
Abstract
Background
Despite India being one of the largest contributors to the measles burden, crucial epidemiological information is significantly lacking. We have analyzed the national-level representative data between 2011 and 2020 to estimate the national- and state-level incidence, first dose vaccine coverage, and mortality; and developed a prediction model to examine the trend of the disease.
Methods
We extracted the Health Management Information System (HMIS) for monthly aggregated measles cases, deaths, and child immunization (9–11 months) for first dose measles vaccine coverage across all states & Union Territories (UT). Population information & projections were extracted based on Census 2011. A multilevel fixed effect panel data model was used to predict measles incidence rate, assuming measles vaccination coverage as a predictor while accounting for time fixed effects.
Results
Total 558,536 measles cases and 4209 measles deaths were reported in India between 2010 and 2020. The incidence rate was highest in 2013 (628.8/million population), followed by a significant decline to reach 52.0/million in 2020. Measles vaccination coverage for the first dose was 84.1% in 2011 to 91.3% in 2019. Higher vaccination coverage was significantly correlated (r = 0.7, p = 0.02) with decline of measles incidence rate. The case fatality rate (CFR) was least in 2014 (0.13%) but upsurged consistently reaching to 3.3% in 2020. The predictive model indicates that with a first-dose vaccine coverage of 93.5%, and keeping other factors constant, the national measles incidence is projected to reach zero by 2025.
Conclusion
Measles incidence is declining in India due to higher vaccination coverage, yet the rise in death rates emphasizes the need for continued collaborative efforts to achieve a measles-free nation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The global strategy for measles elimination has faced setbacks, with persistent challenges hindering its success [1, 2]. The resurgence of measles in recent years highlights the fragility of elimination efforts [3,4,5,6]. First, vaccine coverage gaps exist, leading to pockets of susceptible populations, which facilitates measles transmission [7]. Additionally, weak healthcare infrastructure in some regions limits effective vaccine delivery and surveillance [8]. Furthermore, vaccine hesitancy and misinformation contribute to suboptimal immunization rates, impeding the achievement of herd immunity [9].
Globally, measles was a prominent cause of childhood mortality, claiming over 2 million lives annually prior to the introduction of the measles vaccine [10]. The period from 2000 to 2016 witnessed a significant decline in measles incidence and mortality by 88% and 84%, respectively, attributed to increased vaccination rates [11]. However, since 2016, a resurgence of measles has emerged worldwide due to insufficient vaccination campaigns and policy initiatives in numerous countries [12]. By the close of 2019, none of the WHO regions had managed to maintain measles elimination successfully. In 2019, the African region exhibited the highest measles incidence at 567 cases per 1 million population, followed by the European region with 116 cases per 1 million population [11].
The measles burden and mortality related information is often unreliable due to insufficient data from high-burden settings [7, 13, 14]. Estimating the precise burden and mortality is critical to strengthen health systems and assess vaccination program effectiveness. Analysis based on the global burden of disease suggests that the incidence of measles has fallen considerably in the last three decades, but the infection burden and mortality (expressed as case fatality rate or CFR) has predominantly been concentrated to a few areas in the Sub-Saharan Africa and South Asia [14, 15]. However, the incidence and mortality data are often criticized because of data insufficiency, and thereby largely underestimating the burden. Moreover, the mortality data is confined to specific contexts, populations, and time [16,17,18]. On the top of that, inadequate data on vaccination coverage makes the situation even difficult for policy decisions.
India contributes significantly to the global burden of measles infection [15, 19]. Though enhanced vaccination drive has clearly reduced measles death significantly since 2000, [20] reportedly, India alone contributes half of the global death due to the infection among the under-five children [1, 21]. In response to the global drive for measles eradication, India has introduced the second dose of measles containing vaccine (MCV) in the routine immunization schedule and supplementary immunization activity (SIA) to enhance the MCV coverage in the target population [22, 23]. Use of existing surveillance data is critical for policy decisions at the country level [15]. Unfortunately, a national- and sub-national-level data on measles epidemiology is lacking to understand the current status of the infection control in the country. While outbreaks are reported through the national-level surveillance system called Integrated Disease Surveillance Programme (IDSP), the number of measles cases and deaths are reported through the Health Management and Information System (HMIS). IDSP is often criticized for its lack of validity [24]. In this study, we have analyzed the HMIS data between 2011 and 2020 to estimate the national- and state-level incidence, mortality, and first dose vaccine coverage of measles in India. We have also developed a prediction model to examine the trend of the disease.
2 Methods
We extracted the publicly available HMIS data for monthly aggregated measles cases, deaths, and child immunization (9–11 months) with the first dose of measles vaccine (or measles containing vaccine like MR/MMR) across all states (28 in number) and the Union Territories (UT) (8 in number) from 2011 to 2020 [25].
The HMIS is a web-based monitoring system established by the Indian Ministry of Health & Family Welfare. It monitors the key indicators of various national health programs, offering crucial insights for policy development and program interventions. It collects monthly data on service delivery like maternal and child health related, immunisation family planning, quarterly training information, and annual infrastructure data from health facilities, enabling gap analysis and evidence-based corrections. The HMIS portal facilitates data flow and generates periodic reports on health service and resource status. The data utilized in this research was obtained from the HMIS and encompassed monthly records of measles cases and deaths of children below five years, and first dose of measles vaccine (or measles containing vaccine like MR/MMR) on child 9–11 months for states/union territories (UTs) during the period from 2011 to 2020 which is publicly available [25]. Data for Lakshadweep was available but recorded the zero measles cases, while the data for Dadra and Nagar Haveli (DNH) and Daman and Diu (DD) was combined, while data for Ladakh was only available for the year 2020.
To assess measles vaccination coverage and incidence rates, we relied on population data specific to infants for coverage and children aged 0–5 years for incidence rates. Population information was extracted from the Census 2011 and projected populations for 2019, provided by the National Commission of Population, Ministry of Health & Family Welfare, Government of India. We projected population figures for each state from 2011 to 2020, assuming a consistent annual state-specific growth rate. Based on the available age-wise population data for each state, we calculated the proportions for the target age groups. These proportions helped estimating age-specific populations of each state between 2011 and 2020 after applying state-specific growth rate. Age-standardization was applied to these rates to account for any variations in age distributions across states and over time.
To ensure that vaccine coverage is realistically represented among the target population in this analysis, we verified the vaccination coverage from other data sources including immunization data under the National Health Mission (NHM), and universal immunization coverage data, to rule out any major variations in the coverage. On examination, we found that the other sources had several limitations like difficulty in extracting the target population coverage, non-reporting of state-level coverage, and unreliable figures (e.g. MCV1 coverage > 100%).
In this study, our primary focus was on measuring measles incidence, which represents the number of measles cases per million population of children under five years of age. Measles incidence was calculated by taking the monthly aggregated data on measles cases obtained from HMIS and dividing it by the estimated children under five years population in each state for each year.
CFR was determined by dividing the monthly aggregated data on measles-related deaths by the monthly measles cases in each state for each year. The final variable of interest was the coverage of the first dose of measles-containing vaccine (MCV1), recommended for children aged 9 to 11 months. To calculate this coverage, we used the same HMIS data to observe the number of vaccinated children and paired it with population estimate data. This coverage was computed by dividing the total number of vaccinated children by the total infant population in each state for each year.
Data collected from HMIS encompassed the following elements: number of measles cases reported among children under five years old, number of deaths in children aged one month to five years, where measles was a cause, and the number of infants who received their first measles immunization dose.
We performed data cleaning and validation on the database and identified 56 cell observations with incorrect entries, where the number of deaths exceeded the number of reported measles cases. Consequently, we removed these observations from the final analysis. Next, we aggregated the monthly data into annual data to facilitate trend analysis. We computed annual incidence rates per million, CFR, and measles vaccination coverage using this consolidated information, in conjunction with population estimates.
Statistical analyses in this study were conducted utilizing the Stata 14 statistical software. Categorical variables were presented as frequencies and percentages, while quantitative variables were expressed as the median along with the interquartile range (IQR). We conducted analyses at both the national and state levels. To visualize trends, we generated a trend plot with a bar graph displaying annual incidence rates and vaccination coverage. The Pearson correlation coefficient (r) was calculated to assess the relationship between the incidence rate and vaccination coverage. Additionally, we developed a multilevel fixed effect panel data model to estimate the measles incidence rate, using measles vaccination coverage as a predictor while accounting for time fixed effects. The incidence rate was calculated using the following equation:
where yit represents the measles incidence per million child population (0–5 years age group) in zone i at time t and xi,t−j denotes the MCV in the ith state at time t−j, with j varies the dependence on coverage over the past five years because vaccine coverage was reported in HMIS for infants (< 1 years) only. The coefficient βj indicates the impact of vaccine coverage at different time lags (up to five years) on measles incidence. The other variables in the model represent the following:
αi: State-specific intercept term accounting for unobservable time-invariant characteristics within each state.
γt: Time fixed effects capturing the overall trend of measles incidence over time.
μi: Random state-specific effects capturing unobservable factors that influence measles incidence but are constant over time.
εit: Error term representing unexplained variation in measles incidence not accounted for by the model.
By incorporating the lagged variable of vaccination coverage and its estimation, we were able to determine the impact of vaccination coverage on measles incidence rates. Furthermore, we included dummy variables in our analysis to account for any additional unobservable time-invariant characteristics within each state that could influence measles incidence. To ensure the accuracy and validity of our model, we conducted several checks. We first assessed the model’s fit using statistical measures such as the coefficient of determination (R2), Akaike information criterion (AIC) and Bayesian information criterion (BIC). Additionally, we performed diagnostic tests to examine the residuals for patterns or outliers, ensuring that the model assumptions were met. Statistical significance was considered when p-values were less than 0.05.
3 Results
The number of children aged 0 to 5 years was 138,658,432 in 2011 in India. A total number of 558,536 measles cases and 4209 measles deaths were reported in HMIS between 2011 and 2020 for children aged 0 to 5 years. The median number of measles cases and deaths were 66,621 (IQR 35,014 to 77,082) and 310 (IQR 136 to 1225), respectively. Despite an initial surge from 2011, the number of cases declined consistently since 2014 (Table 1). On the contrary, the number of deaths has shown inconsistent changes during this period (Table 1).
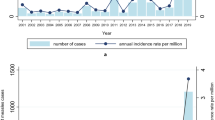
The incidence rate per million children population aged 0 to 5 years was highest (628.8) in 2013, followed by a significant decline, thereafter, reaching to 52.0 in 2020. This gives a reduction in incidence for children aged 0 to 5 years by 10 times during this period (Fig. 1). In 2011, the CFR was 0.67% which showed a considerable declining pattern till 2014 (0.12%), the rate has since shown a sharp upsurge reaching to 3.68% in 2020 (Table 1). Conversely, the measles vaccination coverage in infant children for the first dose showed a gradual increase from 84.1% in 2011 to 91.3% in 2019. However, the coverage estimate declined to 86.3% in 2020, the COVID-19 pandemic period. Higher vaccination coverage was significantly correlated (r = 0.7, p = 0.02) with the decrease in the measles incidence rate per million children population aged 0 to 5 years (Fig. 1).

Annual incidence rate per million children population aged 0 to 5 years of measles and measles vaccination coverage between 2011 and 2020, India
During these 10 years, the annual incidence of measles among children aged 0 to 5 years has significantly declined in all the states and UTs (Fig. 2). The north-eastern states such as Sikkim, Arunachal Pradesh, and Mizoram witnessed a notably high annual measles incidence per million children population aged 0 to 5 years. With varying fluctuations up to 2017, the incidence decreased significantly in 2020. Unlike the north-Eastern states, the decline in the incidence in the other regions was relatively consistent. In 2020, the highest incidence was noticed in the states of Mizoram (569.8/million) and West Bengal (251.2/million) (Fig. 2).

Annual incidence rate of measles among children aged 0–5 years in State/UT wise between 2011 and 2020, India
Measles vaccination coverage under infant has remained persistently low in North–East region. While the coverage in the other regions has been improved gradually throughout this period, a slight downward trend has been noticed in the year 2020, the COVID pandemic time (Fig. 3). Some remarkable improvement has been noticed in the states/UTs like Nagaland, Arunachal Pradesh and Jammu & Kashmir. The states/UTs with lowest vaccination coverage in 2020 include- Manipur, Meghalaya, and Arunachal Pradesh.

Measles vaccination coverage among infants in State/UT wise between 2011 and 2020, India
The national level increasing pattern of CFR has been reflected in a majority of the states and UTs. The upsurge is remarkable since 2017 (Fig. 4). Unlike the distribution of incidence, the CFR is comparatively less in the North-East states. Noticeably, the states with high CFR are more concentrated in the northern region. For example, the state Haryana had a persistently high CFR during this period. In 2020, high CFR was noticed in the states of Bihar (18.2%), Haryana (16.2%), Madhya Pradesh (14.9%), Karnataka (14.9%), and Himachal Pradesh (11.8%).

Case fatality rate of measles among children ages 0–5 years in State/UT wise between 2011 and 2020, India
Table 2 summarizes the findings of a panel data analysis that explores the association between measles vaccination coverage over the preceding five years and the incidence of measles cases per million children population under five years of age. The coefficients (β) in the table represent the estimated effect of a one-unit change in measles vaccination coverage on the incidence of measles, accounting for different model specifications and holding other variables constant. For example, β1 in the fixed effect model with only a time effect suggests that a one-unit increase in vaccination coverage is associated with a decrease of 9.1 measles cases per million children 0–5 years population, though this effect is not statistically significant. Overall, the results suggested a negative association, i.e., a one per cent increase in measles vaccination coverage during the past five years is linked to a corresponding decrease in measles incidence. The random effect model suggests smaller effects of vaccination coverage on measles incidence compared to the fixed effect model, indicating that some of the variation may be explained by unobserved factors specific to each state. The R-squared values indicate the proportion of variance in measles incidence explained by the model. A higher R-squared value suggests that the model with both time and geographic effects (random effect model) explains more of the variance in measles incidence compared to the other models. Based on this estimated model, if current measles prevention strategies and a vaccination rate of 93.5% are maintained in the upcoming years, the national measles incidence is predicted to reach zero by 2025. However, this prediction is based on the assumption that vaccination coverage remains constant and other factors influencing measles transmission remain unchanged.
4 Discussion
In this paper, we have estimated the national- and state-level incidence of measles and the CFR due to the disease among the children below five years of age from 2011 to 2020. We have also provided the first dose vaccination coverage for infants during this period. Our analysis suggests that the measles incidence has decreased substantially over this time; however, the death rate has increased alarmingly in the recent past, though not related to the vaccine coverage, unlike measles incidence. It is expected that a sustained coverage of MCV above 93.5% can cease measles incidence to zero.
Globally, the prevalence of measles manifested a consistent downturn from 1990 to 2019, with documented cases diminishing from 80 to 12 million. The Annual Standardized Rate (ASR) of measles infection exhibited an annual decline of 6.13%, ranging from 1278.81 per 100,000 in 1990 to 191.04 per 100,000 in 2019. Notably, the ASR underwent a substantial reduction between 1995 and 2015, with marginal decreases observed from 1990 to 1995 and from 2015 to 2019 [2, 13]. While overall trends showed improvement, regional disparities were evident. Regions with high incidence rates are predominantly concentrated in Sub-Sharan Africa, South Asia, and South-east Asia characterized by low socio-demographic indices and vaccine coverage [13, 26]. Throughout 1990 to 2019, children under the age of 5 emerged as the predominant demographic cohort, constituting a minimum of 80% of total cases. The proportion attributed to this age group demonstrated a general decline from 1990 to 2017, followed by an increase post-2017 [13]. In Asia, countries like India, and China recorded significant numbers of measles cases in 2019, contributing 19.84%, and 6.83%, respectively to the global burden [13]. Our analysis reveals a sustained declining trend in measles incidence in the Indian context since 2013, with rates below the global average of 191/100,000 in 2019. It is imperative to note that this analysis exclusively pertains to under-five children, and thus, the overall incidence may be slightly higher. Nonetheless, the national average was reflected in all states and Union Territories, exhibiting some fluctuations in specific pockets. The Eastern and North-Eastern regions of the country continue to experience higher incidence rates compared to other regions.
The administration of MCV through routine immunization has proven instrumental in the control and prevention of measles, boasting an impressive 97% effectiveness in preventing the disease and establishing MCV as one of the most efficacious vaccines developed to date. Over the period from 2000 to 2019, global coverage for the routine MCV1 increased from 72 to 85%, and the count of countries achieving ≥ 90% MCV1 coverage rose from 86 (45%) to 122 (63%) [27]. Given the highly contagious nature of measles, maintaining high (≥ 95%) coverage for the recommended two doses of MCV is critical for effective measles control and achieving elimination. However, the plateauing of global MCV coverage over nearly a decade, coupled with the global resurgence of measles in 2018–2019, underscores the need for sustained efforts.
While India initiated the second dose of measles vaccination in 2010, comprehensive data on vaccine coverage at lower administrative levels remains elusive. State-level analysis reveals a consistent first-dose coverage ranging between 85 and 90% over the past 5 years, with uncertainty surrounding the coverage for the second dose. Encouragingly, vaccine coverage has exhibited a steady increase since 2011, with a minor dip during the COVID-19 pandemic. Despite substantial progress in first-dose coverage at the state level over the past decade, focused efforts are imperative in the North-Eastern states, where coverage is comparatively lower, resulting in a higher incidence of cases.
Measles CFR exhibit considerable variation, influenced by factors such as access to quality healthcare, nutritional status, and overall health conditions [13, 28,29,30]. In high-income countries like the United States, CFRs can be as minimal as 0.1% or even lower, while in other contexts, particularly in Africa, they may escalate to 4%–5%, reaching as high as 30% in vulnerable children during humanitarian crises [14]. A comprehensive systematic review reveals a global halving of CFRs, decreasing from 2.6% in 1990 to 1.32% in 2019, with South Asia achieving a notable decline from 3.16% to 0.82%, marking a substantial achievement in reducing measles-related mortality [31]. However, contrasting with this trend, the present analysis identifies a significant increase in CFRs across the country and all regions, irrespective of vaccine coverage. The present finding contradicts the earlier evidence that measles death is proportionate to the disease [21]. Severe measles and associated fatalities can be attributed to various factors, notably infants with low levels of maternal antibodies, the presence of undernutrition, and deficiencies in health system quality and access [32,33,34].
Given the findings from our study and the global context, India must focus on enhancing measles vaccination coverage especially in low-coverage pockets and where incidence rates remain high. Moreover, the increase in measles CFR, despite high vaccination coverage, suggests underlying health system challenges that require immediate attention. Strengthening health infrastructure, improving access to quality healthcare, and addressing nutritional deficiencies are crucial for reducing mortality associated with measles.
Limitations: We expect an under-reporting of the measles cases and death as the coverage of the HMIS data for the private sector is unclear; and hence, both incidence and CFR is also expected to be under-estimated than the actual value. The incidence is also expected to alter marginally as we have assumed a fixed growth rate to project the populations. Our analysis was constrained up to early 2020 due to data unavailability during the COVID-19 pandemic. Due to unavailability of the state-level data, we could not extend our analysis to include age groups beyond five years, MCV2, and SIA. Nevertheless, the present paper provides with a valuable insight on measles till pre-COVID-period to understand the disease epidemiology. Finally, our model cannot explain the complexities around the herd immunity due to vaccine coverage.
5 Conclusion
In conclusion, our analysis reveals a declining trend in measles cases since 2014 in India, highlighting the impact of vaccination. However, fluctuating deaths and an abrupt increase in mortality underscore persistent challenges in the nation. National and state-level commitments to enhance immunization access, bolster public health infrastructure, and implement innovations are crucial for a measles-free nation. Sustained efforts and collaboration from stakeholders are imperative to achieve and maintain optimal measles vaccination rates in India.
Data availability
Data can be made available on reasonable request to the corresponding author.
Code availability
Code for data analysis can be made available on reasonable request to the corresponding author.
References
Simons E, Ferrari M, Fricks J, Wannemuehler K, Anand A, Burton A, et al. Assessment of the 2010 global measles mortality reduction goal: results from a model of surveillance data. Lancet. 2012;379(9832):2173–8.
Gastañaduy PA, Goodson JL, Panagiotakopoulos L, Rota PA, Orenstein WA, Patel M. Measles in the 21st century: progress toward achieving and sustaining elimination. J Infect Dis. 2021;224(Suppl 4):S420–8.
Feemster KA, Szipszky C. Resurgence of measles in the United States: how did we get here? Curr Opin Pediatr. 2020;32(1):139.
Suvvari TK, Kandi V, Mohapatra RK, Chopra H, Islam MdA, Dhama K. The re-emergence of measles is posing an imminent global threat owing to decline in its vaccination rates amid COVID-19 pandemic a special focus on recent outbreak in India – a call for massive vaccination drive to be enhanced at global level. Int J Surg. 2023. https://doi.org/10.1097/JS9.0000000000000228.
Abad CL, Safdar N. The reemergence of measles. Curr Infect Dis Rep. 2015;17(12):51.
Ilyas M, Afzal S, Ahmad J, Alghamdi S, Khurram M. The resurgence of measles infection and its associated complications in early childhood at a tertiary care hospital in peshawar. Pakistan Pol J Microbiol. 2020;69(2):177–84.
Patel MK, Antoni S, Nedelec Y, Sodha S, Menning L, Ogbuanu IU, et al. The changing global epidemiology of measles, 2013–2018. J Infect Dis. 2020;222(7):1117–28.
Cheng M, Lan T, Geater A, Deng QY, Lin YD, Jiang LY, et al. Health system barriers to timely routine measles vaccinations in rural southwest china: a qualitative study on the perspectives of township vaccination professionals and village doctors. BMJ Open. 2023;13(11): e072990.
Venkatesan P. Worrying global decline in measles immunisation. The Lancet Microbe. 2022;3(1): e9.
Moss WJ. Measles. Lancet. 2017;390(10111):2490–502.
Patel MK, Goodson JL, Alexander JP, Kretsinger K, Sodha SV, Steulet C, et al. Progress toward regional measles elimination—worldwide, 2000–2019. MMWR Morb Mortal Wkly Rep. 2020;69(45):1700–5.
Patel MK, Dumolard L, Nedelec Y, Sodha SV, Steulet C, Gacic-Dobo M, et al. Progress toward regional measles elimination—worldwide, 2000–2018. MMWR Morb Mortal Wkly Rep. 2019;68(48):1105–11.
Wang R, Jing W, Liu M, Liu J. Trends of the global, regional, and national incidence of measles, vaccine coverage, and risk factors in 204 countries from 1990 to 2019. Front Med (Lausanne). 2022;20(8): 798031.
Sbarra AN, Mosser JF, Jit M, Ferrari M, Ramshaw RE, O’Connor P, et al. Estimating national-level measles case–fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study. Lancet Glob Health. 2023;11(4):e516–24.
Dabbagh A, Patel MK, Dumolard L, Gacic-Dobo M, Mulders MN, Okwo-Bele JM, et al. Progress toward regional measles elimination—worldwide, 2000–2016. MMWR Morb Mortal Wkly Rep. 2017;66(42):1148–53.
Wolfson LJ, Grais RF, Luquero FJ, Birmingham ME, Strebel PM. Estimates of measles case fatality ratios: a comprehensive review of community-based studies. Int J Epidemiol. 2009;38(1):192–205.
Portnoy A, Jit M, Ferrari M, Hanson M, Brenzel L, Verguet S. Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(4):e472–81.
Portnoy A, Hsieh YL, Abbas K, Klepac P, Santos H, Brenzel L, et al. Differential health impact of intervention programs for time-varying disease risk: a measles vaccination modeling study. BMC Med. 2022;20(1):113.
Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375(9730):1969–87.
Wong BK, Fadel SA, Awasthi S, Khera A, Kumar R, Menon G, et al. The impact of measles immunization campaigns in India using a nationally representative sample of 27,000 child deaths. ELife. 2019. https://doi.org/10.7554/eLife.43290.
Morris SK, Awasthi S, Kumar R, Shet A, Khera A, Nakhaee F, et al. Measles mortality in high and low burden districts of India: estimates from a nationally representative study of over 12,000 child deaths. Vaccine. 2013;31(41):4655–61.
Johri M, Sharma JK, Jit M, Verguet S. Use of measles supplemental immunization activities (SIAs) as a delivery platform for other maternal and child health interventions: opportunities and challenges. Vaccine. 2013;31(9):1259–63.
Auzenbergs M, Fu H, Abbas K, Procter SR, Cutts FT, Jit M. Health effects of routine measles vaccination and supplementary immunisation activities in 14 high-burden countries: a dynamic measles immunization calculation engine (dynaMICE) modelling study. Lancet Glob Health. 2023;11(8):e1194–204.
Goel K, Chaudhuri S, Saxena A. India’s strategy on surveillance system-a paradigm shift from an integrated disease surveillance programme (IDSP) to an integrated health information platform (IHIP). Clin Epidemiol Glob Health. 2022. https://doi.org/10.1016/j.cegh.2022.101030.
Government of India. HMIS-Health Management Information System https://hmis.mohfw.gov.in/#!/standardReports. Accessed 2 May 2024
Sato R, Makinde OA, Daam KC, Lawal B. Geographical and time trends of measles incidence and measles vaccination coverage and their correlation in Nigeria. Hum Vaccin Immunother. 2022;18(6):2114697.
Institute for Health Metrics and Evaluation. Global Health Data Exchange (GHDx. https://ghdx.healthdata.org/. Accessed 17 Jan 2024
Paules CI, Marston HD, Fauci AS. Measles in 2019 - going backward. N Engl J Med. 2019;380(23):2185–7.
Chovatiya R, Silverberg JI. Inpatient morbidity and mortality of measles in the United States. PLoS ONE. 2020;15(4): e0231329.
Donadel M, Stanescu A, Pistol A, Stewart B, Butu C, Jankovic D, et al. Risk factors for measles deaths among children during a nationwide measles outbreak—Romania, 2016–2018. BMC Infect Dis. 2021;19(21):279.
Sbarra AN, Rolfe S, Nguyen JQ, Earl L, Galles NC, Marks A, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature. 2021;589(7842):415–9.
Roberts L. Polio, measles, other diseases set to surge as COVID-19 forces suspension of vaccination campaigns https://www.science.org/content/article/polio-measles-other-diseases-set-surge-covid-19-forces-suspension-vaccination-campaigns. Accessed 17 Jan 2024
Takahashi S, Metcalf CJE, Ferrari MJ, Tatem AJ, Lessler J. The geography of measles vaccination in the African great lakes region. Nat Commun. 2017;25(8):15585.
Kundrick A, Huang Z, Carran S, Kagoli M, Grais RF, Hurtado N, et al. Sub-national variation in measles vaccine coverage and outbreak risk: a case study from a 2010 outbreak in Malawi. BMC Public Health. 2018;18(1):741.
Acknowledgements
Nil.
Funding
Not available.
Author information
Authors and Affiliations
Contributions
VA has contributed to designing the study, acquisition of data, analysis of data, revision of the draft, approved the version to be published, and agreed to be accountable for all aspects of the work. SC has contributed to designing the study, analysis of data, and interpretation of analysis, drafting manuscript, revision of the version to be published, and agreed to be accountable for all aspects of the work. MVK has contributed to designing the study, interpretation of data, drafting manuscript, revision of draft and approved the version to be published, and agreed to be accountable for all aspects of the work. PVY has contributed to designing the study, interpretation of data, drafting manuscript, revision of draft and approved the version to be published, and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Agiwal, V., Chaudhuri, S., Kumar, M.V. et al. Decadal analysis of measles epidemiological data in India (2011–2020). Discov Public Health 21, 4 (2024). https://doi.org/10.1186/s12982-024-00125-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12982-024-00125-w