
Abstract
Background
The relationship between A Body Shape Index (ABSI) and female infertility is not well understood. ABSI, a novel anthropometric measure, is gaining recognition for its ability to more accurately capture visceral fat characteristics than traditional metrics like BMI. This study aims to explore the association between ABSI and female infertility, considering its potential applications in medical screening and risk assessment.
Methods
This cross-sectional study analyzed data from the NHANES from 2013 to 2020. Female infertility was assessed through reproductive health questionnaires, and ABSI was calculated using waist circumference, BMI, and height. Weighted logistic regression models and trend tests were used to evaluate the association between ABSI and female infertility. Restricted cubic splines (RCS) were employed to explore potential nonlinear relationships. Subgroup analyses were conducted to examine the consistency of the association across various demographic and health-related factors. Sensitivity analyses were also performed, including the exclusion of participants with missing covariate data, the application of propensity score matching, and restricting the analysis to women aged 20–45 years.
Results
The study included 3,718 participants, 433 of whom were diagnosed with infertility. Higher ABSI was associated with an increased risk of female infertility (OR = 1.56, 95% CI: 1.21-2.00, P = 0.001), as demonstrated by weighted logistic regression and trend tests. Women in the highest ABSI quartile had a significantly higher prevalence of infertility compared to those in the lowest quartile (OR = 1.73, 95% CI: 1.27–2.37, P = 0.001). RCS curves indicated a linear positive relationship between ABSI and infertility risk, with a critical value at 0.079. Subgroup and sensitivity analyses confirmed the stability of these findings.
Conclusion
This study demonstrates a positive linear relationship between ABSI and the risk of female infertility. The use of a simple, non-invasive ABSI measurement could facilitate the early identification of high-risk individuals in large-scale screenings, potentially helping to prevent or reduce the incidence of infertility.
Similar content being viewed by others

Introduction
Infertility is a significant public health issue that affects women’s health and quality of life globally, impacting approximately 10–15% of women of reproductive age [1, 2]. Infertility imposes substantial psychological and emotional stress on women and has profound social and economic implications. The etiology of infertility is multifaceted, involving genetic, environmental, lifestyle, and metabolic factors, which create considerable challenges for effective prevention and treatment [3]. Therefore, identifying new and reliable markers for the prevention and management of infertility is crucial for improving the prognosis and quality of life for affected women.
Obesity has been shown to influence reproductive health through various mechanisms [4]. Specifically, visceral fat is considered more detrimental to reproductive health than subcutaneous fat [5, 6] due to its association with metabolic syndromes such as insulin resistance, hormonal imbalance, and immune dysfunction. These factors collectively impact women’s reproductive health through multiple pathways. Traditional measures like body mass index (BMI) are commonly used to assess obesity; however, they fail to accurately distinguish between visceral and subcutaneous fat [7, 8]. Metrics such as waist-to-hip ratio (WHR) and visceral adiposity index (VAI) are also used to evaluate visceral fat. While these measures address some limitations of BMI, they still have drawbacks. For instance, WHR is not highly precise in assessing visceral fat [9], and VAI, despite incorporating several metabolic parameters, is relatively complex to calculate and has limited applicability in large-scale screenings [10].
A Body Shape Index (ABSI) is a novel anthropometric measure designed to address the limitations of traditional obesity metrics [11]. ABSI is calculated using the formula: ABSI = WC / (BMI^(2/3) * Height^(1/2)). This calculation standardizes waist circumference by accounting for height and weight, providing a more precise estimate of abdominal obesity and visceral fat. Research has demonstrated that ABSI is a robust predictor of cardiovascular disease [12, 13], diabetes [14, 15], cognitive decline [16, 17], metabolic syndrome [18, 19], and mortality [14, 20]. By isolating the effects of central obesity from overall body fat, ABSI is particularly valuable in identifying individuals at high risk for metabolic conditions that BMI might overlook. Additionally, ABSI is straightforward to calculate and non-invasive, making it especially suitable for large-scale epidemiological screenings and clinical settings where rapid and accurate assessments are required. Nevertheless, no studies to date have systematically evaluated the relationship between ABSI and female infertility.
This study aims to utilize data from the National Health and Nutrition Examination Survey (NHANES) from 2013 to 2020 to assess the relationship between ABSI and female infertility and to explore ABSI’s potential as an independent predictor of infertility. By investigating this relationship, we aim to uncover the potential value of ABSI in assessing infertility risk, aiding healthcare professionals in better identifying and managing women at high risk of infertility, and providing a basis for future research on the relationship between visceral fat and women’s reproductive health.
Methods
Survey description
NHANES is a biennial survey conducted in the United States using a multistage probability sampling design to ensure a nationally representative sample. Data collection involves in-home interviews to gather demographic and health information, along with physical examinations and laboratory tests conducted in mobile examination centers to collect biological samples and clinical data. This study was approved by the Ethics Review Board of the National Center for Health Statistics (NCHS), and informed consent was obtained from all participants.
Study population
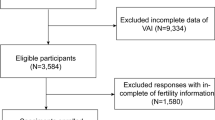
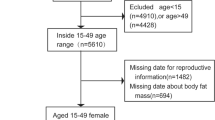
The NHANES survey from 2013 to 2020 included 44,960 participants. We excluded 22,173 male participants, 14,525 participants without infertility diagnosis data (those who answered “Refused,” “Don’t know,” or had “Missing” responses were excluded), 297 participants with missing ABSI data, 2,734 participants with missing weight data, and 1,513 participants aged over 50 or under 20. The final sample consisted of 3,718 female participants aged 20–50 years (Fig. 1).

Inclusion and exclusion criteria flowchart
Infertility assessment
Infertility was assessed during NHANES interviews based on the reproductive health question RHQ074: “Have you ever tried to get pregnant for a year or longer without success?” Participants who answered “yes” were classified as having infertility.
ABSI assessment
In this study, ABSI was the exposure variable. ABSI is calculated using BMI, waist circumference, and height. BMI is derived by dividing weight (kg) by height squared (m²). The formula for calculating ABSI is as follows [21, 22]:
Covariates
The covariates considered in this study included age (recorded in years), poverty-income ratio (PIR), age at menarche (recorded in years), infertility status (yes/no), race (categorized as White, Mexican, Black, and Other), alcohol use (yes/no), education level (less than high school, high school, and above high school), smoking status (yes/no), hypertension (yes/no), diabetes (yes/no), marital status (married, never married, and separated), and pregnancy history (yes/no). These data were collected through standardized questionnaires and interview procedures administered by NHANES. PIR was calculated by dividing household income by the poverty threshold, adjusted for family size [23, 24]. Smoking was defined as having smoked at least 100 cigarettes in a lifetime, and alcohol use was defined as having consumed at least 12 alcoholic drinks in a lifetime. Hypertension and diabetes were determined through self-report. Detailed information on the procedures for obtaining these covariates is available at www.cdc.gov/nchs/nhanes/.
Statistical analysis
To ensure national representativeness, appropriate weighting methods were applied. Baseline characteristics for continuous variables were expressed as means (standard errors), while categorical variables were presented as N (weighted percentage). Multiple imputation was used to address missing covariate data. Weighted logistic regression models were employed to examine the association between ABSI and infertility, with restricted cubic splines (RCS) used to explore potential nonlinear relationships. Subgroup analyses were conducted to evaluate the consistency of the association across various demographic and health-related factors, including race, education, marital status, pregnancy history, smoking status, alcohol use, diabetes, and hypertension. To assess the robustness of the relationship between ABSI and female infertility, three sensitivity analyses were performed. First, the association was re-evaluated using weighted logistic regression after excluding participants with missing covariate data. Second, propensity score matching (PSM) with 1:1 nearest neighbor matching was applied to further assess the significance of the association. Third, the analysis was restricted to participants aged 20–45 years to examine the association within this specific age group. Statistical significance was defined as P < 0.05, and all analyses were conducted using R software.
Results
Characteristics of study population
This study included 3,718 participants, of whom 433 were diagnosed with female infertility. Table 1 presents the weighted baseline characteristics of the study population, stratified by ABSI quartiles. Participants with higher ABSI scores tended to be older and had lower PIR. They also experienced menarche at a later age and had a higher prevalence of infertility. Significant racial differences were observed across ABSI quartiles, with a greater proportion of White and Mexican American women in the highest ABSI quartile. These participants also had lower education levels, lower rates of alcohol consumption, higher smoking rates, and a higher prevalence of hypertension and diabetes. Additionally, participants with higher ABSI scores were more likely to be married and have no history of pregnancy. These findings underscore the substantial differences in demographic, socioeconomic, and health-related variables across different ABSI quartiles.
Association between ABSI and female infertility
We assessed the relationship between ABSI and female infertility using weighted logistic regression (Table 2). In the fully adjusted model (Model 3), where ABSI was treated as a continuous variable, a significant positive association emerged between ABSI and female infertility (OR = 1.56, 95% CI: 1.21-2.00, P = 0.001). This indicates that higher ABSI is correlated with an increased risk of infertility. Further analysis by ABSI quartiles reinforced this finding, as the highest quartile exhibited a significantly greater prevalence of infertility compared to the lowest quartile (OR = 1.73, 95% CI: 1.27–2.37, P = 0.001). Trend analyses also demonstrated that women with higher ABSI had a significantly elevated risk of infertility (P < 0.001). Moreover, RCS curves depicted a linear positive relationship between ABSI and infertility risk, with a critical threshold at 0.08 (P for overall < 0.001, P for nonlinearity = 0.42) (Fig. 2). Additionally, the RCS curves illustrated a linear positive relationship between ABSI and infertility risk, with a critical value at 0.079 (P for overall < 0.001, P for nonlinearity = 0.42) (Fig. 2).

Non-linear relationship between ABSI and female infertility
Subgroup analysis
In subgroup analyses, we further investigated the influence of various demographic and health-related factors on the association between ABSI and female infertility (Fig. 3). The findings indicated that the positive association between ABSI and female infertility remained consistent across different subgroups, including race, education, marital status, pregnancy history, smoking status, alcohol use, hypertension, and diabetes. However, the interaction effects were not statistically significant. These subgroup analyses underscore the consistency and generalizability of the association between ABSI and female infertility risk across diverse populations.

Forest plot of stratified analysis and interaction effects for the association between ABSI and female infertility
Sensitivity analysis
To assess the robustness of the association between ABSI and female infertility, we conducted three sensitivity analyses: excluding participants with missing covariate data, applying PSM, and restricting the analysis to women aged 20–45 years. First, after excluding participants with missing covariate data, 3,286 participants remained, including 398 with infertility (Supplementary Table 1). The weighted multivariable regression confirmed a significant association between ABSI and infertility (OR = 1.51, 95% CI: 1.16–1.98, P = 0.004) (Supplementary Table 2). Second, we applied PSM to balance covariates between groups (Supplementary Table 3). Even after matching, women in higher ABSI quartiles continued to show a significantly increased risk of infertility (P < 0.05). Finally, in a subset of women aged 20–45 years, weighted multivariable regression analysis demonstrated that the risk of infertility increased with higher ABSI (OR = 1.82, 95% CI: 1.34–2.48, P < 0.001) (Supplementary Tables 4 and 5). These findings collectively reinforce ABSI as a reliable and independent predictor of infertility risk.
Discussion
This study is the first to investigate the relationship between A Body Shape Index (ABSI) and female infertility using NHANES data. Our results indicate that higher ABSI is associated with an increased risk of female infertility, as demonstrated by weighted multivariable logistic regression analysis and trend tests. The RCS curves reveal a linear positive correlation between ABSI and infertility risk. Subgroup and sensitivity analyses further confirm the robustness of these findings, supporting the potential of ABSI as a risk predictor for female infertility.
Our study is the first to describe the association between ABSI and female infertility, further supporting the link between visceral obesity and an increased risk of infertility. We found that participants with higher ABSI scores exhibited several characteristics, including older age [14, 25], lower poverty-income ratio (PIR) [25, 26], lower education levels [27], higher smoking rates [28, 29], and a higher prevalence of hypertension and diabetes [30,31,32]. These findings are consistent with other studies on abdominal obesity. Additionally, a higher proportion of White and Mexican American women were in the higher ABSI quartiles, possibly due to racial susceptibility. The literature supports the association between these characteristics and infertility risk, as advanced age [33, 34] and metabolic disorders like hypertension and diabetes [35,36,37] are recognized as high-risk factors for female infertility. Furthermore, limited access to healthcare, often linked to poverty and low education levels, increases the difficulty in managing infertility, thereby raising the risk [38, 39]. Unhealthy lifestyle choices, such as smoking, are also associated with infertility [40, 41], which our study further corroborates. However, while these risk factors aligned with higher ABSI scores, the relationship between these factors and infertility did not consistently align in our study, particularly with alcohol consumption. This suggests that more complex interactions may need to be considered when interpreting the relationship between ABSI and infertility.
Weighted multivariable logistic regression analysis indicates that high ABSI is an independent risk factor for female infertility, whether ABSI is treated as a continuous variable or divided into quartiles. The RCS analysis reveals a significant positive linear relationship between ABSI and female infertility, with a marked increase in risk when ABSI exceeds 0.079. This threshold is clinically significant, suggesting that early intervention in women with high ABSI may effectively reduce infertility risk. Subgroup and sensitivity analyses further demonstrate the robustness of these results, validating ABSI’s potential as a predictor of infertility risk.
Although several studies have explored the association between visceral obesity and female infertility [5, 6], our research highlights the potential of ABSI as a predictive tool for female infertility and emphasizes its unique clinical application value. Compared to other visceral obesity indices such as VAI, ABSI maintains accuracy while offering non-invasiveness and ease of acquisition, making it particularly suitable for large-scale screening initiatives. Current research indicates that visceral obesity is closely related to various metabolic syndromes and more directly impacts female reproductive health than general obesity, through mechanisms such as insulin resistance, chronic inflammation, and hormonal imbalances [42,43,44]. Abnormal vascularization of adipose tissue often leads to local hypoxia, triggering insulin resistance—an important mechanism in the development of polycystic ovary syndrome (PCOS) [45,46,47,48]. PCOS is one of the most common causes of female infertility [49,50,51]. In PCOS patients, abnormal fat distribution leads to reduced quality of oocytes and the endometrium, significantly impairing fertility [52, 53]. Insulin resistance may also increase insulin and insulin-like growth factor-1 (IGF-1) levels, which excessively stimulate androgen production, disrupting normal follicle development and ovulation processes [54]. Additionally, the accumulation of visceral fat triggers systemic chronic low-grade inflammation, increasing the release of pro-inflammatory cytokines such as TNF-α and IL-6. These cytokines not only disrupt the microenvironment of the endometrium but also impair ovarian function, ultimately affecting embryo implantation and pregnancy outcomes [55, 56]. Simultaneously, the increase in visceral fat often accompanies elevated estrogen levels, which further disrupt menstrual cycles and ovulation, thereby diminishing fertility [57]. This study provides new evidence supporting the use of ABSI in screening applications for women’s reproductive health, highlighting its potential in the early identification of high-risk individuals. However, further research is needed to fully understand the specific relationship between ABSI and infertility. In particular, there is currently a lack of strong evidence to suggest that weight loss can effectively improve endometrial quality and reproductive outcomes in PCOS patients.
This study has several strengths, including the use of nationally representative samples and the application of multiple statistical methods to validate the robustness of the results. However, there are also limitations. First, the cross-sectional design of the study cannot establish causality between ABSI and female infertility. Second, the diagnosis of infertility in NHANES is based on self-reports rather than a clinical gold standard, which may introduce information and recall biases. Additionally, despite adjusting for multiple covariates, unmeasured confounding factors may still influence the results. Therefore, future research should consider longitudinal designs to further verify the causal relationship between ABSI and female infertility and explore deeper biological mechanisms.
Conclusions
This study demonstrates a significant positive association between ABSI and female infertility, suggesting that ABSI, as a non-invasive indicator of visceral fat, holds potential value in identifying women at high risk for infertility. Incorporating ABSI into large-scale screening programs could aid in the early identification of high-risk individuals, thereby enabling timely interventions that may enhance reproductive outcomes and overall health.
Data availability
The datasets generated and/or analyzed during this study can be accessed in the NHANES repository at www.cdc.gov/nchs/nhanes.
Abbreviations
- ABSI:
-
A Body Shape Index
- WHR:
-
Waist-to-Hip Ratio
- VAI:
-
Visceral Adiposity Index
- NHANES:
-
National Health and Nutrition Examination Survey
- RCS:
-
Restricted Cubic Splines
- BMI:
-
Body Mass Index
- PIR:
-
Poverty Income Ratios
- CI:
-
Condence Interval
- OR:
-
Odds Ratio
- SE:
-
Standard Error
- PSM:
-
Propensity Score Matching
- NCHS:
-
National Centre for Health Statistics
References
Yang C, Dong N, Li F, Ji Y, Pan Y, She H. The cumulative live birth rate of recombinant follicle-stimulating hormone alfa verse urinary human follicle-stimulating hormone for ovarian stimulation in assisted reproductive technology cycles. J Ovarian Res. 2022;15:74.
Huo P, Zhu Y, Liang C, Yao J, Le J, Qin L, et al. Non-invasive amino acid profiling of embryo culture medium using HPLC correlates with embryo implantation potential in women undergoing in vitro fertilization. Front Physiol. 2020;11:405.
Wang R, Feng Y, Chen J, Chen Y, Ma F. Association between polyunsaturated fatty acid intake and infertility among American women aged 20–44 years. Front Public Health. 2022;10:938343.
Schon SB, Cabre HE, Redman LM. The impact of obesity on reproductive health and metabolism in reproductive-age females. Fertil Steril. 2024;122(2):194–203.
Deng C, Ke X, Lin L, Fan Y, Li C. Association between indicators of visceral lipid accumulation and infertility: a cross-sectional study based on U.S. women. Lipids Health Dis. 2024;23:186.
Zhuang J, Wang Y, Wang S, Hu R, Wu Y. Association between visceral adiposity index and infertility in reproductive-aged women in the United States. Sci Rep. 2024;14:14230.
Song J, Chen X, Jiang Y, Mi J, Zhang Y, Zhao Y, et al. Association and Interaction Analysis of Lipid Accumulation Product with impaired fasting glucose risk: a cross-sectional survey. J Diabetes Res. 2019;2019:9014698.
Zhou J, Ren Y, Wang C, Li L, Zhang L, Wang B, et al. Association of change in waist circumference and dyslipidaemia risk: the rural Chinese cohort study. Diabetes Metabolism Res. 2018;34(1):e2949.
Zhao L, Zhu C, Chen Y, Chen C, Cheng J, Xia F, et al. LH/FSH ratio is Associated with visceral adipose dysfunction in Chinese women older than 55. Front Endocrinol (Lausanne). 2018;9:419.
Ratajczak M, Skrypnik D, Bogdański P, Mądry E, Walkowiak J, Szulińska M, et al. Effects of endurance and endurance–strength training on endothelial function in women with obesity: a Randomized Trial. Int J Environ Res Public Health. 2019;16(21):4291.
Leone A, Vizzuso S, Brambilla P, Mameli C, Ravella S, De Amicis R, et al. Evaluation of Different Adiposity Indices and Association with metabolic syndrome risk in obese children: is there a winner? Int J Mol Sci. 2020;21(11):4083.
Cho HW, Chung W, Moon S, Ryu OH, Kim MK, Kang JG. Effect of Sarcopenia and body shape on Cardiovascular Disease according to obesity phenotypes. Diabetes Metab J. 2021;45(2):209–18.
Zhang X, Ye R, Sun L, Liu X, Wang S, Meng Q, et al. Relationship between novel anthropometric indices and the incidence of hypertension in Chinese individuals: a prospective cohort study based on the CHNS from 1993 to 2015. BMC Public Health. 2023;23:436.
Qiao YS, Tang X, Chai YH, Gong HJ, Zhang X, Stehouwer CDA, et al. Association of Sarcopenia and a body shape index with overall and cause-specific mortality. Front Endocrinol (Lausanne). 2022;13:839074.
Lee DH, Keum N, Hu FB, Orav EJ, Rimm EB, Willett WC, et al. Comparison of the association of predicted fat mass, body mass index, and other obesity indicators with type 2 diabetes risk: two large prospective studies in US men and women. Eur J Epidemiol. 2018;33(11):1113–23.
Li J, Sun J, Zhang Y, Zhang B, Zhou L. Association between weight-adjusted-waist index and cognitive decline in US elderly participants. Front Nutr. 2024;11:1390282.
Zhang Y, Zhang P, Yin D. Association between a body shape index and cognitive impairment among US older adults from a cross-sectional survey of the NHANES 2011–2014. Lipids Health Dis. 2024;23:169.
Nagayama D, Watanabe Y, Yamaguchi T, Suzuki K, Saiki A, Fujishiro K, et al. Issue of Waist circumference for the diagnosis of metabolic syndrome regarding arterial stiffness: possible utility of a body shape index in Middle-aged nonobese Japanese urban residents receiving Health Screening. Obes Facts. 2022;15(2):160–9.
Gradidge PJ, Norris SA, Crowther NJ. The effect of obesity on the Waist circumference cut-point used for the diagnosis of the metabolic syndrome in African women: results from the SWEET study. Int J Environ Res Public Health. 2022;19(16):10250.
Sun X, Cao L, Liu Y, Huang W, Pei C, Wang X, et al. Sex- and age-specific differences in associations of a body shape index with all-cause and cardiovascular death risks among US adults with diabetes. Nutr Metab Cardiovasc Dis. 2023;33(3):551–559. https://www.nmcd-journal.com/article/S0939-4753(22)00454-9/abstract.
Zhang Y, Gao W, Li B, Liu Y, Chen K, Wang A, et al. The association between a body shape index and elevated urinary albumin–creatinine ratio in Chinese community adults. Front Endocrinol (Lausanne). 2022;13:955241.
Gomez-Peralta F, Abreu C, Cruz-Bravo M, Alcarria E, Gutierrez-Buey G, Krakauer NY, et al. Relationship between a body shape index (ABSI) and body composition in obese patients with type 2 diabetes. Diabetol Metab Syndr. 2018;10:21.
Adamczyk M, Wender-Ozegowska E, Kedzia M. Epigenetic factors in Eutopic Endometrium in Women with endometriosis and Infertility. Int J Mol Sci. 2022;23(7):3804.
Alves MG, Martins AD, Cavaco JE, Socorro S, Oliveira PF. Diabetes, insulin-mediated glucose metabolism and Sertoli/blood-testis barrier function. Tissue Barriers. 2013;1(2):e23992.
Tang R, Fan Y, Luo M, Zhang D, Xie Z, Huang F, et al. General and Central Obesity Are Associated with increased severity of the VMS and sexual symptoms of Menopause among Chinese women: a longitudinal study. Front Endocrinol (Lausanne). 2022;13:814872.
Zare H, Meyerson NS, Nwankwo CA, Thorpe RJ. How Income and Income Inequality Drive depressive symptoms in U.S. adults, does sex matter: 2005–2016. Int J Environ Res Public Health. 2022;19(10):6227.
Alves RFS, Faerstein E. Educational inequality in the occurrence of abdominal obesity: Pró-Saúde Study. Rev Saude Publica. 2015;49:65.
de Oliveira Fontes Gasperin L, Neuberger M, Tichy A, Moshammer H. Cross-sectional association between cigarette smoking and abdominal obesity among Austrian bank employees. BMJ Open. 2014;4(7):e004899.
Liu T, David SP, Tyndale RF, Wang H, Yu XQ, Chen W, et al. Relationship between amounts of daily cigarette consumption and abdominal obesity moderated by CYP2A6 genotypes in Chinese Male current smokers. Ann Behav Med. 2012;43(2):253–61.
Bawadi H, Abouwatfa M, Alsaeed S, Kerkadi A, Shi Z. Body shape index is a stronger predictor of diabetes. Nutrients. 2019;11(5):1018.
Wang F, Chen Y, Chang Y, Sun G, Sun Y. New anthropometric indices or old ones: which perform better in estimating cardiovascular risks in Chinese adults. BMC Cardiovasc Disord. 2018;18:14.
Preuss HG. Bean Amylase inhibitor and other Carbohydrate absorption blockers: effects on Diabesity and General Health. J Am Coll Nutr. 2009;28(3):266–76.
Farnezi HCM, Goulart ACX, dos Santos A, Ramos MG, Penna MLF. Three-parent babies: mitochondrial replacement therapies. JBRA Assist Reprod. 2020;24(2):189–96.
Langarizadeh M, Nadjarzadeh A, Maghsoudi B, Fatemi Aghda SA. The nutritional content required to design an educational application for infertile women. BMC Womens Health. 2023;23:22.
Skåra KH, Hernáez Á, Næss Ø, Fraser A, Lawlor DA, Burgess S, et al. Cardiovascular disease risk factors and infertility: multivariable analyses and one-sample mendelian randomization analyses in the Trøndelag Health Study. Hum Reprod Open. 2024;2024(3):hoae033.
Zaimi M, Michalopoulou O, Stefanaki K, Kazakou P, Vasileiou V, Psaltopoulou T, et al. Gonadal dysfunction in women with diabetes mellitus. Endocrine. 2024;85(2):461–72.
Lei R, Chen S, Li W. Advances in the study of the correlation between insulin resistance and infertility. Front Endocrinol (Lausanne). 2024;15:1288326.
Thakker S, Persily J, Voigt P, Blakemore J, Licciardi F, Najari BB. Evaluating the unevaluated: a secondary analysis of the National Survey for Family Growth (NSFG) examining infertile women who did not access care. J Assist Reprod Genet. 2021;38(5):1071–6.
Nyamhanga T, Frumence G, Simba D. Prevention of mother to child transmission of HIV in Tanzania: assessing gender mainstreaming on paper and in practice. Health Policy Plan. 2017;32(Suppl 5):v22–30.
Park SR, Kim SK, Kim SR, Yu WJ, Lee SJ, Lee HY. Effects of smoking on the tissue regeneration-associated functions of human endometrial stem cells via a novel target gene SERPINB2. Stem Cell Res Ther. 2022;13:404.
Grodstein F, Goldman MB, Cramer DW. Infertility in women and moderate alcohol use. Am J Public Health. 1994;84(9):1429–32.
Diamanti-Kandarakis E. Role of obesity and adiposity in polycystic ovary syndrome. Int J Obes. 2007;31(2):S8–13.
Sato F, Nishi M, Kudo R, Miyake H. Body Fat distribution and Uterine Leiomyomas. J Epidemiol. 1998;8(3):176–80.
Venkatesh SS, Ferreira T, Benonisdottir S, Rahmioglu N, Becker CM, Granne I, et al. Obesity and risk of female reproductive conditions: a mendelian randomisation study. PLoS Med. 2022;19(2):e1003679.
Cifarelli V, Beeman SC, Smith GI, Yoshino J, Morozov D, Beals JW et al. Decreased adipose tissue oxygenation associates with insulin resistance in individuals with obesity. J Clin Invest 130(12):6688–99.
Bednarz K, Kowalczyk K, Cwynar M, Czapla D, Czarkowski W, Kmita D, et al. The role of Glp-1 receptor agonists in insulin resistance with concomitant obesity treatment in polycystic ovary syndrome. Int J Mol Sci. 2022;23(8):4334.
Escobar-Morreale HF, Martínez-García MÁ, Insenser M, Cañellas N, Correig X, Luque-Ramírez M. Serum metabolomics profiling by Proton nuclear magnetic resonance spectroscopy reveals sexual dimorphism and masculinization of intermediate metabolism in women with polycystic ovary syndrome (PCOS). Biol Sex Differ. 2023;14:21.
Ramanjaneya M, Jerobin J, Bettahi I, Bensila M, Aye M, Siveen KS, et al. Lipids and insulin regulate mitochondrial-derived peptide (MOTS‐c) in PCOS and healthy subjects. Clin Endocrinol. 2019;91(2):278–87.
Bourgneuf C, Bailbé D, Lamazière A, Dupont C, Moldes M, Farabos D, et al. The Goto-Kakizaki rat is a spontaneous prototypical rodent model of polycystic ovary syndrome. Nat Commun. 2021;12:1064.
Ezzat RS, Abdallah W, Elsayed M, Saleh HS, Abdalla W. Impact of bariatric surgery on androgen profile and ovarian volume in obese polycystic ovary syndrome patients with infertility. Saudi J Biol Sci. 2021;28(9):5048–52.
Palomba S. Is fertility reduced in ovulatory women with polycystic ovary syndrome? An opinion paper. Hum Reprod. 2021;36(9):2421–8.
Palomba S, Piltonen TT, Giudice LC. Endometrial function in women with polycystic ovary syndrome: a comprehensive review. Hum Reprod Update. 2021;27(3):584–618.
Palomba S, Daolio J, La Sala GB. Oocyte competence in women with polycystic ovary syndrome. Trends Endocrinol Metabolism. 2017;28(3):186–98.
Xing C, Zhao H, Zhang J, He B. Effect of metformin versus metformin plus liraglutide on gonadal and metabolic profiles in overweight patients with polycystic ovary syndrome. Front Endocrinol (Lausanne). 2022;13:945609.
Nair S, Nguyen H, Salama S, Al-Hendy A. Obesity and the Endometrium: Adipocyte-secreted proinflammatory TNFα cytokine enhances the proliferation of human endometrial glandular cells. Obstet Gynecol Int. 2013;2013:368543.
Yildirim G, Attar R, Ficicioglu C, Karateke A, Ozkan F, Yesildaglar N. Etanercept causes regression of endometriotic implants in a rat model. Arch Gynecol Obstet. 2010;283(6):1297–302.
Pérez-Martín AR, Castro-Eguiluz D, Cetina-Pérez L, Velasco-Torres Y, Bahena-González A, Montes-Servín E, et al. Impact of metabolic syndrome on the risk of endometrial cancer and the role of lifestyle in prevention. Bosn J Basic Med Sci. 2022;22(4):499–510.
Acknowledgements
The authors gratefully acknowledge all participants and staff of the National Health and Nutrition Examination Survey, along with the National Center for Environmental Health, for their invaluable contributions. Special thanks to Zhang Jing for developing the nhanesR package.
Funding
This research was funded by the Basic Research and Basic Applied Research Foundation of Guangdong (2023A1515140116); Shunde Hospital, Southern Medical University (SRSP2023021); the Medical Scientific Research Foundation of Guangdong Province, China (No. A2020527); and the Development Center for Medical Science & Technology, National Health Commission of the People’s Republic of China (WKZX2024DN0172).
Author information
Authors and Affiliations
Contributions
Q. Yang and J.X. Wuliu: Conceptualization, data curation, validation, visualization, and writing – original draft. L.L. Zeng and J.F. Huang: Investigation and validation. G.H. Tang and J.C. Zhang: Validation and visualization. K.D. Liao and K.X. Deng: Supervision, funding acquisition, and writing – review & editing. All authors have reviewed and approved the final manuscript and agreed to the author order.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study followed the guidelines of the Declaration of Helsinki and received approval from the NCHS Ethics Review Board. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, Q., Wuliu, J., Zeng, L. et al. Association between a body shape index and female infertility: a cross-sectional study. BMC Women's Health 24, 486 (2024). https://doi.org/10.1186/s12905-024-03335-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03335-1