
Abstract
Background
Mental illness represents a major global burden of disease worldwide. It has been hypothesised that individuals with mental illness have greater blood pressure fluctuations that lead to increased cardiovascular risk and target organ damage. This systematic review aims to (i) investigate the association between mental illness and blood pressure variability (BPV) and (ii) describe methods of BPV measurements and analysis which may affect pattern and degree of variability.
Methods
Four electronic databases were searched from inception until 2020. The quality assessment was performed using STROBE criteria. Studies were included if they investigated BPV (including either frequency or time domain analysis) in individuals with mental illness (particularly anxiety/generalised anxiety disorder, depression/major depressive disorder, panic disorder and hostility) and without hypertension. Two authors independently screened titles, abstracts and full texts. A third author resolved any disagreements.
Results
Twelve studies met the inclusion criteria. Three studies measured short-term BPV, two measured long-term BPV and seven measured ultra-short-term BPV. All studies related to short-term BPV using ambulatory and home blood pressure monitoring found a higher BPV in individuals with depression or panic disorder. The two studies measuring long-term BPV were limited to the older population and found mixed results. Mental illness is significantly associated with an increased BPV in younger and middle-aged adults. All studies of ultra-short-term BPV using standard cardiac autonomic assessment; non-invasive continuous finger blood pressure and heart rate signals found significant association between BPV and mental illness. A mixed result related to degree of tilt during tilt assessment and between controlled and spontaneous breathing were observed in patients with psychological state.
Conclusions
Current review found that people with mental illness is significantly associated with an increased BPV regardless of age. Since mental illness can contribute to the deterioration of autonomic function (HRV, BPV), early therapeutic intervention in mental illness may prevent diseases associated with autonomic dysregulation and reduce the likelihood of negative cardiac outcomes. Therefore, these findings may have important implications for patients' future physical health and well-being, highlighting the need for comprehensive cardiovascular risk reduction.
Similar content being viewed by others


Introduction
Mental illness, such as anxiety, depression and bipolar disorder, poses a significant global disease burden [64]. The presence of mental illness is associated with increased morbidity and mortality [36]. Cardiovascular disease is the most common cause of death among individuals with mental illness [15, 36, 50]. This led to the hypothesis that individuals with mental illness have greater blood pressure fluctuations resulting in increased cardiovascular risk and target organ damage [36, 40].
Impaired autonomic function, as reflected in both sympathetic and parasympathetic activity of the autonomic nervous system, is associated with an increased risk of cardiovascular diseases [14]. Conventional methods to assess autonomic function include measurement of heart rate and blood pressure changes in response to a series of challenge manoeuvers. These methods are relatively crude and lack sensitivity, and therefore not routinely used in practice [11]. Newer methods of measuring heart rate and blood pressure changes include measurement of heart rate variability (HRV) and blood pressure variability (BPV). These methods require minimal patient cooperation and have a high level of sensitivity.
HRV is an assessment of beat-to-beat variation in the heart, and is increasingly used because it is simple to measure and is a reliable indicator for autonomic function [4, 40]. Based on studies on heart rate estimation, electrocardiogram (ECG) signals will first undergo a pre-processing step that includes denoising, segmentation, and filtering to remove any undesirable noise or artefacts [49]. The other purpose of filtering is to emphasise the heartbeat peaks (QRS process) of the ECG signals so that the distance between consecutive peaks can be measured (i.e. each R peak corresponds to a heartbeat) [51]. Heart rate and heart rate variability values can be estimated once these steps are completed. A review of heart rate variability and psychopathology suggested that a constantly changing heart rate is a sign of healthy regulatory systems that can successfully adjust to environmental and psychological challenges [47]. Reduced HRV, on the other hand, indicates that the body's stress response is not optimal, potentially exacerbating the negative effects of chronic stress and increasing the risk of stress-related medical conditions. Previous studies reported that HRV indices, as provided by telemedicine and remote healthcare applications [51] were significantly reduced in patients with depression [31, 53] and anxiety disorders, including generalised anxiety disorder (GAD), social anxiety disorder, panic disorder and post-traumatic stress disorder [16, 32]. Thus, we can conclude from a number of studies on HRV and mental illness that lower HRV in patients with mental illness is associated with poorer cardiovascular health outcomes and a variety of vascular diseases [2].
On the other hand, BPV refers to fluctuations in blood pressure that occur within several minutes, over a 24-h period or a longer period of time (several years) [45]. While blood pressure fluctuations over a 24-h period are normally obtained using non-invasive ambulatory blood pressure recorders, continuous, beat-to-beat blood pressure measurements are acquired using the photoplethysmographic (PPG) technique. Long-term BPV has been associated with stroke and coronary events in high-risks patients [55], while visit-to-visit short-term BPV is a prognostic indicator for cardiovascular mortality in patients with hypertension [44]. Although the association between BPV and coronary diseases has been widely reported, the mechanisms linking these two are unclear due to the dynamic nature of blood pressure, which fluctuates with environmental stimulations and daily life challenges [44, 46]. According to Parati et al. [46], some modifiable risk factors that may alter BPV and affect cardiovascular health outcomes include subjects’ reactivity to emotional stimuli (.e.g., mental state, physiological stress) and behavioural factors (e.g., level of physical activity, sleep cycles, postural changes).
While BPV has been widely studied in hypertension [34, 62], less is known about its relationship with mental illness. Several studies have reported an increase in BPV in individuals with mental illness, which has been linked to an increase in their cardiovascular risk and target organ damage. However, conflicting findings with regard to BPV in patients with psychological disorders have been reported. This may be caused by inconsistencies in the study design among different clinical studies, measurement techniques and experimental procedures as well as types of BPV analysis. Therefore, the current systematic review aims to (i) investigate the association between mental illness and BPV; and (ii) provide an in-depth analysis on the study design, blood pressure (BP) measurement techniques and assessment intervals as well as types of BPV indices used in each study. This would help improve the design of future clinical trials, which aim to identify the relationship between BPV and psychological disorders and use BPV as early indicators of cardiovascular diseases in these patients.
Results
Description of studies
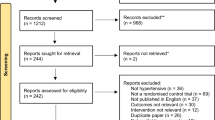
Figure 1 shows the study identification and selection process. Of the 556 records identified through database searching and through other sources, 472 studies were potentially eligible after removal of duplicates. Following screening of title, abstract and full-text articles, 12 articles fulfilled the inclusion criteria.

Flowchart of the study identification and selection process. BPV blood pressure variability
Risk of bias
Table 1 summarises the quality assessment of all studies included in this review (n = 12). The majority of the studies provided detailed information about the research framework. Eleven studies provided a clear description of background of study, aims, objectives and hypotheses in the introduction. No studies reported the sample size calculation, and only two studies addressed missing data [57, 65].
Population characteristics
Table 2 summarises the characteristics of the 12 studies. Five studies involved older adults aged 55 years and above [41, 48, 56, 57, 59], whilst the remaining seven studies assessed BPV in the younger to middle-aged population aged 18 to 46 years [1, 6, 7, 13, 35, 61, 65]. All studies included both males and females [6, 13, 41, 56, 57, 59, 65]. The presence and severity of mental health symptoms or the diagnoses of mental illness was assessed using a number of validated assessments or tools. The assessment tools and the methods of diagnoses are listed in Table 2.
Psychiatric assessment validation
Of the 12 included studies, three aimed at gaining additional insights into the psychological state using the short-term BPV analysis method [1, 7, 41]. Alici et al. [1] diagnosed patients with panic disorder using the DSM-IV criteria (fourth edition of the Diagnostic and Statistical Manual of Mental Disorders), while the study by Carels et al. [7] used the Beck Depression Inventory (BDI), Trait Anxiety Inventory (TAI), Social Support Questionnaire-Short Form (SSQ6) and Daily Stress Inventory (DSI) assessments to distinguish between emotionally responsive and unresponsive individuals. The third study [41] identified subjects with depression using the 15-item Depression rating scale (through a self-administered questionnaire).
Both long-term BPV studies identified patients with late-onset depression [56], generalised anxiety disorder and depression disorder [57] using the MINI International Neuropsychiatric Interview (MINI) screening tool. The interviews were conducted face-to-face by trained clinical psychologists [56].
Of the seven ultra-short-term BPV studies, four involved psychiatrists to diagnose psychological disorders, and trained clinical interviewers to administer structured clinical interviews with DSM-III-R (Diagnostic and Statistical Manual of Mental Disorders, third addition, revised) [6, 35, 65] and DSM-IV. Two studies evaluated the severity of anxiety states using the Spielberger’s State Anxiety Inventory (SAI) [65] and Anxiety Symptom’s scale [48]. Another study [13] performed face-to-face structured clinical interviews based on the MINI International Neuropsychiatric Interview screening tool to identify patients with major depressive disorder. Lastly, self-reported questionnaires, which include Brief Symptoms Inventory (BSI), Spielberger State–Trait Anger Expression Inventory (STAXI) and Toronto Alexithymia scale (TAS-26), were administered by trained researchers in the study by Virtanen et al. [61].
Autonomic nervous system (ANS) testing
A number of physiological assessments were used to determine the HRV and BPV. Studies which measured short-term BPV [1, 7, 41] and long-term BPV [56, 57] utilised either Ambulatory Blood Pressure Monitoring (ABPM) or Home Blood Pressure Monitoring (HBPM). Studies which measured ultra-short-term BPV (second/minute) or beat-to-beat variation used the tilt table or orthostatic challenge test to capture continuous blood pressure (BP) and heart rate (HR) recordings for participants [6, 13, 35, 48, 59, 61, 65]. Out of seven studies on ultra-short-term BPV, we identified two studies that used passive tilt table with a known tilt angles of 60° [35] and 90o [48] for 15-min periods. Two ultra-short-term studies used active standing [65] for 3-min periods [59], whilst the remaining studies used continuous HR and BP measurements from either supine or sitting conditions [6, 13, 61]. Four studies using ultra-short-term also included controlled breathing at 15 breaths/minutes [35, 61], nine breaths/minutes [48] and 12 and 20 breaths/minutes [65].
Blood pressure variability and indices used
Three studies measured short-term BPV [1, 7, 41], two studies measured long-term BPV [56, 57] and seven studies measured ultra-short-term BPV or beat-to-beat variation [6, 13, 35, 48, 59, 61, 65]. Three studies which measured short-term BPV [1, 7, 41] and two studies on long-term BPV [56, 57] assessed time domain variability. Of the seven studies that measured ultra-short BPV, two utilised both time domain and frequency domain methods [48, 65], two evaluated the frequency domain [35, 61] and three determined variability in the time domain [6, 13, 59].
Two types of linear analysis on BPV were used: the time domain and frequency domain analysis. For short-term BPV studies, blood pressure and heart rate data were obtained using non-invasive ambulatory blood pressure monitors/recorders (ABPM) over a 24-h period at regular intervals to observe diurnal and nocturnal blood pressure fluctuations in the patients [1, 7, 41]. For example, Alici et al. [1] and Otsuka et al. [41] observed heart rate and blood pressure readings at 20-min interval and 30-min interval, respectively, during the day and at 30-min interval and 60-min interval, respectively, at night. In contrast, both long-term BPV studies [56, 57] acquired the blood pressure readings using the validated digital electronic tensiometer (OMRON). Since all the heart rate and blood pressure data for short- and long-term BPV were recorded using a device, the stored data were downloaded and processed using statistical analysis method (i.e. SPSS) which resulted in time-domain indices such as standard deviation (SD) [21, 22] and coefficient of variation (CV) [33, 57].
Ultrashort-term BPV studies used standard cardiac autonomic assessment (tilt table/active stand), with beat-to-beat blood pressure signals acquired using the photoplethysmographic (PPG) technique, while R–R intervals were acquired based on the electrocardiogram (ECG) signals [35, 48, 61, 65]. The ECG and finger blood pressure waveforms were then pre-processed using custom written software (i.e. PV-WAVE programming language) [35], where filtering, tracing, and denoising were performed to remove any unwanted artefacts [48]. The QRS peaks of the ECG as well as the peaks/troughs of the cyclical blood pressure waveform within every cardiac cycle were then detected using standard derivative or threshold algorithms for the purpose of estimating heart rate and systolic or diastolic blood pressure [48, 65]. Linear detrending technique was also performed before computing the frequency domain indices using the spectral power analysis method [65]. Autoregressive [35, 48, 59] or fast Fourier transform (FFT) algorithms and triangular smoothing [61] were applied on the extracted beat-to-beat heart rate and systolic/diastolic blood pressure data to obtain the frequency-domain BPV indices: very low-frequency (0.04–0.07 Hz), low-frequency (0.07–0.14 Hz), high-frequency (0.14–0.35 Hz), total power (TP) and low-frequency to high-frequency ratio (LF/HF) [19, 22, 48, 65]:
where very low frequency (VLF), low frequency (LF) and high frequency (HF) power were calculated in absolute values.
Association between mental illness and BPV
Short term: time domain analysis
Three studies on short-term BPV aimed at gaining additional insight into autonomic function by using time domain analysis [1, 7, 41]. Two studies found a higher 24-h [7] and 7-day/24-h [41] average systolic blood pressure (SBP) and diastolic blood pressure (DBP) among individuals with depressive symptoms. The third study [1] similarly reported a higher 24-h average BP specifically in DBP in patients with panic disorder. Apart from 24-h BP fluctuations, short-term BPV was also observed in terms of nocturnal BP dipping and morning BP surge. Panic disorder was significantly associated with lower reduction in both systolic BP and diastolic BP [1].
Long term: time domain analysis
Studies on the association between mental illness and BPV using long-term: time domain analysis were limited to the older population. One study [57] found mixed results while another study [56] found significant association between anxiety and BPV.
Ultra-short term: time domain analysis
Out of the seven studies conducted on ultra-short-term BPV, five presented their findings using parameters within the time domain [6, 13, 48, 59, 65]. Two of the six time domain studies assessed BPV in participants with panic disorder; both studies found increased BPV in patients with panic disorder [6, 65]. Two studies demonstrated increased BPV in individuals with depressive symptoms or major depressive disorder (MDD) [13, 59]. One study found significant association between BPV and anxiety or generalised anxiety disorder [48].
Ultra-short-term: frequency domain analysis
Of the seven studies which evaluated ultrashort-term BPV, four studies found significant association between BPV and mental illness using frequency domain power spectral analysis [35, 48, 61, 65]. Studies by Martinez et al. [35] and Yeragani et al. [65] highlighted a tilt table test in panic disorder participants. Most studies evaluated ultra-short-term BPV during normal, spontaneous breathing. Additional measurements recorded during controlled breathing were conducted in both studies [35, 65] on panic disorder with controlled breathing leading to differences in BPV. Martinez et al. [35] found that controlled breathing phase (15 breaths/minutes) produced significantly lower high frequency and lower total power of SBP in comparison to spontaneous breathing. Yeragani et al. [65] reported controlled in systolic BPV and diastolic BPV, while Martinez et al. [35] did not report diastolic BPV. Yeragani et al. [65] found significantly lower total and low-frequency power for both systolic BPV and diastolic BPV during controlled breathing phase (20 breaths/minutes) compared to spontaneous breathing.
Two studies found significant association between BPV and anxiety or generalised anxiety disorder in spectral analysis parameters [48, 61]. Piccirillo et al. [48] found mixed results with increased very low frequency and total power spectral density if two or more anxiety symptoms were present after tilting. Another study found that higher scores for anxiety were associated with higher low-frequency systolic BPV, while high-frequency diastolic BPV showed no significance at all in anxiety groups [61]. One ultrashort-term BPV study assessed hostility [61] with increased hostility associated with increased low-frequency diastolic BPV (p = 0.001) and increased high-frequency systolic BPV (p = 0.033).
Discussion
Studies using short-term and ultrashort-term BPV supported the hypothesis that young and middle-aged participants with mental illness have dysregulated autonomic function, as reflected by an increased BPV. The association between mental illness and long-term BPV in the older population is less clear.
Short-term BPV which includes day and night time measurements [5] as well as nocturnal BP dipping and morning BP surge [9] indicates blood pressure fluctuations which occur over a 24-h time period. Panic disorder is associated with reduced nocturnal dipping [1]. A reduction in diastolic BP dipping but not systolic BP dipping was observed in individuals with depressive symptoms identified with the depression rating scale [41]. The non-dipper (or reduced nocturnal dipping) patterns observed with panic and depressive symptoms may be a marker of reduced arterial elasticity. Traumatic events, stress or hyperarousal symptoms and poor sleep quality have been associated with changes in nocturnal BP [58]. Stress hormones released by the adrenal glands tend to increase upon sleep onset, resulting in hyperarousal of the sympathetic response at night. Hyperarousal of the sympathetic response results in sleep difficulty, which is commonly associated with psychological illnesses [17, 27, 63]. Reduced baroreflex sensitivity may also explain the presence of non-dipper patterns [24].
Long-term BPV is usually obtained through repeated procedures of BP measurements over days, weeks, months, seasons and even years [45, 52]. Previous studies have shown that generalised anxiety disorder and late-onset depression are associated with higher systolic BPV determined over 8–10 years [56, 57], but major depression is not associated with systolic BPV [56]. The prognostic significance of long-term BPV over short-term BPV remains unclear with factors such as BP treatment and changes in methods of measurement over time likely to confound the overall findings [26, 56].
Ultrashort-term BPV is frequently reflected by the contribution of different humoral systems such as the cardiovascular control system, myogenic response, renin–angiotensin system and endothelium-derived nitric oxide in blood pressure regulation [26]. Previous studies have shown that time domain BPV is significantly associated with panic disorder [65] and anxiety [48]. Higher resting BP has previously been documented in these two groups in studies involving solitary measurement and this observation has been attributed to sympathetic activation and deactivation of vagal activity [60]. Head-up tilting leads to increased sympathetic activation stimulated by the postural challenge, which is usually only demonstrable through frequency domain evaluations manifesting as both increased low-frequency power spectral density and increased low- to high-frequency power density ratio. The percentage increase in these two measurements is reduced in individuals with panic disorder and anxiety symptoms [35, 48, 65]. This may signify reduced sympathetic response due to increased baseline sympathetic activation.
There were significant heterogeneity in both study protocols and sample selections of all studies. The small sample sizes and different time frame may have contributed to the inconsistency in the findings between studies included in this review. The majority of studies included young, middle-aged and older populations; many excluded older adults. The different age groups may also account for the differences in findings between studies. Significant difference in autonomic responses has been observed in older groups compared to younger age groups [43]. Fiske et al. [18] found that increased age is associated with a reduction in neurotransmitter release, which indirectly reduces their mood regulation and the ability to adapt to environmental changes or intrinsic visceral stimuli. Hence, reduction in mood regulation will lead to diminished autonomic reactivity, specifically blood pressure and cerebral blood flow regulation [25].
There is currently a lack of standardisation in terms of protocol for BPV assessment. For instance, there were differences in the tilt angle across the ultrashort-term studies [35, 48]. The duration of the supine position among ultrashort-term studies also differed. Three studies [35, 48, 59] demonstrated a longer supine resting period with at least 10- to 15-min recording, while one study [61] only measured five minutes of supine resting recording. Duration of the baseline recording could play an important role in determining the association between BPV and psychological symptoms. Fluctuations in HR and BP for hostility, for example, could only be detected after a time period long enough to create the interactions between the subjects and their surroundings [54]. Additionally, the relationship between the duration of time for posture recording and autonomic system is still not clear because there is no “gold standard” for tilt-table testing. The different breathing rates employed during postural challenge is likely to result in different in BPV measurements. Controlled breathing may be anxiogenic particularly in individuals with psychological disorders while higher breathing may also lead to hypocapnia resulting from hyperventilation. Therefore, it may not be considered physiological, and hence counterproductive in terms of standardisation of breathing rates to facilitate computational accuracy and reduce noise [23, 35]. Further advancements in both statistical methods and engineering innovations could perhaps resolve this conundrum by measuring breathing rates alongside BP measurements and calculating variability adjusted for spontaneous variabilities in breathing rates which occur within and between individuals.
Our review had some limitations. Firstly, although our review demonstrated changes in BPV in individuals with mental illness, we only included individuals with depression, anxiety, stress and panic disorder. Future studies involving other types of mental illnesses with varying severity, which may affect autonomic function differently, should be considered. Secondly, we did not extract information on medicines use; use of medicines may alter BPV.
Conclusion
Mental illness is significantly associated with an increased BPV in younger and middle-aged adults. The association between mental illness and BPV is less clear in the older population. Larger studies involving older adults are needed to examine the association between mental illness and BPV.
Methods
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 (PRISMA-S) statement [42].
Search strategy and terminology
Four electronic databases, National Library of Medicine (PubMed), PubMed Central® (PMC), MEDLINE® and CINAHL, were searched from inception until 2020. We identified relevant articles reporting human studies published in English for relevant combinations of the following terms and words in titles and abstracts: “Blood pressure variability”, OR “BPV”, OR “blood pressure changes”, AND “psychological disorders”, OR “stress”, OR “depression”, OR “anxiety”, OR “panic disorder”, OR “worry”. Titles, abstracts and full-text articles were assessed for eligibility using methods recommended in the Joanna Briggs Institute (JBI) systematic review [3]. Titles and abstracts of identified articles were independently screened by two authors (NHS and EL) and any disagreements resolved by a third author (SM). Two authors (NHS and EL) assessed the full-text articles of the potentially eligible studies and a third author (SM) resolved any disagreements. Additional articles were identified by checking the reference lists of full-text articles included in this systematic review.
Inclusion and exclusion criteria
Inclusion criteria were: (1) studies that investigated BPV in individuals with mental illness; (2) BPV measures included frequency or time domain analysis; and (3) study participants did not have hypertension. We excluded studies that did not meet with the purpose of the review, such as where BPV was not the main focus of the study.
Data extraction
All papers identified from the initial electronic search process were imported into a reference management software (EndNote Version X9, Clarivate Analytics) where duplicates were removed. Data were extracted by one author (NHS) and crossed checked by a second author (EL) using an electronic data extraction form.
Outcomes
BPV measurements can be divided into short-term, long-term and ultra-short term. Short-term BPV is defined as blood pressure changes or fluctuations that occur over a 24-h time period (minute-to-minute, hour-to-hour, and day-to-night changes) [5, 44]. Long-term BPV is usually obtained through prolonged periods of measurements over days, weeks, months, seasons and even years [45, 52]. Ultrashort-term BPV is defined as beat-to-beat blood pressure measurement over seconds to minutes [26, 44, 45].
BPV analysis can be separated into time domain and frequency domain analysis. Time-domain analysis measures dispersion of blood pressure values over a given time window, while frequency domain analysis measures blood pressure fluctuations as a function of frequency. Time-domain indices are divided into two categories: (1) simply measures of dispersion of average values over a given time window (e.g., standard deviation and coefficient of variation over 10 min of supine rest); (2) estimation that take accounts the sequence of measurements over time (e.g., average real variability, root mean square of real variability, and standard deviation of real variability, all of these take accounts the beat-to-beat changes). Various time domain indices have been proposed, such as the standard deviation (SD) and coefficient variation (CV).
Frequency-domain indices are obtained through spectral analysis techniques, in which we do not express beat-to-beat BP values as a function of time, but as a function of frequency. It concentrates on revealing the cyclical nature hidden in the series of changing beat-to-beat BP values. The frequency and magnitude of these oscillations are measured, which allows the calculation of the power density for separate frequency ranges. Frequency-domain indices are divided into three main components: very-low frequency (0.016–0.04 Hz), low frequency (0.07–0.14 Hz) and high frequency (0.14–0.35 Hz) [21]. Very low frequency metric is related to the renin–angiotensin system, high-frequency component measures the parasympathetic activity, while low frequency measures the sympathetic activity [35, 48]. The ratio of low frequency and high frequency reflects the sympathovagal balance between the sympathetic and the parasympathetic activities [35].
Quality assessment
Risk of bias was assessed using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria [8]. Only 16 items identifying potential sources of bias relevant to the scope and objectives of our review were selected for reporting. The checklist comprised 5 domains: introduction (item 1–3), research methodology (item 4–9), results (item 10–12), discussion (item 13–15) and other information (item 16). Discrepancies were resolved through discussions between two reviewers (NHS, EL), and there were no disagreements between both reviewers regarding the risk of bias assessment.
Availability of data and materials
All relevant data are contained within the article.
Abbreviations
- ANS:
-
Autonomic nervous system
- BPV:
-
Blood pressure variability
- SBPV:
-
Systolic blood pressure variability
- DBPV:
-
Diastolic blood pressure variability
- HRV:
-
Heart rate variability
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- HR:
-
Heart rate
- SDNN:
-
Standard deviation of NN interval
- CV:
-
Coefficient variation
- LF-nu:
-
Low-frequency normalised unit
- HF-nu:
-
High-frequency normalised unit
- TP:
-
Total power
- LF/HF:
-
Ratio of LF and HF
- PD:
-
Panic disorder
- MDD:
-
Major depressive disorder
- GAD:
-
General anxiety disorder
- ABPM:
-
Ambulatory blood pressure monitoring
- HBPM:
-
Home blood pressure monitoring
- LOD:
-
Late-onset depression
- EOD:
-
Early onset depression
- SD:
-
Standard deviation
- BP:
-
Blood pressure
- LLE-SBP:
-
Largest Lyapunov exponent-systolic blood pressure
- LLE-DBP:
-
Largest Lyapunov exponent-diastolic blood pressure
- LLE-HR:
-
Largest Lyapunov exponent-heart rate
- BPvi, Log10 :
-
((BP detrended variance/mean BP2)/(HR detrended variance/mean HR2))
- RRI:
-
RR-interval
- SAP:
-
Systolic arterial pressure
- DAP:
-
Diastolic arterial pressure
References
Alici H, Ercan S, Bulbul F, Alici D, Alpak G, Davutoglu V. Circadian blood pressure variation in normotensive patients with panic disorder. Angiology. 2014;65(8):747–9. https://doi.org/10.1177/0003319713512172.
Alvares GA, Quintana DS, Hickie IB, Guastella AJ. Autonomic nervous system dysfunction in psychiatric disorders and the impact of psychotropic medications: a systematic review and meta-analysis. J Psychiatry Neurosci. 2016;41(2):89–104. https://doi.org/10.1503/jpn.140217.
Aromataris E, Riitano D. Constructing a search strategy and searching for evidence. Am J Nurs. 2014;114(5):49–56. https://doi.org/10.1097/01.NAJ.0000446779.99522.f6.
Berntson GG, Thomas Bigger J, Eckberg DL, Grossman P, Kaufmann PG, Malik M, Nagaraja HN, Porges SW, Saul JP, Stone PH, Van Der Molen MW. Heart rate variability: Origins methods, and interpretive caveats. Psychophysiology. 1997;34(6):623–48. https://doi.org/10.1111/j.1469-8986.1997.tb02140.x.
Brien EO, Parati G, Stergiou G. Ambulatory Blood Pressure Measurement. Hypertension. 2013;62:988–94. https://doi.org/10.1161/HYPERTENSIONAHA.113.02148.
Bystritsky A, Shapiro D. Continuous physiological changes and subjective reports in panic patients: a preliminary methodological report. Biol Psychiat. 1992;32(9):766–77. https://doi.org/10.1016/0006-3223(92)90080-J.
Carels RA, Blumenthal JA, Sherwood A. Emotional responsivity during daily life: relationship to psychosocial functioning and ambulatory blood pressure. Int J Psychophysiol. 2000;36(1):25–33. https://doi.org/10.1016/S0167-8760(99)00101-4.
Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–4. https://doi.org/10.4103/sja.SJA_543_18.
Chadachan VM, Ye MT, Tay JC, Subramaniam K, Setia S. Understanding short-term blood-pressure-variability phenotypes: from concept to clinical practice. Int J Gen Med. 2018;11:241–54. https://doi.org/10.2147/IJGM.S164903.
Chenniappan M. Blood pressure variability: assessment, prognostic significance and management. J Assoc Physicians India. 2015;63(5):47–53.
Conte E, Pieralice M, Laterza V, Losurdo A, Santacroce N, Conte S, Federici A, Giuliani A. Traditional and a new methodology for analysis of heart rate variability: a review physiological and clinical experimental results. In J Res Rev Appl Sci. 2012; 13(1): 206–293. http://www.arpapress.com/Volumes/Vol13Issue1/IJRRAS_13_1_23.pdf
Davies SJC, Ghahramani P, Jackson PR, Noble TW, Hardy PG, Hippisley-cox J, Yeo WW, Ramsay LE. Association of panic disorder and panic attacks with hypertension. Am J Med. 1999;107(4):310–6.
Davydov DM, Shapiro D, Cook IA, Goldstein I. Baroreflex mechanisms in major depression. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(1):164–77. https://doi.org/10.1016/j.pnpbp.2006.08.015.
DePace NL, Mears JP, Yayac M, Colombo J. Cardiac autonomic testing and diagnosing heart disease. “A clinical perspective.” Heart Int. 2014;9(2):37–44. https://doi.org/10.5301/heartint.5000218.
De Hert M, Correll CU, Bobes J, Cetkovich-Bakmas M, Cohen DAN, Asai I, Detraux J, Gautam S, Möller HJ, Ndetei DM, Newcomer JW, Uwakwe R, Leucht S. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011; 10(1): 52–77. https://doi.org/10.1002/j.2051-5545.2011.tb00014.x
Dimitriev DA, Saperova EV, Dimitriev AD. State anxiety and nonlinear dynamics of heart rate variability in students. PLoS ONE. 2016;11(1):1–22. https://doi.org/10.1371/journal.pone.0146131.
Dodt C, Breckling U, Derad I, Fehm HL, Born J. Plasma epinephrine and norepinephrine concentrations of healthy humans associated with nighttime sleep and morning arousal. Hypertension. 1997;30(1):71–6. https://doi.org/10.1161/01.hyp.30.1.71 (PMID: 9231823).
Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5(1):363–89. https://doi.org/10.1097/01.NAJ.0000422251.65212.4b.
Finucane C, Boyle G, Fan CW, Hade D, Byrne L, Kenny RA. Mayer wave activity in vasodepressor carotid sinus hypersensitivity. Europace. 2010;12(2):247–53. https://doi.org/10.1093/europace/eup385.
Fonkoue IT, Le NA, Kankam ML, DaCosta D, Jones TN, Marvar PJ, Park J. Sympathoexcitation and impaired arterial baroreflex sensitivity are linked to vascular inflammation in individuals with elevated resting blood pressure. Physiol Rep. 2019;7(7):1–12. https://doi.org/10.14814/phy2.14057.
Goh CH, Ng SC, Kamaruzzaman SB, Chin AV, Poi PJH, Chee KH, Imran ZA, Tan MP. Evaluation of two new indices of blood pressure variability using postural change in older fallers. Medicine (United States). 2016;95(19):1–6. https://doi.org/10.1097/MD.0000000000003614.
Goh CH, Ng SC, Kamaruzzaman SB, Chin AV, Tan MP. Standing beat-to-beat blood pressure variability is reduced among fallers in the Malaysian Elders Longitudinal Study. Medicine (United States). 2017;96(42):1–7. https://doi.org/10.1097/MD.0000000000008193.
Gorman JM, Kent JM, Sullivan GM, Coplan JD. Neuroanatomical hypothesis of panic disorder. Am J Psychiatry. 2000;147(4):493–505.
Grippo AJ, Moffitt JA, Johnson AK. Evaluation of baroreceptor reflex function in the chronic mild stress rodent model of depression. Psychosom Med. 2008;70(4):435–43. https://doi.org/10.1097/PSY.0b013e31816ff7dd.
Hotta H, Uchida S. Aging of the autonomic nervous system and possible improvements in autonomic activity using somatic afferent stimulation. Geriatric Gerentol Int. 2010;10(1):127–36. https://doi.org/10.1111/j.1447-0594.2010.00592.x.
Höcht C. Blood Pressure Variability: Prognostic Value and Therapeutic Implications. ISRN Hypertension. 2013: 1–16. https://doi.org/10.5402/2013/398485
Huang Y, Mai W, Hu Y, Wu Y, Song Y, Qiu R, et al. Poor sleep quality, stress status, and sympathetic nervous system activation in nondipping hypertension. Blood Press Monit. 2011;16(3):117–23. https://doi.org/10.1097/mbp.0b013e328346a8b4.
Ifeagwazi CM, Egberi HE, Chukwuorji JC. Emotional reactivity and blood pressure elevations: anxiety as a mediator. Psychol Health Med. 2017;23(5):585–92. https://doi.org/10.1080/13548506.2017.1400670.
Jung W, Jang KI, Lee SH. Heart and brain interaction of psychiatric illness: a review focused on heart rate variability, cognitive function, and quantitative electroencephalography. Clin Psychopharmacol Neurosci. 2019;17(4):459–74. https://doi.org/10.9758/cpn.2019.17.4.459.
Kario K. Morning surge in blood pressure and cardiovascular risk: evidence and perspectives. Hypertension. 2010;56(5):765–73. https://doi.org/10.1161/HYPERTENSIONAHA.110.157149.
Kemp AH, Quintana DS, Gray MA, Felmingham KL, Brown K, Gatt JM. Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biol Psychiat. 2010;67(11):1067–74. https://doi.org/10.1016/J.BIOPSYCH.2009.12.012.
Kim K, Lee S, Kim JH. Diminished autonomic neurocardiac function in patients with generalized anxiety disorder. Neuropsychiatr Dis Treat. 2016;12:3111–8. https://doi.org/10.2147/NDT.S121533.
Razanskaite-Virbickiene D, Danyte E, Mockeviciene G, Dobrovolskiene R, Verkauskiene R, Zalinkevicius R. Can coefficient of variation of time-domain analysis be valuable for detecting cardiovascular autonomic neuropathy in young patients with type 1 diabetes: a case control study. BMC Cardiovasc Disord. 2017;17(1):1–9. https://doi.org/10.1186/s12872-016-0467-0.
Li C, Xiong H, Wu W, Tian X, Wang Y, Wu D, Lin WH, Miao F, Zhang H, Huang W, Zhang YT. The relationship between heart-carotid pulse transit time and carotid intima-media thickness in hypertensive patients. J Hum Hypertens. 2015;29(11):663–8. https://doi.org/10.1038/jhh.2015.11.
Martinez JM, Garakani A, Kaufmann H, Aaronson CJ, Gorman JM. Heart rate and blood pressure changes during autonomic nervous system challenge in panic disorder patients. Psychosom Med. 2010;72(5):442–9. https://doi.org/10.1097/PSY.0b013e3181d972c2.
McCorry LK. Physiology of the autonomic nervous system. Am J Pharm Educ. 2007;71(4):270–6. https://doi.org/10.1111/j.1399-6576.1964.tb00252.x.
Melamed S. Emotional reactivity and elevated blood pressure. Psychosom Med. 1987;49(3):217–25. https://doi.org/10.1097/00006842-198705000-00001.
Miller BJ, Paschall CB, Svendsen DP. Mortality and medical comorbidity among patients with serious mental illness. Psychiatr Serv. 2006;57(10):1482–7. https://doi.org/10.1176/ps.2006.57.10.1482.
Nenna A, Lusini M, Spadaccio C, Nappi F, Greco SM, Barbato R, Covino E, Chello M. Heart rate variability: A new tool to predict complications in adult cardiac surgery. J Geriatric Cardiol. 2017;14(11):662–8. https://doi.org/10.11909/j.issn.1671-5411.2017.11.005.
Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, Grassi G, Jordan J, Poulter NR, Rodgers A, Whelton PK. Hypertension. Nat Rev Dis Primers. 2018;4(1):18014. https://doi.org/10.1038/nrdp.2018.14.
Otsuka K, Yamanaka G, Shinagawa M, Murakami S, Yamanaka T, Shibata K, et al. Chronomic community screening reveals about 31% depression, elevated blood pressure and infradian vascular rhythm alteration. Biomed Pharmacother. 2004;58(1):48–55. https://doi.org/10.1016/S0753-3322(04)80010-6.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(n71):1–9. https://doi.org/10.1136/bmj.n71.
Parashar R, Amir M, Pakhare A, Rathi P, Chaudhary L. Age related changes in autonomic functions. J Clin Diagn Res. 2016;10(3):11–5. https://doi.org/10.7860/JCDR/2016/16889.7497.
Parati G, Ochoa JE, Lombardi C, Bilo G. Blood pressure variability: assessment, predictive value, and potential as a therapeutic target. Curr Hypertens Rep. 2015;17(4):1–18. https://doi.org/10.1007/s11906-015-0537-1.
Parati G, Ochoa JE, Lombardi C, Bilo G. Assessment and management of blood-pressure variability. Nat Rev Cardiol. 2013;10(3):143–55. https://doi.org/10.1038/nrcardio.2013.1.
Parati G, Torlasco C, Pengo M, Bilo G, Ochoa JE. Blood pressure variability: its relevance for cardiovascular homeostasis and cardiovascular diseases. Hypertens Res. 2020;43(7):609–20. https://doi.org/10.1038/s41440-020-0421-5.
Pham T, Lau ZJ, Chen SHA, Makowski D. Heart rate variability in psychology: a review of hrv indices and an analysis tutorial. Sensors. 2021;21(12):1–20. https://doi.org/10.3390/s21123998.
Piccirillo G, Elvira S, Bucca C, Viola E, Cacciafesta M, Marigliano V. Abnormal passive head-up tilt test in subjects with symptoms of anxiety power spectral analysis study of heart rate and blood pressure. Int J Cardiol. 1997;60(2):121–31. https://doi.org/10.1016/S0167-5273(97)00088-0.
Rajesh KN, Dhuli R. Classification of imbalanced ECG beats using re-sampling techniques and AdaBoost ensemble classifier. Biomed Signal Process Control. 2018;41:242–54. https://doi.org/10.1016/j.bspc.2017.12.004.
Robson D, Gray R. Serious mental illness and physical health problems: a discussion paper. Int J Nurs Stud. 2007;44(3):457–66. https://doi.org/10.1016/j.ijnurstu.2006.07.013.
Ronca V, Giorgi A, Rossi D, Di Florio A, Di Flumeri G, Aricò P, Sciaraffa N, Vozzi A, Tamborra L, Simonetti I, Borghini G. A video-based technique for heart rate and eye blinks rate estimation: a potential solution for telemonitoring and remote healthcare. Sensors. 2021;21(5):1–15. https://doi.org/10.3390/s21051607.
Rothwell PM, Howard SC, Dolan E, Brien EO, Dobson JE, Dahlöf B, Sever PS, Poulter NR. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010;375(9718):895–905. https://doi.org/10.1016/S0140-6736(10)60308-X.
Schulz S, Koschke M, Bär KJ, Voss A. The altered complexity of cardiovascular regulation in depressed patients. Physiol Meas. 2010;31(3):303. https://doi.org/10.1088/0967-3334/31/3/003.
Sloan RP, Shapiro PA Jr, JTB, Bagiella E, Steinman RC, Gorman JM. Cardiac autonomic control and hostility in healthy subjects. Am J Cardiol. 1994;74(3):298–300.
Stevens SL, Wood S, Koshiaris C, Law K, Glasziou P, Stevens RJ, McManus RJ. Blood pressure variability and cardiovascular disease: systematic review and meta-analysis. BMJ (Online). 2016;354:14–6. https://doi.org/10.1136/bmj.i4098.
Tully PJ, Debette S, Tzourio C. The association between systolic blood pressure variability with depression, cognitive decline and white matter hyperintensities : the 3C Dijon MRI study. Psychol Med. 2017. https://doi.org/10.1017/S0033291717002756.
Tully PJ, Tzourio C. Psychiatric correlates of blood pressure variability in the elderly: the Three City cohort study. Physiol Behav. 2017;168:91–7. https://doi.org/10.1016/j.physbeh.2016.10.024.
Ulmer CS, Calhoun PS, Bosworth HB, Dennis MF, Beckham JC. Nocturnal blood pressure non-dipping, posttraumatic stress disorder, and sleep quality in women. Behav Med. 2013;39(4):111–21. https://doi.org/10.1080/08964289.2013.813434.Nocturnal.
Vasudev A, O’Brien JT, Tan MP, Parry SW, Thomas AJ. A study of orthostatic hypotension, heart rate variability and baroreflex sensitivity in late-life depression. J Affect Disord. 2011;131(1–3):374–8. https://doi.org/10.1016/j.jad.2010.11.001.
Veith CR, Lewis N, Linares AO, Barnes FR, Raskind AM, Villacres E, Murburg MM, Ashleigh EA, Peskind ER, Pascualy M, Halter JB, Veith RC. Sympathetic nervous system activity in major depression. Arch Gen Psychiatry. 1994;51(5):411–22.
Virtanen R, Jula A, Salminen JK, Voipio-Pulkki LM, Helenius H, Kuusela T, Airaksinen J. Anxiety and hostility are associated with reduced baroreflex sensitivity and increased beat-to-beat blood pressure variability. Psychosom Med. 2003;65(5):751–6. https://doi.org/10.1097/01.PSY.0000088760.65046.CF.
Wu D, Xu L, Abbott D, Hau WK, Ren L, Zhang H, Wong KKL. Analysis of beat-to-beat blood pressure variability response to the cold pressor test in the offspring of hypertensive and normotensive parents. Hypertens Res. 2017;40(6):581–9. https://doi.org/10.1038/hr.2017.4.
Wuyts J, De Valck E, Vandekerckhove M, Pattyn N, Bulckaert A, Berckmans D, Haex B, Verbraecken J, Cluydts R. The influence of pre-sleep cognitive arousal on sleep onset processes. Int J Psychophysiol. 2012;83(1):8–15. https://doi.org/10.1016/j.ijpsycho.2011.09.016.
Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiat. 2015;72(4):334–41. https://doi.org/10.1016/j.physbeh.2017.03.040.
Yeragani KV, Mallavarapu M, Radhakrishna R, Tancer M, Uhde T. Linear and nonlinear measures of blood pressure variability : increased chaos of blood pressure time series in patients with panic disorder. Depress Anxiety. 2004;95(38):85–95.
Acknowledgements
Not applicable.
Funding
This work was supported by a University of Malaya Health and Wellbeing Cluster Impactful Interdisciplinary Research Grant (Grant Number IIRG024B-2019).
Author information
Authors and Affiliations
Contributions
NHS extracted and organized the literature and wrote the first draft of the manuscript. EL and SM checked the data, reviewed and provided edits to the manuscript. CHG, MPT and RL contributed in the reviewed and provided edits and modification to the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shahimi, N.H., Lim, R., Mat, S. et al. Association between mental illness and blood pressure variability: a systematic review. BioMed Eng OnLine 21, 19 (2022). https://doi.org/10.1186/s12938-022-00985-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12938-022-00985-w