
Abstract
Background
The main task of dental schools is to prepare professional dentists with a high social responsibility. This study provided some practical suggestions from experts regarding desirable clinical settings, in order to establish an infrastructure for practical studies in Endodontics, Periodontics, Oral and Maxillofacial Surgery, Restorative Dentistry, Pediatric Dentistry, Oral and Maxillofacial Medicine, Prosthodontics, Oral Health, and Social Dentistry.
Methods
This research was conducted using a modified Delphi technique in two rounds. The first round involved qualitative content analysis. Participants in interviews were selected purposeful and maximum diversity across the country. To determine the validity and reliability of the data, the four axes proposed by Lichon and Guba were utilized. The second round involved a researcher-made questionnaire, which consisted of 55 questions. This questionnaire was distributed to all dental schools across the country. The validity of the questionnaire were evaluated and by experts and then reviewed. The reliability of the tool was determined to be 0.96 using the alpha coefficient method.
Results
The final codes from the interviews of the first round were divided into two categories: settings and educational programs. The final results of research were placed into 2 section: educational settings and instructors, and educational infrastructures. 70% participants agreed to use the college’s clinical morning sessions. More than 80% agreed to start up a main clinic with the proposed structure and professors. The use of the hospitalization area also had an agreement of more than 80%. Additionally, community areas such as health service centers, welfare centers, special patient centers, factories, schools, etc. obtained an agreement of over 70%.
Conclusions
The results of this study are presented in the form of suggestions for improving the general dentistry program in relation to educational setting, educators, and educational infrastructures. The common agreement among participants regarding educational settings and their diversity, educational programs, and desired instructors reviewed in the research shows the necessity of reviewing and changing their educational programs in Endodontics, Periodontics, Oral and Maxillofacial Surgery, Restorative Dentistry, Pediatric Dentistry, Oral and Maxillofacial Medicine, Prosthodontics, Oral Health, and Social Dentistry.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Dentistry is one of the important fields of medical science, in which studying is associated with the acquisition of high scientific and professional skills. Due to the large volume of practical units and the wide range of learning skills, providing high-quality services in this field requires special attention. The main goal of dental schools is to prepare professional dentists who have a high sense of social responsibility, are familiar with the culture of the community they serve, and are capable of providing services to the target population [1]. However, by primarily focusing on traditional education methods and not providing opportunities for students to work in community centers and gain experience with fellow dentists and healthcare workers, the opportunity to care for patients or provide services is limited [2]. In Iran, the clinical course for students in the general dentistry program includes an integral treatment block with support, educational-administrative, and treatment areas (dental cabin and imaging cabin). It is expected that during training hours, this block will function as an integral treatment center and during non-administrative hours, it will function as a specialized dental center of the faculty [3]. However, in the current situation, clinical training for learners is conducted in separate specialized departments, and only a small number of faculties use other areas such as university-affiliated clinics, schools, or hospitals as learning environments.
Judian et al.’s study [4] revealed that from students’ perspectives, the educational environment and its supervision are among the factors that influence the quality of clinical education. Another study [5] found that the separation of treatment units, the provision of treatment plans by instructors, and the lack of a defined role for students are among the reasons why students lack the ability to make treatment decisions. Moreover, the separate arrangement of courses weakens students’ education.
Mathieson mentions that in the training program of the Arizona School of Dentistry and Oral Health, in the integrated community service partnership (ICSP), half of the clinical rotations are done outside of the school and the other half is planned in the main school [1]. Smith et al., by implementing a similar program to the Arizona model, showed that 73% of cases involved amalgam, 59% involved composites, 11% involved crowns, 20% involved root canal treatments, 30% involved endodontics, and 68% involved dental extractions in the community clinic [6].
The program of general dentistry should promote students to achieve all educational goals and aspects of clinical skills, based on community needs. In the universal of dental standards have also been mentioned [1]. Cardall quoted research regarding the need to revise and redesign the study course and educational programs of dental areas with the aim of improving the performance of dentists. His study showed that, according to students from various faculties in the United States, clinical experiences and patient management are the most important factors in dental education. These factors are less realized in dental school clinics than in community clinical areas [7].
The need for reviewing and upgrading educational programs and settings has been shown in a number of studies conducted in Iran. One study, related to the response of academic staff members in educational clinics, showed a low average importance given to the subject of student education and attention to all students in conveying material from the student’s perspective [8]. Another study, focusing on the quality of clinical education from the student’s perspective in four areas - professor’s knowledge and performance, clinical facilities, the behavior of faculty and staff, and overall student satisfaction - revealed a low overall satisfaction in the departments of endodontics, removable prosthesis, and fixed prosthesis, while the department of pediatric dentistry and periodontics had the highest level of satisfaction [9]. In yet another study, which evaluated the quality of clinical education from the students’ perspective, educational goals and programs were ranked third, teaching and learning ranked second, and the endodontics department received the lowest score for the educational environment, while surgery had the highest score [10]. Another study, focusing on students’ views on their learning environment, found that the lowest score was related to the appropriateness of educational activities with educational goals [11]. In a study evaluating the evaluation methods of clinical courses from students’ perspective, the methods were rated as average [12]. Additionally, a study showed a negative correlation between students’ satisfaction levels with clinical departments and their grade point average, particularly in restorative, endodontics, pediatric, and community-oriented departments [13]. The existence of a negative gap between the current and desired situation in clinical education will pose an obstacle for their future careers.
Aim
The aim of this study is to provide practical suggestions from view of experts in general dentistry for desired clinical settings, instructors, and the creation of educational infrastructure for practical courses in Endodontics, Periodontics, Oral and Maxillofacial Surgery, Restorative Dentistry, Pediatric Dentistry, Oral and Maxillofacial Medicine, Prosthodontics, Oral Health, and Social Dentistry.
Methods
Study design and settings
This research was conducted using a modified Delphi methods in two rounds [14, 15]. The first round involved qualitative content analysis, while the second round involved sending an electronic file of the questionnaire. The research was conducted in dental schools throughout the country (Iran) in 2020 to 2022.
Study participants and sampling
The participants of the first round include dean and education deputies of dentistry school and manager of departments with at least one year of executive experience, academic staff members with executive experience, preferably from 8 specialized departments: endodontics, restorative, prosthetics, pediatrics, oral and maxillofacial surgery, periodontics, oral and maxillofacial medicine, and oral health and social dentistry, as well as first-year postgraduate residents. Participants were purposefully selected. To achieve maximum diversity [16] in ideas and opinions, our contributors were selected from dental schools across the country. The participants of the second round included the participants from the first round, as well as managers and faculty members of the studied fields in all dental schools across the country, according to the census method.
Data collection tools and technique
Round one of delphi
Data collection was conducted through focus groups, face-to-face interviews, and telephone interviews. Initially, participants were contacted and provided with explanations about the research and its objectives in order to obtain their consent to participate in the study. Agreements were then made regarding the time and location of the interviews. Two focus group discussions, one with heads and one with residents, were conducted face-to-face. Additionally, 12 interviews were conducted over the telephone to gather additional information. Informed consent was obtained at the beginning of each session, with explanations given about the preservation of personal information and the permission to record the interview process. The interviews lasted between 45 and 100 min and were tailored to the interviewee’s field. They began with a general question, “Please tell us the strengths and weaknesses of the current situation in the clinical settings of practical courses in endodontics, periodontics, oral and maxillofacial surgery, restorative dentistry, pediatric dentistry, oral and maxillofacial medicine, prosthetics, oral health, and social dentistry?” Follow-up questions were also asked. All interviews were recorded and transcribed, with each session and participant assigned a code. The sampling continued until theoretical saturation was reached [17, 18]. An inductive approach was used for qualitative content analysis [19, 20]. After data generation, the analysis process began. The text of each interview was fully implemented and read multiple times until data saturation occurred and semantic units were extracted. Next, the semantic units were summarized and compressed to obtain compressed semantic units that retained the same meaning but were shorter in terms of word count. These compressed semantic units were then converted into codes with labels of the same meaning. The codes from each interview were cross-compared, and similarities and differences were identified. They were then categorized into sub-theme groups. These sub-themes were constantly compared and revised throughout the process, with some being merged or separated based on common or different characteristics to form new sub-themes. In the final stage, sub-themes with common properties were merged and given a common theme name [21]. A total of 392 codes were obtained from the interviews in this research. After merging similar codes and removing duplicates, a final count of 293 codes was obtained. To ensure the validity and strength of the data, the four axes of credibility, transferability, dependability, and conformability suggested by Lincoln and Guba were utilized [22].
Round two of delphi
After using the results of the first stage and reviewing the literature, the second round of the Delphi questionnaire was designed. This questionnaire had two parts: demographic information and questions. The questions section included 55 questions in 4 main categories, including conditions of educational settings, variety of educational settings, educational programs, and instructors. The section on the conditions of educational settings had 8 general questions including 20 items. The diversity section of the educational settings had 15 general questions related to the settings of courses examined in the research. The section on educational programs had 23 questions to determine the effectiveness and impact of the stated items in acquiring the expected competencies of students to work in the real environment and improve their performance. The teachers’ section had 9 general questions and included 56 items regarding the members of the teaching team, incentives, and criteria for being in the teaching team for the training of the students of the general dentistry course with a suitable scale. With the aim of confirming validity, the questionnaire was evaluated by experts in the field in terms of the relationship between the items and the research topic and the complete coverage of the research concepts. After review, it was approved. The reliability of the instrument was 0.96 using the alpha coefficient method with an emphasis on internal consistency.
Then the questionnaires were sent to the email addresses of the participants. In order to attract participation, reminders were sent to the respondents in two stages. Also, paper questionnaires were provided to some participants. A total of 130 participants from all over the country responded. In order to check the agreement, the data analysis of the questionnaires was done with the help of SPSS 23 software. Agreement or non-agreement on the items was based on obtaining a frequency of 70% or more in the responses. In such a way that obtaining 70% agreement for positive answers led to the acceptance of the said item as a desirable situation, and with 70% agreement in negative answers, that item was discarded.
A guideline was developed based on the results obtained in the first and second rounds of Delphi. The guide was then reviewed by experts in the field and finalized after implementing suggestions. In this guide, getting 70% or more agreement on the acceptance of educational settings, educational programs, and instructors is considered a strong proposal, and 40–69% agreement is considered a useful proposal.
Ethical consideration and approval
The present research has been approved by the National Center for Medical Education Research of the Ministry of Health and Medical Education (NASR) with ethical code IR.NASRME.REC.1400.207. The anonymity and confidentially of the participants were preserved in every phase. The participants were made fully aware of the nature and purpose of the research, an informed consent form was obtained, and the interviews were recorded.
Results
Round one
The number of participants was 33 individuals. The participants in the focus group were 11 managers and professors. Individual interviews were conducted with 12 participants, and there were 10 individuals in the focus group of first-year residents. The executive positions of the participants included 1 head of the faculty, 2 faculty educational assistants, 8 department managers, 3 department educational assistants, and 1 person responsible for the Educational Development Office (EDO). The scientific rank of the participants included 11 titular professors, 6 associate professors, and 6 assistant professors. Postgraduate residents were from 7 different dental schools, who were studying in 5 fields of specialty investigated in the research. The results of this round were divided into two categories: educational areas and programs, and instructors. The fields and educational programs included 6 main themes. The first theme was the morning clinic, and the special evening clinic of the faculty had 2 sub-themes: the time of implementation and the method of implementation of the program. The second theme was the main clinic with the sub-themes of general program design, the structure of the main clinic, and the educational program of the main clinic. The third theme of fields was hospitals with 2 sub-themes: challenges and opportunities, and the development of the learning situation. The next theme was the community clinics, which had 2 sub-themes. In the sub-theme of health centers and clinics of the treatment deputy, 2 additional sub-themes of the execution program time and development of the learning situation were placed. The next sub-theme of other fields included schools, welfare, associations for special patients, homes for the elderly, factories, barracks, etc., which included 2 sub-themes: the program execution time and the development of learning situations. The multi-day camps were the fifth theme, which included 2 sub-themes: program implementation time and program implementation method. The dental office was the last theme of the field and educational programs. The category of instructors included 3 main themes. The first theme was academic and non-academic instructors with 6 sub-themes: academic staff and educational duties, the role of faculty lecturers in the main clinic, non-academic specialists and the main clinic, academic faculty lecturers and instructors in the hospital setting, faculty instructors and education in the community, and faculty members and incentives. The next theme was postgraduate residents, and the third theme was general dentists with sub-themes that contained the role of general dentists in main clinic education, the role of general dentists in the education of the community, the selection criteria for general dentists, and the material and non-material incentives of general dentists.
Round two
The number of participants in the second round of Delphi was 130 managers and faculty members of dental schools from all over the country. The academic rank of the respondents was 72.2% assistant professor, 15.1% associate professor, and 12.7% professor. 24% (24%) of the respondents had less than 5 years of work experience, 38% had 5–10 years of experience, and 38% had more than 10 years of experience. In terms of executive experience, 15.4% of the respondents had less than one year, 45.2% had an executive experience of 1–5 years, and 39.4% had an experience of more than 5 years. The final results of the second round of Delphi were described in the form of an operational guideline by providing suggestions at two strong and useful levels, in two areas: educational setting and instructors, and educational infrastructures for the integral treatment course (internship) for 8 specialized departments, including endodontics, restorative, prosthetics, children, oral surgery and Maxillofacial, periodontics, oral and maxillofacial medicine, and oral health and social dentistry of the general dentistry course. The results are shown in Tables 1 and 2.
To visualize the distribution of clinical settings from Table 1; Fig. 1 presents the data in a categorical format. The figure reveals that medical clinics are the most frequent setting (highest number), while dental offices are the least frequent (lowest number).

categorical filed information clinical setting
Building on the data in Table 1; Fig. 2 utilizes cluster bar charts to represent the average frequency (as a percentage) of agreement levels across different clinical settings. The chart reveals that main clinics and community clinics have the highest percentage of agreements categorized as “strong suggestion,” while dental offices have the lowest percentage.

Cluster bar mean of frequency percentage by clinical setting and agreement level
Figure 3 utilizes a boxplot to illustrate the distribution of frequency percentages across clinical settings, based on the data in Table 1. The black line in the boxplot represents the median, and the dashed line indicates the mean percentage for each setting. Interestingly, medical clinics and hospital inpatient settings have higher median and mean values compared to other settings. The boxplot also allows us to analyze the variability within each setting. The interquartile range (IQR), represented by the length of the box, shows that medical clinics have the most dispersed data (widest box), indicating a wider range of frequency values. Conversely, dental offices have the least dispersed data (smallest box), suggesting a more consistent frequency distribution.

Boxplot of frequency percentage by clinical setting
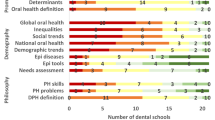
Figure 4 leverages a bar chart to represent the distribution of agreement levels across training programs, based on the data in Table 2. within a specific training program, the figure reveals that curriculum improvement and curriculum management programs have similar overall frequencies (represented by the height of the bars) and these frequencies are higher than the Educational Content Improvement program.

count - training programs bar chart by agreement level
Building on the data from Table 2; Fig. 5 presents a boxplot analysis of frequency percentages across different training programs. The analysis reveals that the “current improvement” program has the highest median frequency compared to other programs. This suggests that a larger portion of participants reported higher frequencies within this program. The interquartile range (IQR), shown by the length of the boxes, indicates that the “current improvement” program has more spread in its data (wider box). This means there’s a wider range of frequency values reported within this program. In contrast, the “educational content improvement” program has a smaller box, suggesting a more consistent distribution of frequencies.

Boxplot of frequency percentage by training programs
Discussion
Identifying the problems and obstacles in running programs and making desirable changes in the educational programs of the general dentistry course will lead to improvements in the training of specialists and, as a result, the improvement of the quality of education and the health of community. In this research, we made suggestions to improve the settings, instructors, and infrastructure of the clinical training programs of final year students of the general dentistry course.
Regarding the use of the faculty’s morning clinic for clinical students, integrated programming, at least at the level of harmonization, in rotations in endodontics, restorative, prosthetics, pediatrics, oral and maxillofacial surgery, periodontics, oral and maxillofacial medicine, and oral health and community dentistry (and other rotations if possible) is agreed upon and strongly recommended. Additionally, the use of evening clinics or clinics affiliated with the faculty was one of the useful suggestions for training students in final year. The results of the research show the importance of implementing clinical education programs in faculty clinics, at least at the level of communication between the professors of the fields and their consultation about the subjects in the curriculum planning committee under the supervision of clinical professors (Field et al.). Furthermore, a study regarding the new framework for the educational program of the general dental course cited providing continuity in the programs based on the continuum of medical education as dental education standards [23]. Perez’s study also states the importance of the faculty clinic to the community in periodontal surgery services, periodontics, implant services, and fixed and mobile prosthesis, due to the greater number of patients visited in this educational setting [24].
Rashidi et al.’s study [25] also found that, from students’ perspectives, the context dimension of the educational environment was evaluated relatively favorably, while the input, process, and output dimensions were evaluated unfavorably. This highlights the need for strategies to review and improve educational areas [26].
Examining the description of the professional duties of the graduates of the general dentistry course reveals their role as the first line of oral health and treatment, and as a result, the necessity of clinical education of students in general setting. In this study, the establishment and equipping of the main clinic setting with the aim of general training is proposed as a strong proposal. The proposed structure for the main clinic setting includes admission and triage departments, admission of emergency patients, a general department with a sufficient number of units suitable for incoming students and visitors to the faculty clinic, and a pediatric department. The recommended members of the teaching team for learners in the main clinic setting are endodontics, restorative, oral and maxillofacial surgery, periodontics, prosthodontics, oral and maxillofacial medicine, and pediatric specialists. The educational process proposed in the main clinic setting, with rotations related to the practical courses of the general dentistry course, including endodontics, restorative, periodontics, oral and maxillofacial surgery, and oral and maxillofacial medicine, is a strong suggestion. Rotations for pediatric dentistry, oral and maxillofacial medicine, prosthetics, and oral health and social dentistry were also proposed as useful suggestions. Additionally, the management of the patient by the generalist from the beginning of the visit to the main clinic, along with the presentation of the treatment plan and follow-up of the patient by the generalist under the supervision of the professor in charge of the main clinic, was a strong suggestion.
One of the advantages of setting up a main clinic setting is to provide training in real workplace. Also, the closeness to specialized departments of faculty clinics, supervision of clinical professors, and patient referral conditions lead to more complete teaching and learning for students. Mashabi, in his study, also shows a more beneficial performance of students who use both community-based and college-based education programs. Students also reported an increase in clinical skills, performing complex procedures in a shorter time, and more confidence in this training program [26]. The study of Lichtenstein et al., showed that students consider the reception service as a learning environment that improves their communication skills [27].
Regarding the existence of rotations in settings outside the faculty, studies have shown that dental education in these cases leads to the promotion of critical thinking, creating professional character, strengthening communication and interpersonal skills, promoting health, executive management and informatics, and patient care from evaluation to diagnosis, presentation of treatment plans, and oral health [28, 29].
Another strong suggestion in this research was the use of the hospital as an arena for educational rotations for oral maxillofacial medicine and surgery practical courses. Also, specialists in oral and maxillofacial medicine and specialists in oral and maxillofacial surgery were proposed as members of the training team for students in this setting. Another proposed area on which there was a strong agreement was the use of dental clinics in hospitals to perform simple procedures and community health centers to train students on preventive action, removing simple cavities, and providing health education. Also, patient management in the setting of health centers was suggested to the students with the aim of teaching the role of the family dentist. Perez et al.’s study also showed that the number of patients visited for diagnosis, prevention, procedures, oral surgery, and general services in the community clinic is more than in the college, and the students perform more effectively and completely in connection with the procedures they present under the supervision of a colleague or faculty member [24].
A study on the attitude of students towards community-based education showed that they believed that some of the limitations of treating patients in other educational departments were compensated and that the faculty groups should provide part of their education in the community setting [30].
Among the other areas of the community proposed in this research were welfare centers, clinics, special patients’ associations, factory clinics, schools, social security clinics and hospitals, and army clinics and hospitals, barracks, and prisons. These facilities can be adapted to the local conditions of the faculty while maintaining compliance with educational standards. If there is an acceptable number of patients, they should be used for educational rotations for students in their final year. Additionally, schools were proposed as educational arenas for practical oral health and social dentistry courses. Assigning the responsibility of improving oral and dental health to students from the first year of dentistry was strongly suggested in order to understand the needs of the community and improve the health and treatment of the covered population. The use of short-term mobile arenas was strongly suggested if there is equipment and an instructor approved by the faculty. Utilizing these settings, while providing exposure to more patients and working in a real workplace, will familiarize students with the needs of community and enhance their communication skills. Furlini et al., in a study related to the evaluation of dental students’ readiness, mentioned faculty clinic training programs and experiential learning in community settings such as community clinics or mobile dental clinics. In some faculties, this program takes the form of one- to two-day educational projects, while in others, students spend a week or more providing services and care for patients under the supervision of a dentist in the community. In all these models, students not only learn and gain experience regarding health and community health, but also provide services to the covered population, such as homeless people, AIDS patients, individuals with mental and physical disabilities, and the elderly. This helps balance the budget and implement the mission of the dental school [31]. Another research study also highlights the existence of many educational opportunities in health centers, non-profit community clinics, native health services clinics, army hospital units, refugee centers, prisons, and mobile dental programs [1].
Asghari et al.’s study found that approximately half of the students believed that providing healthcare services through mobile clinics was essential, and approximately 90% of them believed that community settings are an important part of dental education [30].
Among the other proposed settings, the dental offices or clinics of general dentists were to have criteria such as confirmation of scientific ability, education with scientific tests, confirmation of practical skills, and professional thinking, etc. According to the participants of this research, the use of these settings can be useful for the students of the final year in teaching communication skills, performing techniques, principles of office management, payments, and preparing tools and facilities. Mathieson et al.’s qualitative study on students’ experience from community clinics also shows benefits such as learning how to deal with anxious or scared patients, getting to know the organizational structure of the clinic and its management policies and procedures, the payment and billing system and related challenges, patients’ communication with socio-economic problems. It was establishing interaction between students, patients, instructors, and staff [1].
Regarding the creation of educational infrastructure and the improvement of the curriculum, proposals have been made for tasks such as compiling the task description for students in the final year, determining instructors and evaluation methods, forming an educational team with the appropriate number and specializations for clinical group, and providing students with the opportunity to gain experience through clinical rotations with different professors. Additionally, it has been suggested to establish a curriculum planning committee consisting of professors from the clinical course. In a study focused on formulating a new curriculum framework, it has been recommended to update and define basic competence, teaching and evaluation methods, and learning outcomes [24].
Derisavi et al.’s study on the educational environment also found the lowest scores in the areas of curriculum and the use of active teaching methods by instructors. This highlights the need to implement the proposed solutions [32].
In connection with the improvement of educational content, some strong suggestions have been presented. These include providing training related to the method of preparing and using dental tools and equipment, holding educational seminars and training related to the application of health economics in dentistry, communication skills, health economics, and familiarity with the methods of preparing dental tools and facilities. In a qualitative study related to the experiences of final year dental students, they mentioned things such as improving personal communication skills, strengthening the ability to communicate with patients, and correctly guiding the patient in the stages of diagnosis and treatment [33]. Regarding the management of the educational program, the coordination of the education, treatment, and health departments at the level of university and ministry of health, the formulation of solutions related to the legal principles to facilitate the activities of the students in the community, the revision and amendment of the dental insurance laws in traffic accidents. The aim is to give students more access to all educational cases in medical centers and educational cases related to special and cancer patients in dental treatments. It is obvious that in order to implement education in line with the educational program of the course and to achieve the expected competency of the students, it is necessary to provide the specified infrastructure.
Limitations
One of the limitations of this research was the wideness of the statistical population. To solve this problem, in the first stage, we used a telephone interview in addition to a face-to-face interview. The lack of time of the participants due to their busy schedule and executive, educational, and therapeutic responsibilities was one of the other problems for conducting this research. To solve this problem, the second rounds of questionnaires were distributed with the help of email. In order to check the effectiveness of the suggestions, researchers recommend the implementation and evaluation of the strengths and limitations of the designed program.
Conclusions
The results of the research have been presented in the form of suggestions to improve the general dentistry course program in relation to the educational setting, instructors, and educational infrastructure. Various setting includes faculty clinics, the main clinic, hospital inpatient and outpatient areas, community clinics including community health centers, welfare center clinics, special patients’ associations, factories, schools, social security and army hospitals, barracks, and prisons, short-term dental courses, mobile and dental offices with an educational program and trainers. The next part of the educational infrastructure includes curriculum improvement, educational content improvement, and curriculum management. In this section, the proposals related to the creation of infrastructure for improving and upgrading the programs have been expressed. The participants’ opinion agreement in relation to the educational setting and its diversity, the educational programs, and the desired instructors reviewed in this study show the necessity of revision and transformation in the programs being implemented in the course of integral treatment of learners in the courses of endodontic, periodontics, oral and maxillofacial surgery, restorative dentistry, pediatric dentistry, oral and maxillofacial medicine, prosthetics, and oral health and social dentistry. In order to implement the suggestions made with the aim of improving the quality of dental services at the community level, it is necessary to coordinate the relevant departments at the faculty, university, and national level. The implementation of the solutions derived from the findings of this research may vary depending on the conditions of dental schools, including human resources (faculty and staff), facilities and equipment, financial resources, and infrastructure. We suggest that, in order to improve the general dentistry program, school administrators should use the proposed solutions according to their available resources.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Mathieson KM, Gross-Panico ML, Cottam WW, Woldt JL. Critical incidents, successes, and challenges of community-based dental education. J Dent Educ. 2013;77(4):427–37.
Formicola AJ, Bailit HL. Community-based dental education: history, current status, and future. J Dent Educ. 2012;76(1):98–106.
education M. o.h.a.m. Stand Plann Des Educational Spaces 2015; 1st ed:[.
Joudyian N, Naghiazar P, Azami-Aghdash F, Mosavi S. Identification and comparison of factors affecting the quality of clinical education from the perspective of medical and dental students of Tabriz University of Medical Sciences in 2020. Educational Dev Judishapur. 2021;12:811–7.
Theile CW. Strengths and weaknesses of the current dental hygiene educational system. J Dent Educ, 2017;81(9):eS38-eS44.
Smith KP, Woldt JL, Cottam WW, Cederberg RA. The Arizona model: a new paradigm for dental schools. J Dent Educ. 2011;75(1):3–12.
Cardall WR, Rowan RC, Bay C. Dental education from the students’ perspective: curriculum and climate. J Dent Educ. 2008;72(5):600–9.
Rouhollahpour-Ahangar E, Ghaemi-Amiri M, Hosseini-Motlagh SZ, Gholamnia-Shirvani Z, Soltani M, Dentistry Faculty. Response in Dental Clinics from the perspective of students. babol-mej. 2019;7(2):34–9.
Bashardoust N, Govabar M, Mirfarhadi M. The Education Quality in each clinical departments from the perspective of Fifth- and Sixth-Year Dental students in 2020. Horizon Med Educ Dev. 2022;13(3):6–18.
Sadeghi M. Evaluation of the quality of clinical education from the viewpoint of Rafsanjan dental school students. DSME. 2022;9(3):10–8.
Tahani B. Students’ perspectives in pre-clinical and during the clinical courses in Dental School of Isfahan University of Medical Sciences in year 2016. Iran J Med Educ. 2019;19:136–45.
Ahmad Mehrabi M, Sadeghipour Roudsari M, Dalaie K, Namdari M. Shahid Beheshti dental students’ perspective on clinical course evaluation methods. Iran J Med Educ. 2020;20:103–13.
Nematollahi H, Razeei L, Khanmohammadi R, Shakib H. Evaluating success of pediatric dentistry department at Mashhad dental school in clinical skills education from student’s perspective. J Mashhad Dent School. 2013;37(3):185–200.
Keeney S, McKenna H, Hasson F. The Delphi technique in nursing and health research. 2011, Hoboken, NJ: Wiley-Blackwell. 208.
Humphrey-Murto S, et al. The use of the Delphi and other consensus group methods in medical education research: a review. Acad Med. 2017;92(10):1491–8.
Grove SK, Burns N, Gray J. The practice of nursing research: Appraisal, synthesis, and generation of evidence. Elsevier Health Sciences; 2015.
Braun V, Clark V. Successful Qualitative Research a practical guide for beginners. 2013.
Rebar C. Understanding nursing research. Lippincott Williams & Wilkins; 2011;3:424.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Zhang Y. Qualitative analysis of content. Applications of social research methods to questions in information and library science. 2016. 318.
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–12.
Lincoln YS, Guba EG. Naturalistic inquiry. New Dehli: Sage; 1985. p 416.
Field JC, Cowpe JG, Walmsley AD. The graduating European dentist: a new undergraduate curriculum framework. Eur J Dent Educ. 2017;21(S1):2–10.
Perez FA, Allareddy V, Howell H, Karimbux N. Comparison of clinical productivity of senior dental students in a dental school teaching clinic versus community externship rotations. J Dent Educ. 2010;74(10):1125–32.
Rashidi Maybodi F, Hosseini-Yekani A, Golshahi N. Assessment of Educational Status of Periodontics and oral Health and Community Dentistry Departments in Yazd Dental School using CIPP model in 2018. JSSU. 2021;29(8):4046–56. http://jssu.ssu.ac.ir/article-1-5348-en.html.
Mashabi S, Mascarenhas AK. Impact of community externships on the clinical performance of senior dental students. J Dent Educ. 2011;75(10 Suppl):S36–41.
Lichtenstein N, et al. May I help you?-Evaluation of the new student service at the reception desk during the clinical courses at the Department of Operative Dentistry and Periodontology as a part of a longitudinal curriculum of social and communicative competences for dental students. GMS Zeitschrift für Medizinische Ausbildung; 2015;32(3).
McFarland KK, Nayar P, Ojha D, Chandak A, Gupta N, Lange B. Impact of communitybased dental education on attainment of ADEA competencies: students’ self-ratings. J Dent Educ. 2016;80(6):670–6.
Piskorowski WA, Stefanac SJ, Fitzgerald M, Green TG, Krell RE. Influence of community-based dental education on dental students’ preparation and intent to treat underserved populations. J Dent Educ. 2012;76(5):534–9.
Asgari I, Aghababaei F. Assessment of belief and attitude about community-based dental education among senior students in Isfahan dental school. J Dent Med. 2020;33(3):170–80.
Furlini L, et al. Assessing dental students’ readiness to treat populations that are underserved: a scoping review. J Dent Educ. 2018;82(5):483–91.
Darisavi S, Molaei S, Yazdi NA, Paivan H. Evaluation of Educational Environment of Ardabil Dental School based on DSLES Model. J Isfahan Dent School. 2023;19(1):45–53.
Zokaee H, Pakkhesal M, Ahmadinia AR, Jouybari L. Explaining Dental Students’ experiences of Community-based education: a qualitative study through students’ reflection writings. IJME. 2019;19(0):248–55.
Acknowledgements
Our special thanks to the committed experts in medical sciences universities.
Funding
This research has been financially supported by the National Center for Medical Education Research of the Ministry of Health and Medical Education (NASR).
Author information
Authors and Affiliations
Contributions
BH and MSHJ initiated and designed the study. BH, MSHJ & Ms collected the data. MSHJ and ME analyzed and interpreted the results. MSHJ designed the tables. ME designed the figures. MSHJ wrote the original draft of the manuscript. BH, MSHJ, ME and ECH contributed to the writing and editing of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The present research has been approved by the National Center for Medical Education Research of the Ministry of Health and Medical Education (NASR) with ethical code IR.NASRME.REC.1400. 207.The anonymity and confidentially of the participants were preserved in every phase. The participants were made fully aware of the nature and purpose of the research, an informed consent form was obtained, and the interviews were recorded.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Houshmand, B., Shaterjalali, M., Chegeni, E. et al. Desirable clinical settings in general dentistry: moving towards the improvement of the educational program. BMC Med Educ 24, 966 (2024). https://doi.org/10.1186/s12909-024-05951-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05951-9