
Abstract
Background
Dipeptidyl peptidase-4 (DPP-4) inhibitors may have protective effects in the early stage of atherosclerosis in patients with type 2 diabetes, although similar effects in advanced atherosclerosis were not shown in recent randomized placebo-controlled studies. Therefore, we investigated the efficacy of DPP-4 inhibitor on endothelial function and glycemic metabolism compared with high-dose metformin.
Methods
In this multicenter, open-labeled, prospective, randomized, parallel-group comparison study, patients with type 2 diabetes treated with low-dose metformin (500–750 mg/day) were enrolled and randomly assigned to a vildagliptin, a DPP-4 inhibitor, add-on group (Vilda) or a double dose of metformin group (high Met) for 12 weeks. Flow-mediated dilation (FMD) and serum metabolic markers were assessed before and after treatment. In addition, glycemic control and metabolic parameters were also assessed.
Results
Ninety-seven subjects (aged 58.7 ± 11.0 years; body mass index, 25.9 ± 4.4 kg/m2; HbA1c, 7.3 ± 0.5%; FMD, 5.8 ± 2.6%) were enrolled. Eight subjects dropped out by the end of the study. There were no significant differences between the two groups in baseline characteristics. After 12 weeks, HbA1c was significantly improved in the Vilda group compared with the high Met group (− 0.80 ± 0.38% vs. − 0.40 ± 0.47%, respectively; p < 0.01). However, there were no significant differences in FMD (− 0.51 [− 1.08–0.06]% vs. − 0.58 [− 1.20–0.04]%). Although the apolipoprotein B/apolipoprotein A1 ratio was significantly reduced in the Vilda group compared with baseline (0.66–0.62; p < 0.01), the change did not differ significantly between the two groups (− 0.04 vs. 0.00; p = 0.27). Adiponectin levels were significantly increased in the Vilda group compared with the high Met group (0.75 μg/mL vs. 0.01 μg/mL; p < 0.01).
Conclusions
Regardless of glycemic improvement, combination therapy of vildagliptin and metformin did not affect endothelial function but may exert favorable effects on adipokine levels and lipid profile in patients with type 2 diabetes without advanced atherosclerosis.
Similar content being viewed by others

Background
The dipeptidyl-peptidase-4 (DPP-4) inhibitors reduce blood glucose levels in a glucose-dependent manner by increasing endogenous glucagon-like peptide-1 (GLP-1), and have been reported to have protective effects on pancreatic beta cells [1, 2]. Unlike some other anti-diabetic medications, they are associated with a low risk of hypoglycemia and a neutral effect on body weight [3, 4]. GLP-1 relaxes the vascular endothelium in a nitric oxide (NO)-dependent fashion [5], and short-term (105 min) native GLP-1 infusion has been reported to improve vascular endothelial function in patients with type 2 diabetes [6]. Vascular endothelial dysfunction is thought to be an early marker of arteriosclerotic progression [7]. Hence, improvement of vascular endothelial dysfunction may inhibit the progression of arteriosclerosis. In patients with diabetes, the frequency of coronary artery disease is 2–4 times than in non-diabetic patients [8], and the risk of developing cerebral infarction is approximately twofold greater [9]. Suppression of arteriosclerosis is therefore considered an important goal of diabetes treatment. Metformin suppresses macroangiopathy and is a low-cost treatment for diabetes, being recommended as the first-line treatment for type 2 diabetes in Europe and the United States [10,11,12]. However, DPP-4 inhibitors have been shown to be effective in lean type 2 diabetic patients [13], and are therefore frequently prescribed in Asia, including Japan. It remains unclear whether metformin or a DPP-4 inhibitor should be used to optimally manage the initial stage of arteriosclerosis. Although various studies describe the effects of incretin-related drugs on vascular endothelial function, we previously reported that neither sitagliptin nor liraglutide improve flow-mediated dilatation (FMD) in patients with type 2 diabetes [14, 15]. However, several reports describe different effects of DPP-4 inhibitors on FMD. Suppression of 24-h blood glucose fluctuation by vildagliptin correlated with improved oxidative stress and levels of inflammatory marker compared with sitagliptin [16]. Similar results were reported in Asian patients with type 2 diabetes [17, 18]. Based on these findings, we investigated whether addition of vildagliptin or increased metformin could improve vascular endothelial function in patients with type 2 diabetes and poor glycemic control on low-dose metformin.
Methods
Study population
Ninety-seven subjects with type 2 diabetes and well-controlled blood pressure and plasma lipids were enrolled from 13 medical service units located in Sapporo City (SAIS Study Group). The inclusion criteria were as follows: outpatients with type 2 diabetes receiving metformin (500–750 mg/day) for more than 4 weeks in addition to diet and exercise therapy, with or without sulfonylureas or glinides; age 20–75 years; and inadequate glucose control (defined as HbA1c level between 7.0 and 8.5%). We excluded patients diagnosed with atherosclerotic diseases (angina, myocardial infarction, cerebral infarction, and peripheral arterial disease), patients currently receiving insulin therapy, pregnant women, and patients with persistent elevated serum transaminase levels or renal dysfunction.
Protocol
This was a multicenter, open-labeled, prospective, randomized, parallel-group comparison study. During the study period, diet and exercise therapy were controlled as usual, and changes in dose and frequency of all medications other than vildagliptin and metformin were prohibited during the study period. However, sulfonylureas or glinides could be reduced in patients at risk of hypoglycemia. The primary endpoint of the study was the change in FMD between the treatment groups. The sample size was calculated using the assumption that combination therapy of vildagliptin and metformin or high-dose metformin would improve FMD by 1.5% (SD = 1.8%) and 0.5%, respectively, based on previous single-arm studies using sitagliptin or metformin [19,20,21,22]. It was determined that 52 patients were needed for each group to detect a significant difference with 80% power and statistical significance of 5%, assuming unequal variance between groups, based on a two-sample t test. Secondary endpoints were the changes in metabolic parameters and surrogate markers of beta cell function. After providing informed consent, patients were assigned to a vildagliptin and metformin combination therapy group (Vilda) or a high-dose metformin treatment group (high Met) by Pocock and Simon’s minimization method according to the characteristic factors of age, body mass index (BMI), HbA1c, and FMD using FileMaker Pro 11 Advanced in the allocation institution. In the Vilda group, vildagliptin (100 mg/day) was administered to patients taking metformin (500–750 mg/day). In the high Met group, the pre-study metformin dose was increased to 1000–1500 mg/day. Strict blood glucose control was performed at each respective medical care center for the 12-week study period. The primary endpoint, FMD, was analyzed at Hokkaido University Hospital before and after the trial by the same technician who was blinded to the treatment groups. In addition, assessments of glycemic control and metabolic parameters were conducted. The subject enrollment period was from April 2013 to March 2016, and the last subject completed the study in Octorber 2016.
Endothelial function
Evaluation of endothelial function was performed using FMD of the brachial artery according to published guidelines [17,18,19]. Briefly, FMD was performed in the morning after overnight fasting. From the morning of the examination day, participants refrained from medications, smoking, caffeine, and antioxidant vitamins and received only drinking water prior to FMD measurement. Patients were maintained in a supine position for at least 15 min in a quiet, temperature-controlled room (23–26 °C) before the baseline vascular diameter was measured in the brachial artery of the right arm. Five minutes after systolic compression of the right forearm (50 mmHg over the systolic blood pressure), the cuff was deflated and the vascular diameter was continuously measured. FMD was expressed as a percent change from baseline to peak expansion. Augmentation index and reactive hyperemia index (RHI) were measured using an Endo-PAT device (Itamar Medical Ltd., Cesarea, Israel). Centric systolic blood pressure (cSBP) was measured using HEM-9000AI(OMROM, Kyoto, Japan) according to the manufacturer’s instruction.
Biochemical analysis
Fasting blood samples were placed on ice immediately after collection and centrifuged at 4 °C, and the resulting supernatants were stored at −20 °C until assayed. low-density lipoprotein (LDL)-cholesterol levels were calculated using the Friedewald formula. Plasma adiponectin, high-sensitivity C-reactive protein (hs-CRP), glucagon, tumor necrosis factor alpha (TNF-α), N terminal prohormone of brain natriuretic peptide (NT-proBNP), and proinsulin were measured by latex agglutination, nephelometry, radioimmunoassay, enzyme-linked immunosorbent assay, electro-chemiluminescence immunoassay, and radioimmunoassay, respectively (SRL, Inc, Tokyo, Japan).
Evaluation of relevant factors
Evaluation of beta cell function was based on the proinsulin/insulin ratio. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated from the fasting plasma glucose and insulin levels according to the following formula: (fasting plasma glucose [mg/dl] × insulin concentration [μU/ml])/405. The levels of derivatives of reactive oxygen metabolites (d-ROM), as indicators of the production of reactive oxygen species, and biological anti-oxidant potential (BAP), as an indicator of antioxidant capacity, were measured as described previously [14, 15].
Statistical analysis
Results are shown as mean ± SD, median (range) or number (%). Differences in baseline characteristics between the two groups were evaluated using Welch’s t-test or the Mann–Whitney U test for continuous variables, and the Chi square test for category variables. The Kolmogorov–Smirnov test for normality was used to determine the appropriate statistical test for the continuous variables. The primary endpoint was analyzed based on the intention-to-treat principle. As the primary analysis, the effects of vildagliptin (Vilda) compared with the high Met group on FMD were assessed by analysis of ANOVA. In Addition, analysis of covariance (ANCOVA) was also performed to adjust for baseline FMD. Multiple imputations were used to address missing outcomes (e.g., FMD after 12 weeks). To impute the missing data, we used the predictive mean matching method, including variables potentially related to the fact that FMD was missing and also variables correlated with FMD. The number of imputations was repeated 100 times. Secondary endpoints were descriptively analyzed for mean baseline and post-treatment changes in endothelial and metabolic parameters in both groups in the complete case population. p values < 0.05 were considered statistically significant. Data were analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) for the primary analysis and Ekuseru-Toukei 2012 (Social Survey Research Information, Tokyo, Japan) for other analyses.
Results
Baseline characteristics
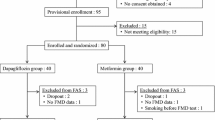
A total of 97 subjects were enrolled, but one was subsequently found not to meet the study criteria and withdrew. Of the 96 subjects who underwent the initial examination, none were excluded. Eight subjects dropped out by the end of the study. The reasons for non-completion included interruption of ambulatory visits (n = 6) and side effects of test drugs, such as diarrhea and increased serum levels of creatinine kinase (n = 2) (Fig. 1). The study group included 57 males and 39 females, with an average age of 58.7 ± 11.0 years, BMI of 25.9 ± 4.4 kg/m2, and HbA1c level of 7.3 ± 0.5%. At baseline, there were no significant differences between the two groups in age, sex, BMI, blood pressure, biological parameters, prevalence of current smoking, complications of diabetes, and proportion of renin-angiotensin system blockers, statins, and metformin (Table 1).

CONSORT flow diagram
Endothelial function and atherosclerosis
Baseline FMD was 5.48% in the Vilda group and 6.14% in the high Met group. FMD decreased in both groups after treatment, and the changes in FMD were not significantly different between the groups. The primary result did not alter even with ANCOVA adjusted for baseline FMD (p = 0.854) (Table 2). Although no clear relationship was observed between the change in FMD and HbA1c level in either group, the change of apolipoprotein (apo)B/apoA1 ratio decreased significantly in correlation with the change in FMD in the Vilda group (Table 3). Other cardiovascular parameters, such as cSBP, augmentation index, and RHI, remained unchanged (Table 4).
Glycemic control and metabolic factors
After the treatment period of 3 months, BMI was significantly decreased in the high Met group but there was no significant difference in the change in BMI between the Vilda and the high Met groups. HbA1c significantly improved in the Vilda group compared with the high Met group (p < 0.01). HOMA-IR also significantly improved in the Vilda group (p = 0.01). Serum glucagon level, TNF-α, and hsCRP were significantly reduced in the high Met group (p = 0.04, 0.02, and 0.03, respectively), and the proinsulin/insulin ratio significantly improved in both groups after treatment, although there were no significant differences between the groups. Changes in the oxidative stress parameters, d-ROM and BAP, were not observed in either group. With regard to lipid profile, LDL-cholesterol levels were reduced in both groups even though lipid-lowering agents were sustained without any modification during the study period, but there was no significant difference between the two groups. The apoB/apoA1 ratio was significantly reduced in the Vilda group at 12 weeks compared with baseline (p < 0.01), but did not significantly differ between the two groups (p = 0.27). Interestingly, adiponectin level was significantly increased in the Vilda group compared with the high Met group (0.75 μg/mL vs. 0.01 μg/mL, respectively; p < 0.01) (Table 4).
Discussion
Several reports have suggested that incretin-based agents may possess protective effects against atherosclerosis [5, 6, 23,24,25]. However, some randomized clinical trials have reported that DPP-4 inhibitors failed to reduce cardiovascular events compared with placebo in patients with type 2 diabetes [26,27,28]. The European Diabetes Association and the American Diabetes Association recommend that metformin is prescribed as a first-line drug regardless of body weight, and DPP-4 inhibitors are increasingly being used as second-line treatment as add-on to metformin [29]. In Japan, fewer patients are prescribed metformin and the daily doses are lower than in Europe and the United States, but since high-dose metformin has been covered by insurance, the number of prescriptions and the daily dosage has gradually increased. In the United Kingdom prospective diabetes study (UKPDS) 34, a significant risk reduction was observed for metformin in diabetes-related end points, all deaths, and stroke, as compared with insulin [10]. A sub-analysis of patients with diabetes in the prevention of restenosis with tranilast and its outcome (PRESTO) trial reported a significant risk reduction with metformin compared with insulin or sulphonylureas in major adverse cardiac events, myocardial infarction, and total deaths [30]. In support of these reports, improvements in vascular endothelial function [21], increased GLP-1 concentration [31], and, in mouse studies, increased GLP-1 receptors in islets [32] have been reported for metformin. Taken together, combination therapy of metformin and GLP-1 related agents appear to be clinically effective in enhancing the GLP-1 effect, with a positive influence on vascular endothelial function. However, we observed no improvement in FMD with vildagliptin or metformin over 12 weeks in our study. Although improvement of endothelial dysfunction with a single administration of vildagliptin has been reported [33], in fact the reported short-term effects of treatment with DPP-4 inhibitors on FMD have been controversial [20, 34,35,36,37,38]. Because some studies over a longer period showed that DPP-4 inhibitors have an anti-atherosclerosis effect [39,40,41], the length of the study period may be a concern. However, one study reported that adjunctive sitagliptin added to conventional antihyperglycemic drugs in patients with type 2 diabetes did not alter endothelial function evaluated by FMD during a 2-year study period [42]. Several explanations can be hypothesized regarding these conflicting results. First, DPP-4 inhibitors are multitarget compounds, and their activity is therefore connected with the inhibition of various substrates, leading to undesirable effects. Moreover, DPP-4 inhibitors may exert differential effects on substrate activity in a diabetic versus a normoglycemic setting, and chronic treatment with gliptins exerts progressive changes in metabolic parameters beyond those detected in single-dose administration studies [23]. Moreover, the results of FMD can be confounded by factors such as patients’ background [43], air temperature [44], and concomitant medications [45,46,47,48]. In this study, no significant differences were observed between the groups for any of these confounding factors. Additionally, adjusted change in FMD, which was calculated based on baseline FMD values, yielded similar results in both groups. Regarding glycemic control, HbA1c significantly improved in the Vilda group compared with the high Met group. We sought to adjust the dose of metformin to achieve HbA1c of < 7% and achieved this for the high Met group after treatment, with HbA1c of 6.8%. The hypoglycemic effect of vildagliptin was larger than expected, however, and was associated with a significant improvement in HbA1c. The Vilda group did not exert any additional beneficial effect on vascular endothelium despite a greater effect on HbA1c. Because metformin has beneficial effects on vascular endothelium [37, 49,50,51], there is a possibility that the effect of improving FMD had already been achieved by pretreatment with metformin. Moreover, because the baseline FMD in this population was similar to that of the healthy group [52], it is also possible that the improvement was difficult to obtain by treatment. Indeed, our result demonstrated a negative correlation between the baseline FMD and ΔFMD (Additional file 1: Figure S1). Systolic blood pressure in each group did not change after treatment for 12 weeks, whereas central blood pressure decreased in both groups. As central blood pressure was related to cardiovascular events rather than peripheral blood pressure [53], arteriosclerosis in both groups was beneficially affected. LDL-cholesterol is a major atherogenic lipoprotein which contributes to the development of coronary heart disease, and currently represents the primary target for lipid-lowering therapy for the prevention and treatment of cardiovascular disease [54, 55]. ApoB reflects the amount of cholesterol, (and, to some degree, triglyceride)-containing particles [56, 57]. ApoA1 is the major apolipoprotein associated with high-density lipoprotein (HDL), and is associated with several anti-atherogenic effects [58]. The apoB/apoA1 ratio is also a marker of risk for future cardiovascular disease [59]. In addition to improving lipid by improving blood glucose, it has been reported that anagliptin inhibits lipogenesis in the liver [60]. Another study showed that linagliptin for 16 weeks improved endothelial function evaluated by FMD and that this effect was mediated, at least in part, by reduction in apoB [61]. In this study, the apoB/apoA1 ratio was significantly improved and negatively correlated with the change in FMD in the Vilda group compared with baseline. Moreover, the addition of vildagliptin to metformin significantly improved serum adiponectin levels compared with high-dose metformin. As there was no clear relationship observed between the changes in HbA1c and adiponectin in both groups, the improvement of adiponectin was thought to be independent of HbA1c. Adiponectin is known to exert multifaceted effects, having anti-inflammatory, anti-arteriosclerotic, and anti-diabetic activities [62, 63]. Furthermore, treatment with sitagliptin or vildagliptin has been shown to increase adiponectin levels [14, 20, 64, 65] through a mechanism which may involve decreased oxidative stress or visceral fat [66]. Markers of oxidative stress were altered in neither group in this study. However, we did not evaluate visceral fat, so we could not confirm the potential involvement of this mechanism. In accord with decreasing ApoB/ApoA1 ratio and increasing adiponectin levels, there is a possibility that vildagliptin-induced improvement of lipid metabolism might exert a beneficial effect on cardiovascular function. Consistent with a basic scientific study demonstrating that adiponectin could have an insulin-sensitizing function [67], HOMA-IR improved in the Vilda group in which adiponectin increased. On the other hand, despite a lesser effect on HbA1c levels in the high-Met group, the high-Met group performed better on pro-inflammatory cytokines. This could be related to greater reduction of body weight in the Met group. It was also reported that metformin inhibited inflammatory cytokines by attenuating nuclear factor κB activation via AMPK activation [68], downregulating chemokine ligand 10 and tissue inhibitor of metalloproteinase 1 gene expression, and increasing vascular endothelial growth factor A [50]. It is possible that short-term combination therapy of vildagliptin and metformin has an inhibitory effect on arteriosclerosis. Recent reports show that alogliptin and sitagliptin did not improve the intima-media thickness over 12 months, but did significantly improve it following a 24-month treatment period [39, 40]. Given that centric systolic blood pressure, HOMA-IR, apoB/apoA1 ratio, and adiponectin improved following 12 weeks of treatment with vildagliptin in this study, FMD may also improve with longer vildagliptin treatment.
A major limitation of this study was the failure to enroll the target number of subjects (97 out of 104). Because of the severity of entry criteria, enrollment was not easy in three years. Future studies should thus involve a larger number of institutes, a longer study period, or a simpler protocol. There is a report that FMD was significantly reduced (worsened) by a DPP-4 inhibitor over 6 weeks [34]. Although there was no significant difference in our study over 12 weeks of treatment, given that 7 enrolled patients did not complete the study, we cannot fully rule out significant worsening of FMD by the DPP-4 inhibitor. Another potential limitation of our study was that medication use was not blinded, although the investigator who performed the FMD was unaware of the patient status and medical history. Moreover, HbA1c reduction was significantly greater in the Vilda group than in the high-Met group. This difference may have influenced some results in this study. This difference may have affected to some results in this study. Finally, the 12-week study duration may have been insufficient to assess the change in FMD or atherosclerosis, as stated in the discussion. To resolve these potential issues, our findings should be validated in a double-blind study, using a larger population over a longer period of time (Additional file 2).
Conclusions
In this study, combination therapy of vildagliptin and metformin did not further improve vascular endothelial function compared with high-dose metformin over 12 weeks. However, combination therapy improved the apoB/apoA1 ratio and increased serum adiponectin levels, suggesting that long-term combined administration of vildagliptin and metformin may have an inhibitory effect on arteriosclerosis (Additional file 3).
Abbreviations
- ANCOVA:
-
analysis of covariance
- apoA1:
-
apolipoprotein A1
- apoB:
-
apolipoprotein B
- BAP:
-
biological antioxidant potential
- BMI:
-
body mass index
- cSBP:
-
centric systolic blood pressure
- DBP:
-
diastolic blood pressure
- DPP-4:
-
dipeptidyl-peptidase-4
- d-ROMs:
-
reactive oxygen metabolites-derived compounds
- FMD:
-
flow-mediated dilation
- FPG:
-
fasting blood glucose
- GLP-1:
-
glucagon-like peptide-1
- HbA1c:
-
hemoglobin A1c
- HDL:
-
high-density lipoprotein
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- hsCRP:
-
high-sensitivity C-reactive protein
- LDL:
-
low-density lipoprotein
- NO:
-
nitric oxide
- NT-proBNP:
-
N terminal prohormone of brain natriuretic peptide
- PRESTO:
-
prevention of restenosis with tranilast and its outcome
- RHI:
-
reactive hyperemia index
- SBP:
-
systolic blood pressure
- TNF-α:
-
tumor necrosis factor alpha
- UKPDS:
-
United Kingdom prospective diabetes study
References
Ahren B, Landin-Olsson M, Jansson PA, Svensson M, Holmes D, Schweizer A. Inhibition of dipeptidyl peptidase-4 reduces glycemia, sustains insulin levels, and reduces glucagon levels in type 2 diabetes. J Clin Endocrinol Metab. 2004;89(5):2078–84.
Chon S, Gautier JF. An update on the effect of incretin-based therapies on beta-cell function and mass. Diabetes Metab J. 2016;40(2):99–114.
Barnett A. DPP-4 inhibitors and their potential role in the management of type 2 diabetes. Int J Clin Pract. 2006;60(11):1454–70.
Foley JE, Jordan J. Weight neutrality with the DPP-4 inhibitor, vildagliptin: mechanistic basis and clinical experience. Vasc Health Risk Manag. 2010;6:541–8.
Anagnostis P, Athyros VG, Adamidou F, Panagiotou A, Kita M, Karagiannis A, Mikhailidis DP. Glucagon-like peptide-1-based therapies and cardiovascular disease: looking beyond glycaemic control. Diabetes Obes Metab. 2011;13(4):302–12.
Nystrom T, Gutniak MK, Zhang Q, Zhang F, Holst JJ, Ahren B, Sjoholm A. Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am J Physiol Endocrinol Metab. 2004;287(6):E1209–15.
Henderson A. Endothelial dysfunction: a reversible clinical measure of atherogenic susceptibility and cardiovascular inefficiency. Int J Cardiol. 1997;62(Suppl 1):S43–8.
Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. New Engl J Med. 1998;339(4):229–34.
Iso H, Imano H, Kitamura A, Sato S, Naito Y, Tanigawa T, Ohira T, Yamagishi K, Iida M, Shimamoto T. Type 2 diabetes and risk of non-embolic ischaemic stroke in Japanese men and women. Diabetologia. 2004;47(12):2137–44.
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352(9131):854–65.
Selvin E, Bolen S, Yeh HC, Wiley C, Wilson LM, Marinopoulos SS, Feldman L, Vassy J, Wilson R, Bass EB, et al. Cardiovascular outcomes in trials of oral diabetes medications: a systematic review. Arch Intern Med. 2008;168(19):2070–80.
Saenz A, Fernandez-Esteban I, Mataix A, Ausejo M, Roque M, Moher D. Metformin monotherapy for type 2 diabetes mellitus. Cochrane database Syst Rev. 2005;3:cd002966.
Kim YG, Hahn S, Oh TJ, Kwak SH, Park KS, Cho YM. Differences in the glucose-lowering efficacy of dipeptidyl peptidase-4 inhibitors between Asians and non-Asians: a systematic review and meta-analysis. Diabetologia. 2013;56(4):696–708.
Nomoto H, Miyoshi H, Furumoto T, Oba K, Tsutsui H, Inoue A, Atsumi T, Manda N, Kurihara Y, Aoki S. A Randomized controlled trial comparing the effects of sitagliptin and glimepiride on endothelial function and metabolic parameters: Sapporo Athero-Incretin Study 1 (SAIS1). PLoS ONE. 2016;11(10):e0164255.
Nomoto H, Miyoshi H, Furumoto T, Oba K, Tsutsui H, Miyoshi A, Kondo T, Tsuchida K, Atsumi T, Manda N, et al. A comparison of the effects of the GLP-1 analogue liraglutide and insulin glargine on endothelial function and metabolic parameters: a randomized, controlled trial Sapporo Athero-Incretin Study 2 (SAIS2). PLoS ONE. 2015;10(8):e0135854.
Rizzo MR, Barbieri M, Marfella R, Paolisso G, et al. Reduction of oxidative stress and inflammation by blunting daily acute glucose fluctuations in patients with type 2 diabetes: role of dipeptidyl peptidase-IV inhibition. Diabetes Care. 2012;35(10):2076–82.
Koyanagawa N, Miyoshi H, Ono K, Nakamura A, Cho KY, Yamamoto K, Takano Y, Dan-Noura M, Atsumi T. Comparative effects of vildagliptin and sitagliptin determined by continuous glucose monitoring in patients with type 2 diabetes mellitus. Endocr J. 2016;63(8):747–53.
Nomoto H, Kimachi K, Miyoshi H, Kameda H, Cho KY, Nakamura A, Nagai S, Kondo T, Atsumi T. Effects of 50 mg vildagliptin twice daily vs. 50 mg sitagliptin once daily on blood glucose fluctuations evaluated by long-term self-monitoring of blood glucose. Endocr J. 2017;64(4):417–24.
Suzuki K, Watanabe K, Suzuki T, Ouchi M, Futami-Suda S, Igari Y, Nakano H, Oba K. Sitagliptin improves vascular endothelial function in Japanese type 2 diabetes patients without cardiovascular disease. J Diabetes Mellit. 2012;02(03):338–45.
Kubota Y, Miyamoto M, Takagi G, Ikeda T, Kirinoki-Ichikawa S, Tanaka K, Mizuno K. The dipeptidyl peptidase-4 inhibitor sitagliptin improves vascular endothelial function in type 2 diabetes. J Korean Med Sci. 2012;27(11):1364–70.
Mather KJ, Verma S, Anderson TJ. Improved endothelial function with metformin in type 2 diabetes mellitus. J Am Coll Cardiol. 2001;37(5):1344–50.
Naka KK, Papathanassiou K, Bechlioulis A, Pappas K, Kazakos N, Kanioglou C, Kostoula A, Vezyraki P, Makriyiannis D, Tsatsoulis A, et al. Effects of pioglitazone and metformin on vascular endothelial function in patients with type 2 diabetes treated with sulfonylureas. Diabetes Vasc Dis Res. 2012;9(1):52–8.
Fisman EZ, Tenenbaum A. Antidiabetic treatment with gliptins: focus on cardiovascular effects and outcomes. Cardiovasc Diabetol. 2015;14:129.
Manrique C, Habibi J, Aroor AR, Sowers JR, Jia G, Hayden MR, Garro M, Martinez-Lemus LA, Ramirez-Perez FI, Klein T, et al. Dipeptidyl peptidase-4 inhibition with linagliptin prevents western diet-induced vascular abnormalities in female mice. Cardiovasc Diabetol. 2016;15:94.
Murase H, Kuno A, Miki T, Tanno M, Yano T, Kouzu H, Ishikawa S, Tobisawa T, Ogasawara M, Nishizawa K, et al. Inhibition of DPP-4 reduces acute mortality after myocardial infarction with restoration of autophagic response in type 2 diabetic rats. Cardiovasc Diabetol. 2015;14:103.
White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, Perez AT, Fleck PR, Mehta CR, Kupfer S, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. New Engl J Med. 2013;369(14):1327–35.
Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman P, Frederich R, Wiviott SD, Hoffman EB, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. New Engl J Med. 2013;369(14):1317–26.
Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, Josse R, Kaufman KD, Koglin J, Korn S, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. New Engl J Med. 2015;373(3):232–42.
Giaccari A, Giorda CB, Riccardi G, De Micheli A, Bruno G, Monge L, Frontoni S. Management of hyperglycemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35:1364–79.
Kao J, Tobis J, McClelland RL, Heaton MR, Davis BR, Holmes DR Jr, Currier JW. Relation of metformin treatment to clinical events in diabetic patients undergoing percutaneous intervention. Am J Cardiol. 2004;93(11):1347–50.
Mannucci E, Ognibene A, Cremasco F, Bardini G, Mencucci A, Pierazzuoli E, Ciani S, Messeri G, Rotella CM. Effect of metformin on glucagon-like peptide 1 (GLP-1) and leptin levels in obese nondiabetic subjects. Diabetes Care. 2001;24(3):489–94.
Maida A, Lamont BJ, Cao X, Drucker DJ. Metformin regulates the incretin receptor axis via a pathway dependent on peroxisome proliferator-activated receptor-alpha in mice. Diabetologia. 2011;54(2):339–49.
Noguchi K, Hirota M, Miyoshi T, Tani Y, Noda Y, Ito H, Nanba S. Single administration of vildagliptin attenuates postprandial hypertriglyceridemia and endothelial dysfunction in normoglycemic individuals. Exp Ther Med. 2015;9(1):84–8.
Ayaori M, Iwakami N, Uto-Kondo H, Sato H, Sasaki M, Komatsu T, Iizuka M, Takiguchi S, Yakushiji E, Nakaya K, et al. Dipeptidyl peptidase-4 inhibitors attenuate endothelial function as evaluated by flow-mediated vasodilatation in type 2 diabetic patients. J Am Heart Assoc. 2013;2(1):e003277.
Nakamura K, Oe H, Kihara H, Shimada K, Fukuda S, Watanabe K, Takagi T, Yunoki K, Miyoshi T, Hirata K, et al. DPP-4 inhibitor and alpha-glucosidase inhibitor equally improve endothelial function in patients with type 2 diabetes: EDGE study. Cardiovasc Diabetol. 2014;13:110.
Ida S, Murata K, Betou K, Kobayashi C, Ishihara Y, Imataka K, Uchida A, Monguchi K, Kaneko R, Fujiwara R, et al. Effect of trelagliptin on vascular endothelial functions and serum adiponectin level in patients with type 2 diabetes: a preliminary single-arm prospective pilot study. Cardiovasc Diabetol. 2016;15(1):153.
Li F, Chen J, Leng F, Lu Z, Ling Y. Effect of saxagliptin on circulating endothelial progenitor cells and endothelial function in newly diagnosed type 2 diabetic patients. Exp Clin Endocrinol Diabetes. 2017;125(6):400–7.
Baltzis D, Dushay JR, Loader J, Wu J, Greenman RL, Roustit M, Veves A. Effect of linagliptin on vascular function: a randomized, placebo-controlled study. J Clin Endocrinol Metab. 2016;101(11):4205–13.
Mita T, Katakami N, Shiraiwa T, Yoshii H, Onuma T, Kuribayashi N, Osonoi T, Kaneto H, Kosugi K, Umayahara Y, et al. Sitagliptin attenuates the progression of carotid intima-media thickening in insulin-treated patients with type 2 diabetes: the Sitagliptin Preventive Study of Intima-Media Thickness Evaluation (SPIKE): a randomized controlled trial. Diabetes Care. 2016;39(3):455–64.
Mita T, Katakami N, Yoshii H, Onuma T, Kaneto H, Osonoi T, Shiraiwa T, Kosugi K, Umayahara Y, Yamamoto T, et al. Alogliptin, a dipeptidyl peptidase 4 inhibitor, prevents the progression of carotid atherosclerosis in patients with type 2 diabetes: the study of preventive effects of alogliptin on diabetic atherosclerosis (SPEAD-A). Diabetes Care. 2016;39(1):139–48.
Dell’Oro R, Maloberti A, Nicoli F, Villa P, Gamba P, Bombelli M, Mancia G, Grassi G. Long-term Saxagliptin Treatment improves endothelial function but not pulse wave velocity and intima-media thickness in type 2 diabetic patients. High blood Press Cardiovas Prev. 2017.
Maruhashi T, Higashi Y, Kihara Y, Yamada H, Sata M, Ueda S, Odawara M, Terauchi Y, Dai K, Ohno J, et al. Long-term effect of sitagliptin on endothelial function in type 2 diabetes: a sub-analysis of the PROLOGUE study. Cardiovasc Diabetol. 2016;15(1):134.
Benjamin EJ, Larson MG, Keyes MJ, Mitchell GF, Vasan RS, Keaney JF Jr, Lehman BT, Fan S, Osypiuk E, Vita JA. Clinical correlates and heritability of flow-mediated dilation in the community: the Framingham Heart Study. Circulation. 2004;109(5):613–9.
Iwata M, Miyashita Y, Kumagai H. Seasonal variation of endothelium-dependent flow-mediated vasodilation measured in the same subjects. Am J Cardiovasc Dis. 2012;2(2):111–5.
Li S, Wu Y, Yu G, Xia Q, Xu Y. Angiotensin II receptor blockers improve peripheral endothelial function: a meta-analysis of randomized controlled trials. PLoS ONE. 2014;9(3):e90217.
Takagi H, Yamamoto H, Iwata K, Goto SN, Umemoto T. Low-density lipoprotein-independent improvement of flow-mediated dilatation with atorvastatin: a meta-analysis and meta-regression of randomized controlled trials. Int J Cardiol. 2012;158(2):285–9.
Papathanassiou K, Naka KK, Kazakos N, Kanioglou C, Makriyiannis D, Pappas K, Katsouras CS, Liveris K, Kolettis T, Tsatsoulis A, et al. Pioglitazone vs glimepiride: differential effects on vascular endothelial function in patients with type 2 diabetes. Atherosclerosis. 2009;205(1):221–6.
Wascher TC, Schmoelzer I, Wiegratz A, Stuehlinger M, Mueller-Wieland D, Kotzka J, Enderle M. Reduction of postchallenge hyperglycaemia prevents acute endothelial dysfunction in subjects with impaired glucose tolerance. Eur J Clin Invest. 2005;35(9):551–7.
Romualdi D, Costantini B, Selvaggi L, Giuliani M, Cristello F, Macri F, Bompiani A, Lanzone A, Guido M. Metformin improves endothelial function in normoinsulinemic PCOS patients: a new prospective. Hum Reprod. 2008;23(9):2127–33.
Bakhashab S, Ahmed FW, Schulten HJ, Bashir A, Karim S, Al-Malki AL, Gari MA, Abuzenadah AM, Chaudhary AG, Alqahtani MH, et al. Metformin improves the angiogenic potential of human CD34(+) cells co-incident with downregulating CXCL10 and TIMP1 gene expression and increasing VEGFA under hyperglycemia and hypoxia within a therapeutic window for myocardial infarction. Cardiovasc Diabetol. 2016;15:27.
Triggle CR, Ding H. Metformin is not just an antihyperglycaemic drug but also has protective effects on the vascular endothelium. Acta Physiol. 2017;219(1):138–51.
Maruhashi T, Soga J, Fujimura N, Idei N, Mikami S, Iwamoto Y, Kajikawa M, Matsumoto T, Hidaka T, Kihara Y, et al. Relationship between flow-mediated vasodilation and cardiovascular risk factors in a large community-based study. Heart. 2013;99(24):1837–42.
Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali T, Umans JG, Howard BV. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the strong heart study. Hypertension. 2007;50(1):197–203.
Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, Tsai J, Orazem J, Magorien RD, O’Shaughnessy C, Ganz P. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. New Engl J Med. 2005;352(1):29–38.
Sharma RK, Singh VN, Reddy HK. Thinking beyond low-density lipoprotein cholesterol: strategies to further reduce cardiovascular risk. Vasc Health Risk Manag. 2009;5:793–9.
Walldius G, Jungner I. Apolipoprotein B and apolipoprotein A–I: risk indicators of coronary heart disease and targets for lipid-modifying therapy. J Intern Med. 2004;255(2):188–205.
Cromwell WC, Barringer TA. Low-density lipoprotein and apolipoprotein B: clinical use in patients with coronary heart disease. Current Cardiol Rep. 2009;11(6):468–75.
Hoang A, Murphy AJ, Coughlan MT, Thomas MC, Forbes JM, O’Brien R, Cooper ME, Chin-Dusting JP, Sviridov D. Advanced glycation of apolipoprotein A–I impairs its anti-atherogenic properties. Diabetologia. 2007;50(8):1770–9.
Sierra-Johnson J, Fisher RM, Romero-Corral A, Somers VK, Lopez-Jimenez F, Ohrvik J, Walldius G, Hellenius ML, Hamsten A. Concentration of apolipoprotein B is comparable with the apolipoprotein B/apolipoprotein A–I ratio and better than routine clinical lipid measurements in predicting coronary heart disease mortality: findings from a multi-ethnic US population. Eur Heart J. 2009;30(6):710–7.
Yano W, Inoue N, Ito S, Itou T, Yasumura M, Yoshinaka Y, Hagita S, Goto M, Nakagawa T, Inoue K, et al. Mechanism of lipid-lowering action of the dipeptidyl peptidase-4 inhibitor, anagliptin, in low-density lipoprotein receptor-deficient mice. J diabetes Invest. 2017;8(2):155–60.
Shigiyama F, Kumashiro N, Miyagi M, Iga R, Kobayashi Y, Kanda E, Uchino H, Hirose T. Linagliptin improves endothelial function in patients with type 2 diabetes: a randomized study of linagliptin effectiveness on endothelial function. J Diabetes Invest. 2017;8(3):330–40.
Kishida K, Funahashi T, Shimomura I. Molecular mechanisms of diabetes and atherosclerosis: role of adiponectin. Endocr Metab Immune Disord Drug Targets. 2012;12(2):118–31.
Kishida K, Funahashi T, Shimomura I. Adiponectin as a routine clinical biomarker. Best Pract Res Clin Endocrinol Metab. 2014;28(1):119–30.
Miyagawa K, Kondo T, Goto R, Matsuyama R, Ono K, Kitano S, Kawasaki S, Igata M, Kawashima J, Matsumura T, et al. Effects of combination therapy with vildagliptin and valsartan in a mouse model of type 2 diabetes. Cardiovasc Diabetol. 2013;12:160.
Shestakova MV, Suhareva O, Chernova TO, Shmushkovich IA, Aleksandrov AA, Il’in AV, Dedov II. A combination of dipeptidyl peptidase-4 inhibitor and metformin in the treatment of patients with type 2 diabetes mellitus: effective control of glycemia, weight, and quantitative body composition. Ter Arkh. 2013;85(8):49–55.
Hibuse T, Maeda N, Kishida K, Kimura T, Minami T, Takeshita E, Hirata A, Nakagawa Y, Kashine S, Oka A, et al. A pilot three-month sitagliptin treatment increases serum adiponectin level in Japanese patients with type 2 diabetes mellitus–a randomized controlled trial START-J study. Cardiovasc Diabetol. 2014;13:96.
Yamauchi T, Kamon J, Waki H, Terauchi Y, Kubota N, Hara K, Mori Y, Ide T, Murakami K, Tsuboyama-Kasaoka N, et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat Med. 2001;7(8):941–6.
Hattori Y, Suzuki K, Hattori S, Kasai K. Metformin inhibits cytokine-induced nuclear factor kappaB activation via AMP-activated protein kinase activation in vascular endothelial cells. Hypertension. 2006;47(6):1183–8.
Authors’ contributions
HM and NK: Conceived and designed the experiments. NK, HM, HN, AM, CY, AI, KT, NM, YK, AN, and SA: Performed the experiments. NK, HM, and KO: Analyzed the data. TF: Contributed reagents/materials/analysis tools. NK, HM, and HN: Wrote the paper. KO: Statistical analysis. TA: Reviewed and edited the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors thank Ms. N. Fujimori and Ms. M. Watanabe for technical assistance, the Translational Research and Clinical Trial Center of Hokkaido University Hospital for data analysis and useful discussion, and Ms. S. Miura for all the assessments of FMD. SAIS study group consists of Y. Edagawa, M. Oita, A. Kondo, K. Takahashi, H. Sugawara, M. Dan-noura, Y. Takano, N. Kitao, N. Koyanagawa, A. Miya, K. Yamamoto, C. Yamamoto, H. Nomoto, Y. Kameda, KY Cho, A. Nakamura, H. Miyoshi and T. Atsumi belong to Division of Rheumatology, Endocrinology and Nephrology, Hokkaido University Graduate School of Medicine, T. Watanabe belongs to First Department of Medicine, Hokkaido University, K. Takahashi, N. Koyanagawa belong to Clark Hospital, K. Kito and C. Yamamoto belong to Ogasawara Clinic Sapporo Hospital, M. Endo belongs to Ohtsuka Eye Hospital, J. Takeuchi belongs to Sapporo Diabetes and Thyroid Clinic, S. Nagai belongs to NTT East Japan Sapporo Hospital, H. Masuda belongs to Japan Community Healthcare and Organization Sapporo Hokushin Hospital, A. Inoue belongs to Japan Community Healthcare and Organization Hokkaido Hospital, Y. Ono belongs to Yuri Ono Clinic, K. Tsuchida and N. Manda belong to Manda Memorial Hospital, Y. Kurihara belongs to Kurihara Clinic and S. Aoki belongs to Aoki Clinic.
Competing interests
The authors of this manuscript have the following competing interests: H. Miyoshi has received honoraria for lectures from Astellas, AstraZeneca, Dainippon Pharma, Eli Lilly, Kissei, Mitsubishi Tanabe Pharma, MSD, Novartis, Novo Nordisk, and Sanofi; and received scholarship grants from Astellas, AstraZeneca, Daiichi Sankyo, Eli Lilly, Mitsubishi Tanabe Pharma, MSD, Novo Nordisk, Sanofi, Takeda, and Taisho Pharmaceutical Co., Ltd. T. Atsumi has received honoraria for lectures from Takeda Pharmaceutical, Mitsubishi Tanabe Pharma, Pfizer, Eisai, Avvie, UCB Japan, Astellas Pharma and Chugai Pharmaceutical Co., Ltd; received research grants from Astellas, Chugai, Sanofi, Eisai, Alexion, Bristol-Myers Squibb, Mitsubishi Tanabe Pharma, and Janssen Pharmaceutical K.K.; and received scholarship grants from Astellas, Takeda, Mitsubishi Tanabe Pharma, Chugai, Daiichi Sankyo, Eisai and Bayer, Ltd. This does not alter our adherence to Cardiovascular Diabetology policies on sharing data and materials.
Availability of data and materials
All relevant data are within the paper and its supporting information files.
Consent for publication
Written informed consent was obtained from study participants for participation in the study and for publication of this report. Consent and approval for publication was also obtained from the institutional review board of Hokkaido University.
Ethics approval and consent to participate
This study protocol was reviewed and approved by the institutional review board of Hokkaido University and written consent was obtained from all participants.
Funding
This work was financially supported by grants from the Japan Diabetes Foundation and the Hokkaido Diabetes Clinical Research Organization, including Aoki Clinic, Kurihara Clinic, Manda Memorial Hospital, Hokkaido University Hospital, NTT East Japan Sapporo Hospital, Yuri Ono Clinic, and Clark Hospital.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional files
12933_2017_607_MOESM1_ESM.pptx
Additional file 1: Figure S1. Relationship between the changes in FMD and baseline FMD with vildagliptin or high-dose metformin.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kitao, N., Miyoshi, H., Furumoto, T. et al. The effects of vildagliptin compared with metformin on vascular endothelial function and metabolic parameters: a randomized, controlled trial (Sapporo Athero-Incretin Study 3). Cardiovasc Diabetol 16, 125 (2017). https://doi.org/10.1186/s12933-017-0607-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-017-0607-6