
Abstract
Objective
The present study examined the ability of the body roundness index (BRI) to predict the incidence of diabetes and prediabetes among adults in the USA.
Method
The study enrolled 11,980 adults aged ≥ 20 years from the National Health and Nutrition Examination Survey (NHANES). Logistic regression served as the primary method for analyzing the relevant link between BRI and the incidence of diabetes and prediabetes, including univariate analysis, multivariate regression analysis, smooth curve fitting analysis, and subgroup analysis. What’s more, receiver operating characteristic (ROC) analysis was applied to confirm the predictive values of BRI for diabetes and prediabetes.
Results
Each unit higher than BRI was associated with a 17% increased risk of diabetes and prediabetes after covariate adjustments (OR: 1.17, 95% CI: 1.07–1.27). Those with BRI in the high scores (Q4) possessed an increased likelihood of having diabetes and prediabetes than individuals in the reference group (OR: 1.83, 95% CI: 1.29–2.58). A smooth curve fitting analysis revealed a non-linear trend. The results across all population subgroups were uniform to those of the total population. The ROC curve indicated that the BRI was the best predictor of diabetes and prediabetes among other anthropometric indices.
Conclusions
Diabetes and prediabetes occurrence rates and BRI have a positive and non-linear relationship in American adults. The BRI indices could function as predictive markers for diabetes and prediabetes.
Similar content being viewed by others

Introduction
Characterized by persistent hyperglycemia, type 2 diabetes mellitus (diabetes) is a metabolic disorder that can result in multi-organ complications and stands as a leading global cause of mortality [1]. The International Diabetes Federation predicts that the diabetes prevalence is projected to rise from 9.3 to 10.9% in the range of 2019 to 2045, resulting in a rise in the affected population from 463 million up to 693 million [2]. Prior to diagnosis, the majority of individuals with diabetes undergo a phase of prediabetes. This phase represents an aberrant glucose metabolism state that falls between normal glucose tolerance to diabetes [3]. The yearly transition rate from prediabetes to diabetes is projected to be around 5–10% [3]. Of significant importance, projections indicate that by the year 2030, the number of individuals affected by prediabetes will reach nearly 470 million [3]. Research findings indicate that prediabetes can lead to various complications, including cardiovascular disease (CVD), diabetic retinopathy, neuropathies, and kidney disease [4,5,6,7]. The rising incidence of prediabetes and diabetes poses a significant economic burden on the healthcare system, families, and society as a whole. As a result, early risk factor identification and reduction for prediabetes and diabetes are important in effectively preventing and alleviating the disease burden.
There is substantial evidence indicating that obesity, especially in viscera, poses a substantial risk towards diabetes [8,9,10]. Within various methods used in assessing intra-abdominal fat, there are two most accurate methods for evaluating fat distribution, one is magnetic resonance imaging (MRI) and the other is computed tomography (CT), but their practical utility is constrained by high costs, time-intensive procedures, and the employment of ionizing radiation. Non-invasive and readily available measures, such as body mass index (BMI) and waist circumference (WC), offer limited information on visceral fat, body composition, and fat distribution [11, 12]. The body roundness index (BRI), a novel obesity metric that assesses the percentage of visceral and total body fat using WC and height, was first presented by Thomas et al. in 2013 [13]. BRI addresses the limitations of conventional indicators like BMI and WC [13]. Although earlier research has demonstrated the BRI’s potential to detect diabetes [14,15,16,17], there is currently no evidence linking the BRI to diabetes in Americans. Furthermore, prior studies have predominantly centered on diabetic patients, with limited investigations into prediabetic individuals. Therefore, the hypothesis of this study is that the BRI is significantly associated with both diabetes and prediabetes in a diverse American adult population. The novel aspect of this research lies in its focus on a large and representative sample of various ethnic groups among American adults, as well as its inclusion of prediabetic individuals, which has been underexplored in previous studies.
Considering this, this article intends to study the potential correlation between BRI and diabetes and prediabetes in a larger and more representative sample of various ethnic groups among American adults.
Methods
Research methodology and subjects
12 years of data (2007 to 2018) from the National Health and Nutrition Examination Survey (NHANES) were applied. As for the NHANES, a nationwide cross-sectional survey, evaluates the nutritional status as well as general health of noninstitutionalized individuals in the United States. It consisted of interviews, clinical assessments, and diagnostic tests. The design, methodologies, as well as data of the survey were made openly available through its website (http://www.cdc.gov/nchs/nhanes.htm). Every participant has given their written consent for the NHANES study, and the project has also received ethical approval [18]. Therefore, this study did not necessitate any specific approval or ethical review.
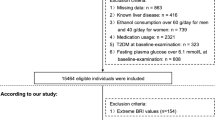
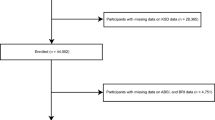
Out of the initial 59,842 participants recruited for the study, 25,072 individuals aged under 20 and 372 participants who were pregnant were not included in the analysis. Subsequently, individuals who missed BRI data (N = 3,397), incomplete diabetes information including diagnoses (N = 158), and absent covariates (N = 18,863) were sequentially excluded. The final analysis had 11,980 individuals in total (Fig. 1).

Flowchart of participant selection. Abbreviation NHANES: National Health and Nutrition Examination Surveys
Exposure variable and outcomes
Based on Diabetes Association Guidelines in 2023, according to at least one of the following conditions, an individual was identified as suffering from prodromal diabetes: the level of glycosylated haemoglobin (HbA1c) ranged between 5.7% and 6.4%, the range of the fasting blood glucose (FPG) was 5.6 mM to 7.0 mM, the 2-hour oral glucose tolerance test (OGTT) blood glucose level content ranged from 7.8 mM up to 11.1 mM, or obtained the clinical identification about prodromal diabetes from the health care provider [19]. Subjects were recognized to possess diabetes as long as individual up to grade one of the following conditions: an FPG level ≥ 7.0 mM, an HbA1c level ≥ 6.5%, the blood glucose content of random blood glucose or 2-hour OGTT of ≥ 11.1 mM, reported by a doctor diagnosing to prove diabetes, or taking oral hypoglycemic drugs or insulin [19]. BRI was calculated using 364.2-365.5*(1-[WC(m)/2π]2/[0.5*height(m)]2) ½ [13].
Covariates
The potential confounding factors of diabetes and prediabetes were selected based on previous studies, mainly including age, gender, race, degree of education, smoking status, alcohol use, marital status, poverty income ratio (PIR), physical activity, daily energy intake, BMI, WC, HbA1c, high density lipoprotein (HDL), total cholesterol (TC), hyperlipidemia, hypertension, cancer, and CVD. The smoking habits of participants were categorized into the following distinct types: never smoked, used to smoke, currently smoke. Participants’ drinking habits were assessed based on whether they drink a minimum of 12 glasses of various kinds of alcohol each year. Physical activity could be assessed by metabolic equivalent scores (METs) = sum of walking + moderate + vigorous MET [20]. The total daily energy intake (kcal) was computed based on the dietary recall data from the first day of 24-hour. HbA1c, HDL, and TC were measured using the NHANES laboratory protocol. Hyperlipidemia was evaluated by considering the use of lipid-lowering medications, a clinical diagnosis of hyperlipidemia, or laboratory results suggestive of elevated lipid levels [21]. The characteristics of hypertension included blood pressure ≥ 140/90 mmHg, a history of hypertension, or currently using antihypertensive drugs. The presence of cancer was determined through a positive answer this to issue, “Did a doctor inform you that you had cancer or a malignancy?” The criteria used to identify a history of CVD required a medically confirmed diagnosis of coronary artery disease or stroke.
Statistical analysis
In line with NHANES analysis guidelines, sample weights were applied to address the complexities of the sampling design. Chi-square tests were used to compare the percentages (%) that represented the categorical variables. Continuous variables were assessed using the Kruskal-Wallis H test, with results shown as mean values accompanied by standard deviations (SD). Multivariate logistic regression and univariate analysis were conducted to assess the potential correlation of BRI with diabetes and prediabetes. This study used three different models. While Model 2 had controls for age, race, and gender, Model 1 did not have any covariate adjustments. Covariates were included in Model 3 if they resulted in a greater than 10% change in the effect estimate. The possible relationship among BRI with diabetes and prediabetes was further analyzed by curve fitting. Subgroup analyses were conducted by age, gender, smoking status, alcohol use, marital status, PIR, physical activity, hypertension, hyperlipidemia, cancer, and CVD. Interaction P-values were utilized to assess the consistency of effects across subgroups. Finally, a comparison between BMI, a body shape index (ABSI), and WC was made in order to ascertain the diagnostic significance of the BRI in predicting diabetes and prediabetes using receiver operating characteristic (ROC) curve analysis. The P < 0.05 exhibited significance. EmpowerStates (www.empowerstats.com) was employed in whole statistical assessments.
Results
Participant characteristics
Out of a total of 11,980 individuals, there were 6,468 individuals diagnosed with diabetes (N = 2,090) and prediabetes (N = 4,378), while 5,512 individuals had normal blood glucose levels, as indicated in Table 1. Different from the group with normal blood glucose content, individuals within the group of diabetes and prediabetes were generally older, female, Mexican American, other Hispanic and non-Hispanic black, less educated, fewer never-married, were former smokers, non-drinkers, had lower family PIR, lacked physical activity, had lower daily energy intake, had lower HDL levels, and had significantly higher levels of BMI, WC, HbA1c, and BRI (P < 0.05). Moreover, they exhibited an increased risk of hyperlipidemia, hypertension, cancer, and CVD (P < 0.05).
Univariate analysis of diabetes and prediabetes
Table 2 displays a favourable correlation (P < 0.05) between age, daily energy intake, BMI, HbA1c, WC, and BRI with prediabetes and diabetes. Education level, physical activity, HDL were negatively related to diabetes and prediabetes (P < 0.05). When contrasted to males, females were at an elevated risk of diabetes development and prediabetes development. Non-Hispanic whites exhibited a reduced incidence of diabetes and prediabetes compared to Mexican Americans, while non-Hispanic blacks demonstrated an elevated risk. Being widowed/divorced/separated was at an elevated risk of diabetes and prediabetes than those who were being married/living with a partner. Individuals who were never married exhibited a decreased incidence of diabetes and prediabetes. Former smokers had an increased likelihood of developing diabetes and prediabetes compared to nonsmokers. Current alcohol drinkers showed a reduced risk of diabetes and prediabetes than non-drinkers. Individuals with a high PIR (> 3.5) had a lower incidence of diabetes and prediabetes than those with a low PIR (≤ 1.3). Moreover, diabetes and prediabetes were strongly correlated with hyperlipidemia, hypertension, malignancy, and CVD.
BRI level and diabetes and prediabetes
There was a marked positive relationship among BRI and diabetes and prediabetes in models 1, 2, and 3 (odds ratio [OR]: 1.17, 95% confidence intervals [CI]: 1.07–1.27). When BRI was categorized into quartiles, those who were in the top quartile (Q4: ≥ 6.40) demonstrated a significantly increased risk of diabetes and prediabetes development across models 1, 2, and 3 (OR: 1.83, 95% CI: 1.29–2.58) compared to the reference group (Q1: < 3.81). All P < 0.05 (as shown in Table 3). Furthermore, full adjustment of the smooth curve fitting revealed a nonlinear relationship existed in BRI with diabetes as well as prediabetes (P for non-linear = 0.01 < 0.05) (Fig. 2). As demonstrated in Table S1 and Figure S1, this investigation also identifies a non-linear positive association between BRI and prediabetes.

The non-linear relationship between BRI and incident of diabetes and prediabetes after adjusting for confound-ing variables
Subgroup analysis
In order to test the reliability of the link between the BRI and diabetes and prediabetes, further subgroup analyses were conducted. The findings study revealed that this positive relationship among BRI with diabetes and prediabetes could be observed across all subgroups (P < 0.05) (Fig. 3). Interactions terms were not significant in all subgroups (all P-values for interaction were > 0.05).

Subgroup analysis for the association between BRI and diabetes and prediabetes. Abbreviation BRI: body roundness index; CI: confidence interval; CVD: cardiovascular diseases; OR: odds ratio; PIR: poverty income ratio
BRI as a predictor for diabetes and prediabetes
Figure 4 shows the area under the curve (AUC) of diagnostic capability in the prediction of diabetes and prediabetes. These results revealed that both BMI, WC, ABSI, and BRI had statistically significant diagnostic capability for the detection of diabetes and prediabetes (AUC > 0.5) (Fig. 4). Furthermore, BRI performed better than BMI, ABSI, and WC indices (AUC = 0.68).

ROC curves for BMI, WC, ABSI, and BRI for predicting diabetes and prediabetes. Abbreviation ABSI: a body shape index; AUC: area under the curve; BMI: body mass index; BRI: body roundness index; ROC: receiver operating characteristic; WC: waist circumference
Discussion
This study is the first to merge and analyze data from the 2007–2018 NHANES for exploring the link between BRI values and being of diabetes and prediabetes within individuals in the USA. The statistical analysis shows a strong and stable positive correlation between BRI as well as the risk of both prediabetes and diabetes. This association remained consistent even after adjusting for confounding variables, suggesting that diabetes and prediabetes could be impacted by BRI. The likelihood of diabetes and prediabetes increased by 17% with each one-unit rise in BRI. Individuals with high BRI scores (Q4) exhibited greater odds of diabetes and prediabetes compared to those in the Q1 category. In this study, this was further by fund a non-linear relationship among BRI with diabetes and prediabetes. Furthermore, subgroup analysis and interaction assessments revealed that these consistent relationships were upheld across diverse population groups. Moreover, BRI exhibited the highest predictive value for diabetes and prediabetes compared to BMI, ABSI, and WC, as indicated by the largest AUC. Therefore, these results highly implied the latent availability of BRI acting to be the predictor for diabetes and prediabetes.
Obesity undoubtedly contributes significantly to the development of diabetes. Specifically, deposition of visceral organs of the abdomen with adipose tissue (abdominal obesity) exhibits a stronger correlation among insulin resistance and the threats of diabetes compared to subcutaneous fat [22, 23]. BMI is a commonly used indicator in diagnosing obesity, but it cannot fully reflect the actual body fat content [24], nor can it evaluate the risk of diseases associated with obesity in individuals possessing high body fat and low muscle mass [25]. Although WC is used as a diagnostic measure for identifying increased abdominal fat, it cannot distinguish between visceral fat and subcutaneous fat. Existing techniques for assessing abdominal fat through MRI or CT are expensive and require considerable time to perform, limiting their use in research and clinical settings. Consequently, the development and use of novel anthropometric indices have continued. Consequently, BRI is developed, and it has the ability to reflect body roundness related to height, and compared to traditional anthropometric indices, it can more accurately approximate visceral fat levels [13] and is highly correlated with visceral adipose tissue as assessed by CT imaging [26, 27].
The correlation between BRI level and diabetes is better than BMI, WC, and ABSI, as confirmed by a longitudinal study in Japan [16]. An investigation that was cross-sectional in the Northeast region of China also yielded similar conclusions [28]. Another retrospective cohort study found that BRI is more accurate than BMI in predicting diabetes [17]. A cohort study of 7,902 participants in China showed that BRI was significantly associated with diabetes among both sexes [14]. Zhang et al. [29] likewise found a favorable association between middle-aged and older Chinese individuals’ BRI levels with diabetes. Additionally, Zhao et al. [15] suggested that BRI displayed a positive correlation with diabetes risk in women and a curvilinear association in men. In terms of predicting diabetes in both sexes, BRI is superior to BMI and WC [15]. Nevertheless, the aforementioned studies had limited focus on the pre-disease stage of diabetes. A 4-year investigation carried out in Chinese adults revealed that a decrease in initial BRI levels was found to be correlated with a positive outcome of prediabetes regression, and its attributable fractions were around 20% [30]. However, among the population of Montenegro, there was no association between BRI and prediabetes [31]. For these inconsistent results, differences in race, subject characteristics, region, sample size, and study design may account for the differences between these studies. Additionally, it has not explored the connection among BRI with diabetes as well as prediabetes in the USA; therefore, this study validated the relationship among BRI to diabetes and prediabetes within American adults. Consistent with earlier findings in other populations, this study demonstrates that the BRI can be used as an indicator to evaluate risk factors for diabetes and prediabetes. Moreover, the consistent positive association between BRI and diabetes and prediabetes persisted across all subgroup analyses, underscoring the robustness of these results.
The following are a few plausible relationships that may explain the connection among BRI and diabetes and prediabetes. Initially, dysregulated lipid accumulation triggers endoplasmic reticulum stress and oxidative stress responses, leading to reduced gene expression, secretion, and increased apoptosis of pancreatic β-cells, culminating in β-cell dysfunction, resulting in reduced insulin sensitivity and secretion, which causes persistent hyperglycemia [32]. Additionally, elevated visceral fat levels reduce adiponectin (a protective adipokine) levels, leading to a rise in pro-inflammatory cytokines, including tumor necrosis factor and interleukin 6, potentially worsening insulin resistance [33]. Furthermore, compromised inhibition of lipolysis in adipocytes of individuals with obesity results in elevated levels of liver fatty acids, contributing to the accumulation of liver lipids. This process reduces liver insulin sensitivity, enhances hepatic gluconeogenesis, and ultimately results in dysglycemia [34].
Study the advantages and disadvantages
This study had two important advantages. Initially, the data was reliably analyzed to provide a good representation of the current state of the U.S. population. Secondly, the correlation between BRI and diabetes and prediabetes was consistent across various subgroup analyses, indicating the robustness of the findings. In spite of these important advantages, it also existed certain limitations that should not be overlooked. At first, based on a cross-sectional design, the study could not establish a causal connection among BRI with the development of diabetes and prediabetes. Furthermore, while this study accounted for potential confounders in the data analysis, residual confounding stemming from undisclosed or unmeasured variables may remain. Finally, this study population consisted of only American participants, so the generalizability of this study to other national populations is uncertain.
Conclusion
In this study, the increased BRI had a nonlinear positive association to the prevalence of diabetes and prediabetes among American adults. The predictive capacity of BRI outperformed that of BMI, ABSI, and WC. As a non-invasive and straightforward anthropometric tool, the BRI can offer clinicians a practical method to screen for prediabetes and diabetes in high-risk populations. Physicians should advise patients with higher BRI values to lead healthy lifestyles, which include eating a balanced diet and doing regular exercise, to manage their weight and abdominal fat and reduce their risk of developing prediabetes and diabetes.
Data availability
No datasets were generated or analysed during the current study. https://www.cdc.gov/nchs/nhanes.
Abbreviations
- ABSI:
-
A body shape index
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- BRI:
-
Body roundness index
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- CVD:
-
Cardiovascular diseases
- FPG:
-
Fasting blood glucose
- HDL:
-
High density lipoprotein
- HbA1c:
-
Glycosylated haemoglobin
- METs:
-
Metabolic equivalent scores
- MRI:
-
Magnetic resonance imaging
- NHANES:
-
The National Health and Nutrition Examination Survey
- OGTT:
-
Oral glucose tolerance test
- OR:
-
Odds ratio
- PIR:
-
Poverty income ratio
- ROC:
-
Receiver operating characteristic
- SD:
-
Standard deviations
- TC:
-
Total cholesterol
- WC:
-
Waist circumference
References
Ma RCW. Epidemiology of diabetes and diabetic complications in China. Diabetologia. 2018;61:1249–60.
Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–81.
Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379:2279–90.
Nguyen TT, Wang JJ, Wong TY. Retinal vascular changes in pre-diabetes and prehypertension: new findings and their research and clinical implications. Diabetes Care. 2007;30:2708–15.
Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953.
Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33:2285–93.
Echouffo-Tcheugui JB, Narayan KM, Weisman D, Golden SH, Jaar BG. Association between prediabetes and risk of chronic kidney disease: a systematic review and meta-analysis. Diabet Med. 2016;33:1615–24.
Lebovitz HE, Banerji MA. Point: visceral adiposity is causally related to insulin resistance. Diabetes Care. 2005;28:2322–5.
Wander PL, Boyko EJ, Leonetti DL, McNeely MJ, Kahn SE, Fujimoto WY. Change in visceral adiposity independently predicts a greater risk of developing type 2 diabetes over 10 years in Japanese americans. Diabetes Care. 2013;36:289–93.
Neeland IJ, Turer AT, Ayers CR, Powell-Wiley TM, Vega GL, Farzaneh-Far R, et al. Dysfunctional adiposity and the risk of prediabetes and type 2 diabetes in obese adults. JAMA. 2012;308:1150–9.
Müller MJ, Lagerpusch M, Enderle J, Schautz B, Heller M, Bosy-Westphal A. Beyond the body mass index: tracking body composition in the pathogenesis of obesity and the metabolic syndrome. Obes Rev. 2012;2:6–13.
Busetto L, Baggio MB, Zurlo F, Carraro R, Digito M, Enzi G. Assessment of abdominal fat distribution in obese patients: anthropometry versus computerized tomography. Int J Obes Relat Metab Disord. 1992;16:731–6.
Thomas DM, Bredlau C, Bosy-Westphal A, Mueller M, Shen W, Gallagher D, et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity. 2013;21:2264–71.
Wang Y, Zhang X, Li Y, Gui J, Mei Y, Yang X, et al. Obesity- and lipid-related indices as a predictor of type 2 diabetes in a national cohort study. Front Endocrinol. 2024;14:1331739.
Zhao W, Tong J, Li J, Cao Y. Relationship between body roundness index and risk of type 2 diabetes in Japanese men and women: a reanalysis of a Cohort Study. Int J Endocrinol. 2021;29:4535983.
Wu L, Pu H, Zhang M, Hu H, Wan Q. Non-linear relationship between the body roundness index and incident type 2 diabetes in Japan: a secondary retrospective analysis. J Transl Med. 2022;20:110.
Yang T, Zhao B, Pei D. Evaluation of the Association between Obesity Markers and type 2 diabetes: a Cohort Study based on a physical examination Population. J Diabetes Res. 2021;2021:6503339.
NHANES - NCHS Research Ethics Review Board Approval. https://www.cdc.gov/nchs/nhanes/irba98.htm (2022).
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. Classification and diagnosis of diabetes: standards of Care in Diabetes-2023. Diabetes Care. 2023;46:S19–40.
Murray JM, Coleman HG, Hunter RF. Physical activity and cancer risk: findings from the UK Biobank, a large prospective cohort study. Cancer Epidemiol. 2020;68:101780.
National Cholesterol Education Program (NCEP). Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421.
Westphal SA. Obesity, abdominal obesity, and insulin resistance. Clin Cornerstone. 2008;9:23–9.
Casanueva FF, Moreno B, Rodríguez-Azeredo R, Massien C, Conthe P, Formiguera X, et al. Relationship of abdominal obesity with cardiovascular disease, diabetes and hyperlipidemia in Spain. Clin Endocrinol. 2010;73:35–40.
Lavie CJ, De Schutter A, Patel D, Artham SM, Milani RV. Body composition and coronary heart disease mortality—an obesity or a lean paradox? Mayo Clin Proc. 2011;86:857–64.
Thibault R, Pichard C. The evaluation of body composition: a useful tool for clinical practice. Ann Nutr Metab. 2012;60:6–16.
Li G, Yao T, Wu XW, Cao Z, Tu YC, Ma Y, et al. Novel and traditional anthropometric indices for identifying arterial stiffness in overweight and obese adults. Clin Nutr. 2020;39:893–900.
Ishida A, Taira H, Shinzato T, Ohya Y. Association between visceral fat mass and arterial stiffness among community-based screening participants. Hypertens Res. 2023;46:2488–96.
Chang Y, Guo X, Chen Y, Guo L, Li Z, Yu S, et al. A body shape index and body roundness index: two new body indices to identify diabetes mellitus among rural populations in northeast China. BMC Public Health. 2015;15:794.
Zhang X, Wang Y, Li Y, Gui J, Mei Y, Yang X, et al. Optimal obesity- and lipid-related indices for predicting type 2 diabetes in middle-aged and elderly Chinese. Sci Rep. 2024;14:10901.
Yang H, Zhang M, Nie J, Zhang M, Lu G, Chen R, et al. Associations of obesity-related indices with prediabetes regression to normoglycemia among Chinese middle-aged and older adults: a prospective study. Front Nutr. 2023;10:1075225.
Klisic A, Radoman Vujačić I, Kostadinovic J, Patoulias D, Ninic A. Novel anthropometric parameters in the adult population with prediabetes. Eur Rev Med Pharmacol Sci. 2023;27:11063–72.
Wagner R, Eckstein SS, Yamazaki H, Gerst F, Machann J, Jaghutriz BA, et al. Metabolic implications of pancreatic fat accumulation. Nat Rev Endocrinol. 2022;18:43–54.
Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol. 2011;11:85–97.
Perry RJ, Samuel VT, Petersen KF, Shulman GI. The role of hepatic lipids in hepatic insulin resistance and type 2 diabetes. Nature. 2014;510:84–91.
Funding
This study was supported by the Natural Science Foundation of Hunan Province (2024JJ5309), Hunan University of Traditional Chinese Medicine collaborate Hunan Zhonghe Dahan Health Industry Operation and Management Foundation Focused Projects (020000202917).
Author information
Authors and Affiliations
Contributions
LQ: article conception, methodology, software, and writing-original draft. ZX: analysis, review, and data integration. BF: methodology and software. LL: review and methodological guidance. GS: writing review and editing, and methodology. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This investigation was approved by the National Center for Health Statistics. Ethics Review Board. Informed consent was obtained from all subjects involved in the NHANES.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qiu, L., Xiao, Z., Fan, B. et al. Association of body roundness index with diabetes and prediabetes in US adults from NHANES 2007–2018: a cross-sectional study. Lipids Health Dis 23, 252 (2024). https://doi.org/10.1186/s12944-024-02238-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02238-2