
Abstract
Background
Previous studies using trajectory models focused on examining the longitudinal changes in triglyceride-glucose (TyG) levels and lifestyle scores separately, without exploring the joint evolution of these two factors. This study aimed to identify the multi-trajectories of TyG levels and lifestyle scores and assess their association with the risk of cardiovascular disease (CVD).
Methods
The study enrolled 47,384 participants from three health surveys of the Kailuan Study. The TyG index was computed as Ln [fasting triglycerides (mg/dL) × fasting blood glucose (mg/dL)/2], and the lifestyle scores were derived from five factors, including smoking, alcohol consumption, physical activity, sedentary behaviors, and salt intake. A group-based multi-trajectory model was adopted to identify multi-trajectories of TyG levels and lifestyle scores. The association of identified multi-trajectories with incident CVD was examined using Cox proportional hazard model.
Results
Five distinct multi-trajectories of TyG levels and lifestyle scores were identified. During a median follow-up period of 10.98 years, 3042 participants developed CVD events (2481 strokes, 616 myocardial infarctions, and 55 co-current stroke and myocardial infarctions). In comparison to group 3 with the lowest TyG levels and the best lifestyle scores, the highest CVD risk was observed in group 5 characterized by the highest TyG levels and moderate lifestyle scores (HR = 1.76, 95% CI: 1.50–2.05). Group 2 with higher TyG levels and the poorest lifestyle scores had a 1.45-fold (95% CI 1.26–1.66) risk of CVD, and group 1 with lower TyG levels and poorer lifestyle scores had a 1.33-fold (95% CI 1.17–1.50) risk of CVD. Group 4, with moderate TyG levels and better lifestyle scores, exhibited the lowest CVD risk (HR = 1.32, 95% CI: 1.18–1.47).
Conclusions
Distinct multi-trajectories of TyG levels and lifestyle scores corresponded to differing CVD risks. The CVD risk caused by a high level TyG trajectory remained increased despite adopting healthier lifestyles. These findings underscored the significance of evaluating the combined TyG and lifestyle patterns longitudinally, and implementing early interventions to reduce CVD risk by lowering TyG levels.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide [1]. Diabetes, metabolic syndrome, and obesity are known to be important, modifiable risk factors for CVD, all characterized by insulin resistance [2]. The triglyceride-glucose (TyG) index, calculated from fasting triglyceride and blood glucose levels, offers an improved and cost-effective marker for identifying insulin resistance [3, 4]. A growing number of studies have reported the predictive value of the TyG index in CVD. In the Iranian population, each standard deviation increase in the TyG index was associated with a 1.16-fold increase in the CVD risk and a 1.19-fold increase in coronary heart disease risk [5]. A linear association between the TyG index and stroke risk has been observed as well [6].
Given the dynamic nature of both CVD progression and individual TyG levels, assessing only a single time-point TyG level has limitations. Utilizing trajectory modeling enables the tracking of individual trends and recognition of diverse change patterns, and offers more precise approaches for personalized CVD prevention and intervention [7]. Few studies examined the association between changes in TyG over time and CVD incidence, and the results indicated that individuals with TyG trajectory at a high level were independently associated with an increased CVD risk, regardless of the baseline TyG index [8, 9].
However, the existing investigations did not consider the correlation of TyG with lifestyle and assessed the effect of TyG on CVD separately. Notably, the Healthy Lifestyle Promotion Program for Yaquis revealed significant short- and medium-term decreases in the Homeostasis Model Assessment of Insulin Resistance and TyG index among program completers [10]. In another randomized controlled trial, diabetes-related markers, including TyG, weight, fasting glucose, and triglyceride, also improved across all four lifestyle interventions [11]. A healthy lifestyle holds a crucial role in the context of overall well-being, with long-term benefits for CVD reduction [12, 13]. While evidence showed independent changes in TyG and lifestyle, co-evolution patterns in both remained unknown. Moreover, there was an absence of research on the impact of combined TyG and lifestyle trajectories on CVD.
Consequently, we used the Kailuan Study and employed group-based multi-trajectory modeling, a discovery-oriented statistical approach, to identify longitudinal multi-trajectories of TyG levels and lifestyle scores within the Chinese population. This approach enabled the identification of subgroups with similar changing patterns over time. We also examined the associations between the identified multi-trajectory groups and subsequent CVD risk, to further characterize risk differences between different subgroups.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study population and study design
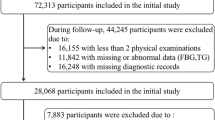
Participants were recruited from the Kailuan Study, a prospective cohort conducted at Kailuan General Hospital and its 10 affiliated hospitals. The study details have been previously described [14]. Briefly, participants from the Kailuan community completed the initial survey through face-to-face interviews between June 2006 and October 2007, followed by biennial follow-ups. The study’s objectives and design were previously published and registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR-TNRC11001489). Our study had two parts: first, to identify joint developmental trajectories of TyG levels and lifestyle scores from 2006 to 2010 survey in the population; second, to predict CVD after 2010 survey. To meet the temporal requirements for multi-trajectory modeling and allow for a sufficiently long follow-up for incident events, data from health surveys conducted in 2006/07, 2008/09, and 2010/11 survey were included. Participants were excluded based on: (1) missing any of the three health surveys; (2) incomplete data on TyG levels and lifestyle scores at any time point; (3) a history of CVD in or before the third health survey. Ultimately, 47,384 participants were included in the final analytic sample (Fig. 1). Approval for this study was granted by the Ethics Committees of Kailuan General Hospital (Approval No.: 2006-5), and written informed consent was acquired from all enrolled participants.

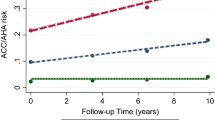
A) Flow chart for the selection of study participants; B) Study design for examine examining the association between multi-trajectories and CVD risk
Definition of lifestyle scores
Trained staff employed a standard questionnaire to gather lifestyle information including smoking status, alcohol consumption, physical activity, sedentary behavior, and salt intake. Each lifestyle aspect received a score on a scale from 0 (poor) to 2 (ideal), detailed in Supplementary Table 1. Total scores ranged from 0 (worst) to 10 (best) [13].
Current smokers were defined as those who smoked daily for at least six months prior. Past smokers had quit before or during the survey. Similarly, current drinkers had consumed alcohol at least once a month in the past year, while past drinkers had quit before or during the survey. Sedentary behavior was categorized as poor (≥ 8 h/day), intermediate (4–7 h/day), or ideal (< 4 h/day). Intermediate physical activity involved ≥ 20 min per session, 1–2 times weekly, while ideal activity meant ≥ 3 times per week during leisure. Due to limited dietary data from 2006 to 2010 survey and considering the impact of salt on CVD in China, salt intake was measured by questionnaire as a proxy for diet quality, which has been validated in previous studies, with a strong association between higher perceived salt intake and lower healthy diet score [15]. Poor, intermediate, and ideal diets corresponded to salt intakes of ≥ 10 g/day, 6–9 g/day, and < 6 g/day.
Definition of the TyG index
The TyG index was computed as Ln [fasting triglycerides (mg/dL) × fasting blood glucose (mg/dL)/2] [16]. fasting blood glucose and fasting triglycerides were measured using standard laboratory methods at Kailuan General Hospital. Blood samples (approximately 5 ml) were drawn from the cephalic vein in the morning after an overnight (> 8 h) fast. Fasting blood glucose was analyzed using the hexokinase method (< 2% coefficient of variation, upper linearity limit: 33.3 mmol/L), and serum fasting triglycerides were assessed using the enzymatic colorimetric method. Hematological parameters were analyzed with an autoanalyzer (Hitachi, Tokyo, Japan).
Assessment of outcomes
The primary outcome of our study was the first occurrence of CVD (including stroke and myocardial infarction). The diagnosis of CVD has been previously described, employing the tenth revision of the International Classification of Diseases (ICD-10) codes for identification (MI: I21, stroke: 160–163). All participants were linked to the municipal social insurance institution and the hospital discharge register system to obtain incidence data for CVD, updated annually. This coverage included all participants of the Kailuan Study. To further identify potential CVD events, we reviewed the discharge lists from 11 hospitals between 2006 and 2021. During biennial health surveys, we gathered insights into participants’ CVD history via questionnaires. A panel of three experienced physicians independently reviewed medical records for suspected CVD cases without knowledge of the study design. The diagnosis of stroke was based on neurological signs, clinical symptoms, and neuroimaging tests, including computed tomography or magnetic resonance imaging, according to the World Health Organization criteria [17]. Myocardial infarction was diagnosed based on clinical symptoms, changes in serum concentrations of cardiac enzymes and biomarkers, and electrocardiographic results [18].
Covariates at baseline
Data on covariates were acquired via questionnaires, basic anthropometric measurements, and laboratory assessments. The demographics collected included age, sex, marital status, and educational background. Medical history and medication usage were assessed by self-report and medical record reviews. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg, antihypertensive drug usage, or self-reported history of physician-diagnosed hypertension. Diabetes mellitus was defined as self-reported diabetes mellitus, glucose-lowering drug usage, or fasting blood glucose ≥ 7 mmol/L. Weight, height, SBP, and DBP were all measured by trained staff. Body mass index (BMI) was computed by dividing weight in kilograms by height in meters squared [19]. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation [20].
All laboratory tests, including high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), high-sensitivity C-reactive protein (Hs-CRP), and serum creatinine, were performed using Hitachi 7600 auto-analyzer.
Statistical analysis
We employed the group-based multi-trajectory modeling, using PROC TRAJ in SAS software [21], to identify jointly longitudinal changes of TyG levels and lifestyle scores within the Kailuan Study. This approach aimed to capture similar changing patterns over time in two variables [7]. Notably, when constructing the model and assigning cluster membership, both TyG levels and lifestyle scores at each visit were taken into consideration. To determine the optimal number of stable trajectories for inclusion in the multi-trajectory model and validate statistical assumptions, separate estimations were initially conducted for each dimension. Model comparison started with a single category and progressively increased the categories until model fit indicators no longer met the recommended criteria or were unable to differentiate meaningful trajectories. We evaluated fit indices including lower absolute Bayesian Information Criterion, log-likelihood ratio compared to the prior model, posterior probabilities of group allocation > 0.7, group size > 5%, and odds of correct classification > 5. Subsequently, data visualization methods were employed to evaluate data separation and model fit, following specific reporting guidelines [22].
Person-years were calculated from the date of the 2010 survey to the date of the first occurrence of CVD, death, or the end of the follow-up (31 December 2021), whichever came first. Kaplan-Meier method was utilized to estimate CVD probabilities and log-rank tests were employed to compare inter-group differences. To explore the association between multi-trajectory groups and the occurrences of CVD, stroke, and myocardial infarction, we conducted Cox proportional hazards regression for each outcome separately. Group 3, characterized by the lowest TyG levels and the best lifestyle scores, was used as the reference. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported as results. The model met the proportional assumption criteria according to Schoenfeld residuals and log-log tests. Our study comprised three models: Model 1 adjusted for age and sex. Model 2 further adjusted for marital status, education background, and BMI. Model 3 further adjusted for HDL-C, LDL-C, Hs-CRP, eGFR, hypertension, diabetes mellitus, antihypertensive, hypoglycemic, and hypolipidemic medications.
We performed stratified analyses by age, sex, diabetes mellitus and hypertriglyceridemia to assess whether the influence of TyG levels and lifestyle scores multi-trajectories on CVD varied across specific factors. We employed likelihood ratio tests to evaluate interactions between stratified variables and multi-trajectories. To test the robustness of our findings, we performed several sensitivity analyses. First, we adjusted for baseline TyG levels and lifestyle scores to explore whether the effect of multi-trajectories on CVD was independent of baseline conditions. Second, we excluded participants using medications as a separate analysis. Furthermore, we excluded participants with inflammation condition (Hs-CRP ≥ 10 mg/L). To mitigate reverse causality, we conducted a lagged analysis excluding CVD events within the initial 2 years of follow-up. Lastly, we applied a Fine-Gray competing risk model, treating non-CVD deaths as competing risk events.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC). A 2-sided P < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 47,384 participants were enrolled in the current study, with a mean age of 52.42 ± 11.77 years. We identified five distinct multi-trajectories from all investigated models. Trajectories were labeled as group 1 (lower TyG levels and poorer lifestyle scores, n = 10,469, 21.90%), group 2 (higher TyG levels and the poorest lifestyle scores, n = 6559, 13.97%), group 3 (the lowest TyG levels and the best lifestyle scores, n = 11,974, 25.76%), group 4 (moderate TyG levels and better lifestyle scores, n = 15,621, 32.26%), and group 5 (the highest TyG levels and moderate lifestyle scores, n = 2761, 6.11%) detailed in Fig. 2. The average posterior probability of the five multi-trajectories was 0.84 (Supplementary Table 2). Table 1 presented the basic characteristics of participants grouped by multi-trajectories of TyG levels and lifestyle scores. Compared with other groups, participants in group 5 were more likely to be older; men; have hypertension, diabetes mellitus, and dyslipidemia; more likely to take antihypertensive, hypoglycemic, and hypolipidemic medications; and have a higher level of BMI, SBP, DBP, LDL-C, and Hs-CRP.

Multi-trajectory groups of TyG levels and lifestyle scores using group-based multi-trajectory modeling
Multi-trajectory groups of TyG levels and lifestyle scores and CVD
During a median follow-up time of 10.98 (10.53–11.31) years, 3042 participants developed CVD events (2481 strokes, 616 myocardial infarctions, and 55 co-current stroke and myocardial infarctions). The highest incidence rate of CVD was observed in participants in group 5 with the highest TyG levels and moderate lifestyle scores (11.22 per 1000 person-years), while the lowest incidence rate was observed in participants in group 3 with the lowest TyG levels and the best lifestyle scores (4.09 per 1000 person‐years). The Kaplan-Meier curves also showed that participants in group 5 experienced higher risk of CVD, stroke, and myocardial infarction than those in other groups (P < 0.0001 for log‐rank test; Fig. 3).

The Kaplan–Meier curves of cardiovascular disease, stroke, and myocardial infarction
After adjustment for potential confounders, participants in group 5, characterized by the highest TyG levels and moderate lifestyle scores, had the highest risk of CVD (HR = 1.76, 95% CI: 1.50–2.05). This risk was followed by group 2 with higher TyG levels and the poorest lifestyle scores (HR = 1.45, 95% CI: 1.26–1.66), and group 1 with lower TyG levels and poorer lifestyle scores (HR = 1.33, 95% CI: 1.17–1.50). Conversely, participants in group 4, with moderate TyG levels and better lifestyle scores, exhibited the lowest risk of CVD (HR = 1.32, 95% CI: 1.18–1.47). In the subtype analyses of CVD, similar results were yielded for stroke. However, participants in group 4 with moderate TyG levels and better lifestyle scores did not have the lowest risk of myocardial infarction (HR = 1.72, 95% CI: 1.34–2.21), but the second highest (Table 2).
Stratification analyses by age and sex showed the association between multi-trajectory groups of TyG levels and lifestyle scores and CVD were consistent across different subgroups. In contrast, we found associations consistent with the main results only in the non-diabetic and non-hypertriglyceridemia populations, which validated previous studies proposing that the use of the TyG index with CVD may be influenced by hypertriglyceridemia and diabetes [23]. There was no significant interaction between stratified variables and multi-trajectory groups in relation to the risk of CVD (all P values for interaction were > 0.05; Fig. 4). Additionally, adjustment for TyG levels and lifestyle scores at baseline did not change the associations materially (Supplementary Table 3). Sensitivity analysis with excluding medication usage (Supplementary Table 4), excluding Hs-CRP≥10 mg/L (Supplementary Table 5), excluding outcomes within the initial 2 years of follow-up (Supplementary Table 6), and treating non-CVD deaths as competing risk events (Supplementary Table 7), all generated similar findings to the primary analysis.

Stratification analyses by age, sex, diabetes mellitus and hypertriglyceridemia
Discussion
Through group-based multi-trajectory analysis of longitudinal data from 3 health surveys, we identified five distinct combined multi-trajectory groups of TyG levels and lifestyle scores. The findings indicated that participants in group 5, characterized by the highest TyG levels and moderate lifestyle scores, had the highest risk of CVD. This risk was followed by group 2 with higher TyG levels and the poorest lifestyle scores, and group 1 with lower TyG levels and poorer lifestyle scores. Conversely, participants in group 4, with moderate TyG levels and better lifestyle scores, exhibited the lowest risk of CVD. Notably, the application of the TyG index in CVD patients can be affected by increases in TG and glucose levels [23], and we found that the results remained robust in a non-diabetic and non-hypertriglyceridemic population, but the result of CVD in patients with hypertriglyceridemia or diabetes should be further verified.
Limited research has explored the relationship between TyG changes and CVD risk over time. A Chinese study identified three TyG trajectory classes, including low-stable, moderate-stable, and high-increasing, related to different carotid atherosclerosis progression risks, suggesting that TyG trajectories might serve as a valuable tool for identifying individuals at a higher risk [8]. A North American study supported this conclusion but with four TyG trajectories: low, moderate, high, and very high [9]. Earlier Kailuan Study results indicated that long-term TyG trajectories could predict CVD incidence in normal-weight adults [24]. Their study revealed five TyG trajectories. While our study also identified five distinct trajectories, the pattern development differed significantly, possibly due to our consideration of lifestyle influence.
In our study, lifestyle scores were derived from five factors: smoking, alcohol consumption, physical activity, sedentary behaviors, and salt intake. Previous research from our team revealed that these lifestyle trajectory patterns were associated with CVD and mortality risks [13]. Subsequently, a UK BioBank study established a lifestyle score encompassing smoking, physical activity, diet, body mass index, and sleep duration, highlighting an increased risk of ischemic heart disease with declining lifestyle trajectories [25]. Although no direct parallels exist, the trajectory of cardiovascular health scores has been widely studied since the American Heart Association proposed the 7 cardiovascular health metrics. Various studies have demonstrated the efficacy of cardiovascular health trajectories in predicting CVD development [15, 26, 27], indirectly supporting our perspective.
However, previous studies using trajectory modeling only investigated longitudinal changes in TyG levels and lifestyle scores separately, the present study provided new insights into identifying and monitoring joint developmental trajectories of both factors. Employing group-based multi-trajectory modeling, we uniquely defined trajectory groups based on two indicators, allowing us to capture their interrelationships and visualize their joint developmental patterns over time.
We found that different patterns of combined TyG levels and lifestyle scores were associated with varying risks of CVD. Interestingly, compared to the reference group with the lowest TyG levels and the best lifestyle scores, the pattern with the highest TyG levels and moderate lifestyle scores had the highest risk of CVD, whereas the pattern with moderate TyG levels and better lifestyle scores had the lowest risk of CVD. As we know, the TyG index serves as a reliable predictor of insulin resistance. Elevated TyG levels indicate the presence of insulin resistance (> 8.81 in men and > 8.73 in women) [28], which serves as both a pathogenic cause of metabolic abnormalities and a predictor of CVD. Simulated clinical trials using data from the National Health and Nutrition Examination Survey (NHANES) demonstrated that individuals with insulin resistance had a nearly 3-fold higher risk of coronary artery disease compared to those without [29]. Moreover, insulin resistance could remain latent for years before diabetes manifests, and the resulting chronic hyperglycemia leads to oxidative stress, initiating an inflammatory response and even causing irreversible damage to vascular cells that cannot be fully mitigated by an improved lifestyle [30]. The results from our stratified analysis suggested that the importance of the multi-trajectory of TyG levels and lifestyle scores might vary among different subgroups. In individuals without diabetes or hypertriglyceridemia, the multi-trajectory of TyG levels and lifestyle scores appeared to be more sensitive for assessing CVD risk. Both hypertriglyceridemia and diabetes significantly heighten the risks of incident CVD [31]. In cases where participants were already affected by diabetes or hypertriglyceridemia, these factors per se may have already exerted a substantial influence on CVD risk. In such scenarios, the TyG index may provide relatively less additional information for assessing CVD risk. Additionally, it is also possible that patients previously diagnosed with diabetes or hypertriglyceridemia were under treatment or had adopted healthier habits, so their analytical parameters might be well controlled [32]. Our findings underscored the potential clinical application of the TyG index for CVD risk assessment, especially in populations without those overt risk factors.
Our results emphasized the importance of assessing TyG trajectory in CVD progression and taking lifestyle changes into account may help to refine CVD risk stratification and enable the administration of more targeted therapeutics or prevention measures. The advantages of the TyG index lie in its simplicity for clinical application, utilizing routine lab tests, and eliminating the need for insulin measurements. Although various surrogate markers for insulin resistance exist, such as lipid accumulation product (LAP), visceral obesity index (VAI) [33,34,35], atherogenic index of plasma (AIP) [33], etc., the TyG index stands out for its predictive power for cardiometabolic diseases [34]. For example, a study involving Thai police officers demonstrated a strong association between these insulin-resistance surrogate markers and a high prevalence of metabolic syndrome and hypertension. Additionally, the TyG index appeared to outperform other indices in predictive performance [35]. Similarly, a comparable outcome indicated that the TyG index might exhibit superior discriminative performance compared to AIP for predicting poor cardiovascular outcomes in patients with chronic coronary syndrome [34]. [38]We need to take effective treatment to control TyG levels much earlier. However, we did not deny the benefits of improving lifestyle. Active lifestyle changes can enhance lipid metabolism, decrease inflammation, stabilize blood glucose, and reduce blood pressure, offering sustainable cardiovascular benefits [11]. While our study noted a progressive rise in CVD risk with increasing TyG levels, this trend was independent of lifestyle modifications. Although lifestyle remains vital for general well-being, addressing TyG levels could be a pivotal intervention strategy in certain contexts.
Our research utilized a population-based cohort study with comprehensive data collection and CVD event tracking through follow-ups, allowing us to make inclusive adjustments for risk factors. We were not the first study to use multi-trajectory modeling [36, 37], but our study was the first to investigate joint trajectories of TyG levels and lifestyle scores in relation to CVD. Multi-trajectory analysis enhances the accuracy of individual-specific probabilities by considering interrelationships among multiple metrics. Several limitations should also be acknowledged. Firstly, trajectory models are data-driven and the number of groups is not predetermined [7], requiring cautious interpretation of the results. Secondly, trajectory analyses mandate a minimum of three independent time points [38]. To ensure sufficient follow-up time to capture cardiovascular events, we analyzed TyG and lifestyle data from three health surveys, potentially missing longer trends in TyG levels and lifestyle scores. Future research could encompass more examination intervals. Thirdly, the study was conducted in the context of a northern Chinese population, which may limit the generalization of the findings. Fourthly, despite the large sample size of this study, females constituted a small proportion (approximately 24% of the total), especially in stratified analyses, which limited statistical power.
Conclusion
In conclusion, our study identified five distinct multi-trajectory groups of TyG levels and lifestyle scores over a 4-year follow-up period. The findings indicated that individuals with elevated TyG levels, despite relatively healthier lifestyles, continued to face an increased risk of CVD. This observation underscores the value of monitoring longitudinal TyG levels as a predictor of CVD and the need for early implementation of effective interventions to maintain optimal TyG levels, thus reducing CVD risk.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available but are available from the corresponding author at reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- DBP:
-
Diastolic blood pressure
- eGFR:
-
Estimated glomerular filtration rate
- HDL-C:
-
High-density lipoprotein cholesterol
- Hs-CRP:
-
High sensitivity C-reactive protein
- HR:
-
Hazard ratio
- LDL-C:
-
Low-density lipoprotein cholesterol
- SBP:
-
Systolic blood pressure
- TyG:
-
Triglyceride-glucose
References
Kivimäki M, Steptoe A. Effects of stress on the development and progression of Cardiovascular Disease. Nat Rev Cardiol. 2018;15(4):215–29.
Adeva-Andany MM, Martínez-Rodríguez J, González-Lucán M, Fernández-Fernández C, Castro-Quintela E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab Syndr. 2019;13(2):1449–55.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Guerrero-Romero F, Villalobos-Molina R, Jiménez-Flores JR, Simental-Mendia LE, Méndez-Cruz R, Murguía-Romero M, Rodríguez-Morán M. Fasting triglycerides and glucose index as a diagnostic test for insulin resistance in young adults. Arch Med Res. 2016;47(5):382–7.
Barzegar N, Tohidi M, Hasheminia M, Azizi F, Hadaegh F. The impact of triglyceride-glucose index on incident cardiovascular events during 16 years of follow-up: Tehran lipid and glucose study. Cardiovasc Diabetol. 2020;19(1):155.
Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic Cardiovascular Disease: a population-based study. BMC Med. 2020;18(1):361.
Nagin DS, Tremblay RE. Developmental trajectory groups: fact or a useful statistical fiction? Criminology 2005, 43(4):873–904.
Yu H, Tao L, Li YG, Yang L, Liu D, Wang Y, Hao X, He H, Che Y, Wang P, et al. Association between triglyceride-glucose index trajectories and carotid Atherosclerosis progression. Cardiovasc Diabetol. 2023;22(1):130.
Tai S, Fu L, Zhang N, Zhou Y, Xing Z, Wang Y. Impact of baseline and trajectory of triglyceride-glucose Index on Cardiovascular outcomes in patients with type 2 Diabetes Mellitus. Front Endocrinol (Lausanne). 2022;13:858209.
Castro-Juarez AA, Serna-Gutiérrez A, Alemán-Mateo H, Gallegos-Aguilar AC, Dórame-López NA, Valenzuela-Sánchez A, Valenzuela-Guzmán DM, Díaz-Zavala RG, Urquidez-Romero R, Esparza-Romero J. Effectiveness of a Lifestyle Change Program on Insulin Resistance in Yaquis Indigenous Populations in Sonora, Mexico: PREVISY. Nutrients 2023, 15(3).
Navas-Carretero S, San-Cristobal R, Siig Vestentoft P, Brand-Miller JC, Jalo E, Westerterp-Plantenga M, Simpson EJ, Handjieva-Darlenska T, Stratton G, Huttunen-Lenz M, et al. Appraisal of triglyceride-related markers as early predictors of metabolic outcomes in the PREVIEW lifestyle intervention: a controlled post-hoc trial. Front Nutr. 2021;8:733697.
Kaminsky LA, German C, Imboden M, Ozemek C, Peterman JE, Brubaker PH. The importance of healthy lifestyle behaviors in the prevention of Cardiovascular Disease. Prog Cardiovasc Dis. 2022;70:8–15.
Ding X, Fang W, Yuan X, Seery S, Wu Y, Chen S, Zhou H, Wang G, Li Y, Yuan X, et al. Associations between healthy lifestyle trajectories and the incidence of Cardiovascular Disease with all-cause mortality: a large, prospective, Chinese cohort study. Front Cardiovasc Med. 2021;8:790497.
Zhou H, Ding X, Yang Q, Chen S, Li Y, Zhou X, Wu S. Associations of Hypertriglyceridemia Onset Age with Cardiovascular Disease and all-cause mortality in adults: a Cohort Study. J Am Heart Assoc. 2022;11(20):e026632.
Wu S, An S, Li W, Lichtenstein AH, Gao J, Kris-Etherton PM, Wu Y, Jin C, Huang S, Hu FB, et al. Association of Trajectory of Cardiovascular Health Score and Incident Cardiovascular Disease. JAMA Netw Open. 2019;2(5):e194758.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, Jacques-Camarena O, Rodríguez-Morán M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51.
Stroke–1989. Recommendations on Stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular disorders. Stroke. 1989;20(10):1407–31.
Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A. Myocardial Infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation. 1994;90(1):583–612.
Reynolds K, Gu D, Whelton PK, Wu X, Duan X, Mo J, He J. Prevalence and risk factors of overweight and obesity in China. Obes (Silver Spring). 2007;15(1):10–8.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
JONES BL, NAGIN DS. A SAS Procedure based on mixture models for estimating Developmental trajectories. Sociol Methods Res. 2001;29(3):374–93.
Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6:109–38.
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in Cardiovascular Diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
Tian X, Zuo Y, Chen S, Meng X, Chen P, Wang Y, Wu S, Luo Y, Wang A. Distinct triglyceride-glucose trajectories are associated with different risks of incident Cardiovascular Disease in normal-weight adults. Am Heart J. 2022;248:63–71.
Gao Y, Chen Y, Hu M, Song J, Zhang Z, Sun H, Wang J, Lin Y, Wu IXY. Lifestyle trajectories and ischaemic Heart Diseases: a prospective cohort study in UK Biobank. Eur J Prev Cardiol. 2023;30(5):393–403.
Huang Z, Chen Z, Wang X, Ding X, Cai Z, Li W, Cai Z, Lan Y, Chen G, Fang W, et al. Association of Cardiovascular Health score trajectory with Incident Myocardial Infarction in Hypertensive patients. Hypertension. 2022;79(11):2622–30.
Zhou H, Ding X, Wu S, Yan J, Cao J. Association of cardiovascular health score trajectory and risk of subsequent Cardiovascular Disease in non-diabetic population: a cohort study. BMC Public Health. 2023;23(1):1043.
Yu X, Wang L, Zhang W, Ming J, Jia A, Xu S, Li Q, Ji Q. Fasting triglycerides and glucose index is more suitable for the identification of metabolically unhealthy individuals in the Chinese adult population: a nationwide study. J Diabetes Investig. 2019;10(4):1050–8.
Eddy D, Schlessinger L, Kahn R, Peskin B, Schiebinger R. Relationship of insulin resistance and related metabolic variables to coronary artery Disease: a Mathematical Analysis. Diabetes Care. 2009;32(2):361–6.
Yang Q, Vijayakumar A, Kahn BB. Metabolites as regulators of insulin sensitivity and metabolism. Nat Rev Mol Cell Biol. 2018;19(10):654–72.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. 2019 ACC/AHA Guideline on the primary Prevention of Cardiovascular Disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice guidelines. Circulation. 2019;140(11):e596–e646.
Sánchez-Íñigo L, Navarro-González D, Fernández-Montero A, Pastrana-Delgado J, Martínez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Invest. 2016;46(2):189–97.
Askina L, Tanriverdib O. Is the Atherogenic Index of Plasma (AIP) a Cardiovascular Disease marker? Cor et Vasa. 2023;65(1):100–3.
Erdoğan A, İnan D, Genç Ö, Yıldız U, Demirtola A, Çetin İ, Güler Y, Tekin AF, Barutçu S, Güler A et al. The Triglyceride-Glucose Index Might Be a Better Indicator for Predicting Poor Cardiovascular Outcomes in Chronic Coronary Syndrome. J Clin Med 2023, 12(19).
Ahn N, Baumeister SE, Amann U, Rathmann W, Peters A, Huth C, Thorand B, Meisinger C. Visceral adiposity index (VAI), lipid accumulation product (LAP), and product of triglycerides and glucose (TyG) to discriminate prediabetes and Diabetes. Sci Rep. 2019;9(1):9693.
Tian X, Chen S, Wang P, Zhang Y, Zhang X, Xu Q, Wu S, Wang A. Association of Multitrajectories of lipid indices with premature Cardiovascular Disease: a Cohort Study. J Am Heart Assoc. 2023;12(9):e029173.
Allswede DM, Addington J, Bearden CE, Cadenhead KS, Cornblatt BA, Mathalon DH, McGlashan T, Perkins DO, Seidman LJ, Tsuang MT, et al. Characterizing covariant trajectories of individuals at clinical high risk for psychosis across symptomatic and functional domains. Am J Psychiatry. 2020;177(2):164–71.
Bollen KA, Curran PJ. Latent curve models: a structural equation perspective. John Wiley & Sons; 2006.
Acknowledgements
The authors thank all the survey teams of the Kailuan study group for their contribution and the study participants who contributed their information.
Funding
The work was supported by the Science and Technology Special Fund Projects of Guangdong Province [Grant Numbers: 202053-116, 202053-74].
Author information
Authors and Affiliations
Contributions
SLW and DW had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. SLW, DW, HZ, and XD contributed to the study design and inception. HZ, XD, YLL, and SHC contributed to the acquisition, analysis, or interpretation of data. HZ and XD drafted the manuscript. All authors provided a revision of the manuscript for critically important intellectual content and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was performed according to the guidelines of the Helsinki Declaration and was approved by the Ethics Committee of Kailuan General Hospital. Written informed consent was obtained from all participants for data collection.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, H., Ding, X., Lan, Y. et al. Multi-trajectories of triglyceride-glucose index and lifestyle with Cardiovascular Disease: a cohort study. Cardiovasc Diabetol 22, 341 (2023). https://doi.org/10.1186/s12933-023-02076-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-02076-z