays a crucial role in maintaining calcium homeostasis. Research indicates that it can significantly reduce the hepatic secretion of TG by elevating calcium levels [44, 45]. Calcium intake reduces fatty acid absorption [46, 47]. Increased calcium absorption facilitated by vitamin D may consequently lead to reductions in cholesterol, TG, and LDL levels [48]. Furthermore, vitamin D is associated with lower TG levels, potentially due to heightened lipoprotein lipase activity and increased leptin production, which can diminish lipogenesis and enhance lipolysis [49].
Notably, vitamin D deficiency in overweight or obese adults may inhibit lipoprotein lipase gene expression and lead to dyslipidemia, while hyperparathyroidism can also distort serum vitamin D levels and contribute to lipid profile alterations [50, 51]. Although the exact mechanisms underlying these associations remain elusive, these findings underscore the importance of maintaining adequate vitamin D levels and monitoring hormone function in overweight or obese individuals.
Future studies should explore the impact of lipoprotein lipase levels and hyperparathyroidism status on patients, although confirming these findings will necessitate additional randomized clinical trials.
The strength of our study lies in its large sample size and careful participant selection, which enhances the generalizability of the findings. By including a substantial number of participants, we were able to reduce the likelihood of sampling bias and increase the statistical power of the study. The utilization of Spearman correlation analysis allowed for the examination of non-linear relationships, providing a more nuanced understanding of the issue. Additionally, our study contributes to the existing literature by exploring the association between vitamin D levels and lipid profiles in different subgroups, particularly the overweight or obese subgroup.
Limitations
The findings of Our study are subject to several limitations. First, the presence of confounding factors may have influenced the results. Our study did not consider factors such as dietary fat intake, insulin resistance, and testosterone levels. Furthermore, our study did not include an assessment of total cholesterol levels which limits the interpretation of our findings. Future studies should consider the inclusion of total cholesterol measurements to provide a more comprehensive assessment.
Conclusion
In conclusion, our study did not reveal a significant correlation between vitamin D deficiency and elevated TG, or LDL levels or between vitamin D deficiency and reduced HDL levels in PCOS patients. However, further prospective investigations are warranted to elucidate whether a causal relationship exists between vitamin D deficiency and alterations in lipid profiles among overweight or obese individuals with PCOS. These insights are crucial for advancing our understanding of the complex interplay between vitamin D and lipid metabolism in the PCOS population.
Data availability
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
References
Butt MS, Saleem J, Zakar R, Aiman S, Khan MZ, Fischer F. Benefits of physical activity on reproductive health functions among polycystic ovarian syndrome women: a systematic review. BMC Public Health. 2023;23(1):882.
Jin B, Qian L, Fu X, Zhu J, Shu J. Influence of vitamin D supplementation on lipid levels in polycystic ovary syndrome patients: a meta-analysis of randomized controlled trials. J Int Med Res. 2020;48(8):0300060520935313.
Legro RS, Kunselman AR, Dunaif A. Prevalence and predictors of dyslipidemia in women with polycystic ovary syndrome. Am J Med. 2001;111(8):607–13.
Sniderman AD, Scantlebury T, Cianflone K. Hypertriglyceridemic hyperapob: the unappreciated atherogenic dyslipoproteinemia in type 2 diabetes mellitus. Ann Intern Med. 2001;135(6):447–59.
Barter PJ, Brewer HB Jr, Chapman MJ, Hennekens CH, Rader DJ, Tall AR. Cholesteryl Ester transfer protein: a novel target for raising HDL and inhibiting atherosclerosis. Arteriosclerosis, thrombosis, and vascular biology. 2003;23(2):160–7.
Brunzell JD, Ayyobi AF. Dyslipidemia in the metabolic syndrome and type 2 diabetes mellitus. Am J Med. 2003;115(8):24–8.
Taskinen M-R. LDL-cholesterol, HDL-cholesterol or triglycerides—which is the culprit? Diabetes research and clinical practice. 2003;61:S19–26.
He C, Lin Z, Robb SW, Ezeamama AE. Serum vitamin D levels and polycystic ovary syndrome: a systematic review and meta-analysis. Nutrients. 2015;7(6):4555–77.
Kostrova G, Malyavskaya S, Lebedev A. Relationship between vitamin D level and lipid profile in young adults. Vopr Pitan. 2022;91(4):26–34.
Lupton JR, Faridi KF, Martin SS, Sharma S, Kulkarni K, Jones SR, et al. Deficient serum 25-hydroxyvitamin D is associated with an atherogenic lipid profile: the very large database of lipids (VLDL-3) study. J Clin Lipidol. 2016;10(1):72–81. e1.
Tepper S, Shahar D, Geva D, Avizohar O, Nodelman M, Segal E, et al. Identifying the threshold for vitamin D insufficiency in relation to cardiometabolic markers. Nutr Metabolism Cardiovasc Dis. 2014;24(5):489–94.
Muscogiuri G, Mitri J, Mathieu C, Badenhoop K, Tamer G, Orio F, et al. Mechanisms in endocrinology: vitamin D as a potential contributor in endocrine health and disease. Eur J Endocrinol. 2014;171(3):R101–10.
Savastano S, Valentino R, Di Somma C, Orio F, Pivonello C, Passaretti F, et al. Serum 25-Hydroxyvitamin D levels, phosphoprotein enriched in diabetes gene product (PED/PEA-15) and leptin-to-adiponectin ratio in women with PCOS. Nutr Metabolism. 2011;8:1–8.
Wang TJ. Vitamin D and cardiovascular disease. Annu Rev Med. 2016;67:261–72.
Alyami AM, Lam V, Soares MJ, Zhao Y, Sherriff JL, Mamo JC, et al. The association of vitamin D status with dyslipidaemia and biomarkers of endothelial cell activation in older australians. Nutrients. 2016;8(8):457.
Jiang X, Peng M, Chen S, Wu S, Zhang W. Vitamin D deficiency is associated with dyslipidemia: a cross-sectional study in 3788 subjects. Curr Med Res Opin. 2019;35(6):1059–63.
Luo J, Li T, Yuan J. Effectiveness of vitamin D supplementation on lipid profile in polycystic ovary syndrome women: a meta-analysis of randomized controlled trials. Annals Palliat Med. 2021;10(1):11429–129.
Mazloum Khorasani Z, Bonakdaran S. Relation between vitamin D deficiency and metabolic disturbance in PCOS. Med J Mashhad Univ Med Sci. 2015;58(1):1–6.
Atasayan K, Yoldemir T. The effect of PCOS status on atherosclerosis markers and cardiovascular disease risk factors in young women with vitamin D deficiency. Gynecol Endocrinol. 2021;37(3):225–9.
Kim MR, Jeong SJ. Relationship between vitamin D level and lipid profile in non-obese children. Metabolites. 2019;9(7):125.
Hirschler V, Maccallini G, Molinari C, Aranda C, Group SAdlCS. Low vitamin D concentrations among indigenous Argentinean children living at high altitudes. Pediatr Diabetes. 2013;14(3):203–10.
Mark S, Gray-Donald K, Delvin EE, O’Loughlin J, Paradis G, Levy E, et al. Low vitamin D status in a representative sample of youth from Quebec, Canada. Clin Chem. 2008;54(8):1283–9.
Kim JJ, Choi YM. Dyslipidemia in women with polycystic ovary syndrome. Obstet Gynecol Sci. 2013;56(3):137.
Revised. 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41 – 7.
Tehrani FR, Erfani H, Cheraghi L, Tohidi M, Azizi F. Lipid profiles and ovarian reserve status: a longitudinal study. Hum Reprod. 2014;29(11):2522–9.
Li C, Ford E, Mokdad A, Cook S. Recent trends in waist circumference and waist-height Ratio among US children and adolescents. 2007. 2006.
Gokosmanoglu F, Onmez A, Ergenç H. The relationship between vitamin D deficiency and polycystic ovary syndrome. Afr Health Sci. 2020;20(4):1880–6.
Wang L, Lv S, Li F, Yu X, Bai E, Yang X. Vitamin D deficiency is associated with metabolic risk factors in women with polycystic ovary syndrome: a cross-sectional study in Shaanxi China. Front Endocrinol. 2020;11:171.
Li HWR, Brereton RE, Anderson RA, Wallace AM, Ho CK. Vitamin D deficiency is common and associated with metabolic risk factors in patients with polycystic ovary syndrome. Metabolism. 2011;60(10):1475–81.
Huang X, Yang Y, Jiang Y, Zhou Z, Zhang J. Association between vitamin D deficiency and lipid profiles in overweight and obese adults: a systematic review and meta-analysis. BMC Public Health. 2023;23(1):1653.
Yildizhan R, Kurdoglu M, Adali E, Kolusari A, Yildizhan B, Sahin HG, et al. Serum 25-hydroxyvitamin D concentrations in obese and non-obese women with polycystic ovary syndrome. Arch Gynecol Obstet. 2009;280:559–63.
Kozakowski J, Kapuścińska R, Zgliczyński W. Associations of vitamin D concentration with metabolic and hormonal indices in women with polycystic ovary syndrome presenting abdominal and gynoidal type of obesity. Ginekologia Polska. 2014;85(10).
Lu Z, Pan X, Hu Y, Hao Y, Luo Y, Hu X, et al. Serum vitamin D levels are inversely related with non-alcoholic fatty liver disease independent of visceral obesity in Chinese postmenopausal women. Clin Exp Pharmacol Physiol. 2015;42(2):139–45.
Gariballa S, Shah I, Yasin J, Alessa A, Vitamin D. [25 (OH) D] metabolites and epimers in obese subject: interaction and correlations with adverse metabolic health risk factors. J Steroid Biochem Mol Biol. 2022;215:106023.
Dominoni LAC, Gabiatti MP, Piazza FR, Streb AR, Del Duca GF, Hansen F. Vitamin D is associated with body composition and fat intake, but not with cardiometabolic parameters in adults with obesity. Nutr Res. 2022;105:97–104.
Bellia A, Garcovich C, D’Adamo M, Lombardo M, Tesauro M, Donadel G, et al. Serum 25-hydroxyvitamin D levels are inversely associated with systemic inflammation in severe obese subjects. Intern Emerg Med. 2013;8:33–40.
Boonchaya-anant P, Holick MF, Apovian CM. Serum 25‐hydroxyvitamin D levels and metabolic health status in extremely obese individuals. Obesity. 2014;22(12):2539–43.
Mousa A, Naderpoor N, de Courten MP, Scragg R, de Courten B. 25-hydroxyvitamin D is associated with adiposity and cardiometabolic risk factors in a predominantly vitamin D-deficient and overweight/obese but otherwise healthy cohort. J Steroid Biochem Mol Biol. 2017;173:258–64.
Ong MW, Tan CH, Cheng AKS. Prevalence and determinants of vitamin D deficiency among the overweight and obese singaporeans seeking weight management including bariatric surgery: a relationship with bone health. Obes Surg. 2018;28:2305–12.
Curvello-Silva KL, Oliveira NA, Silva TS, Sousa CD, Daltro C. Association between cardiovascular risk factors and 25 (OH) D levels in obese patients. Metab Syndr Relat Disord. 2020;18(7):328–32.
Zemel MB. Regulation of adiposity and obesity risk by dietary calcium: mechanisms and implications. J Am Coll Nutr. 2002;21(2):S146–51.
Querfeld U, Hoffmann MM, EIFINGER F, ACKERSCHOTT M, KERN MICHALKD. Antagonistic effects of vitamin D and parathyroid hormone on lipoprotein lipase in cultured adipocytes. J Am Soc Nephrol. 1999;10(10):2158–64.
Wang J-H, Keisala T, Solakivi T, Minasyan A, Kalueff AV, Tuohimaa P. Serum cholesterol and expression of ApoAI, LXRβ and SREBP2 in vitamin D receptor knock-out mice. J Steroid Biochem Mol Biol. 2009;113(3–5):222–6.
Zittermann A, Frisch S, Berthold HK, Götting C, Kuhn J, Kleesiek K, et al. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am J Clin Nutr. 2009;89(5):1321–7.
Cho H-J, Kang H-C, Choi S-A, Ju Y-C, Lee H-S, Park H-J. The possible role of Ca2 + on the activation of microsomal triglyceride transfer protein in rat hepatocytes. Biol Pharm Bull. 2005;28(8):1418–23.
Denke MA, Fox MM, Schulte MC. Short-term dietary calcium fortification increases fecal saturated fat content and reduces serum lipids in men. J Nutr. 1993;123(6):1047–53.
Reid IR. Effects of calcium supplementation on circulating lipids: potential pharmacoeconomic implications. Drugs Aging. 2004;21:7–17.
Vaskonen T, Mervaala E, Sumuvuori V, Seppänen-Laakso T, Karppanen H. Effects of calcium and plant sterols on serum lipids in obese Zucker rats on a low-fat diet. Br J Nutr. 2002;87(3):239–45.
Abbas MA. Physiological functions of Vitamin D in adipose tissue. J Steroid Biochem Mol Biol. 2017;165:369–81.
Silverberg SJ. Vitamin D deficiency and primary hyperparathyroidism. J Bone Miner Res. 2007;22(S2):V100–4.
Procopio M, Barale M, Bertaina S, Sigrist S, Mazzetti R, Loiacono M, et al. Cardiovascular risk and metabolic syndrome in primary hyperparathyroidism and their correlation to different clinical forms. Endocrine. 2014;47(2):581–9.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
M.A., T.N., M.D., and F.H. wrote the main manuscript. M.D. and M.S.N. prepared Figs. 1, 2 and 3 and analyzed the data. A.A. and E.S. contributed to data gathering. All authors reviewed the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is approved by the Ethics Committee of the Research Vice-Chancellor of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1402.582) and is conducted at Arash Hospital in Tehran. Informed consent was obtained from each participant before the survey began, and all data collection forms were anonymized. Our study adhered to the principles of the Helsinki Declaration.
Consent for publication
We declare that we consent to publish our work in this journal and that we have obtained written consent from any individual whose personal information is included in this article.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Moieni, A., Haghollahi, F., Dashtkoohi, M. et al. Vitamin D levels and lipid profiles in patients with polycystic ovary syndrome. BMC Women's Health 24, 472 (2024). https://doi.org/10.1186/s12905-024-03294-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03294-7