
Abstract
Background (Rationale/Purpose/Objective)
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is used to temporary control non-compressible truncal hemorrhage (NCTH) as bridge to definitive surgical treatment. The dependence on radiography for safe balloon positioning is one factor that limits the extended use of REBOA in civilian and military pre-hospital settings. We aimed to determine standardized sex and age-based variable-distance catheter insertion lengths for accurate REBOA placement without initial fluoroscopic confirmation.
Methods
Contrast enhanced CT-scans from a representative sample of a Dutch non-trauma population were retrospectively analyzed. Intravascular distances were measured from the bilateral common femoral artery access points (FAAP) to the middle of the aortic occlusion zones and accompanying boundaries. Means and 95% confidence intervals for the distances from the FAAPs to the boundaries and mid-zone III were calculated for all (combined) sex and age-based subgroups. Optimal insertion lengths and potentially safe regions were determined for these groups. Bootstrap analysis was performed in combination with a 40-mm long balloon introduction simulation to determine error-rates and REBOA placement accuracy for the general population.
Results
In total, 1354 non-trauma patients (694 females) were included. Vascular distances increased with age and were longer in males. The iliofemoral trajectory was 7 mm longer on the right side. The optimal zone I catheter insertion length would be 430 mm. Optimal zone III catheter insertion lengths showed up to 30 mm difference, ranging between 234 and 264 mm. Statistically significant and potentially clinically relevant differences were observed between the anatomical distances and necessary introduction depths for each subgroup.
Conclusion
This is the first study to compare aortic morphology and intravascular distances between combined sex and age-based subgroups. As zone III length was consistent, length variability and elongation seem to mainly originate in the iliofemoral trajectory and zone II. The optimal zone I catheter insertion length would be 430 mm. Optimal zone III catheter insertion ranged between 234 and 264 mm. These standardized variable-distance insertion lengths could facilitate safer fluoroscopy-free REBOA in austere, pre-hospital settings.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is an endovascular technique for temporary control of non-compressible truncal hemorrhage (NCTH) to prevent hemodynamic collapse and lethal exsanguination before definitive surgical therapy. The REBOA-concept is straightforward; the aorta is occluded by inflating a balloon at the tip of an intraluminal catheter proximally of the suspected bleeding site. It increases coronary and cerebral perfusion pressures proximally and limits blood flow distally from the aortic occlusion balloon (AOB). REBOA can be performed with a ‘one-step-insertion’ method after obtaining common femoral artery (CFA) access and placement of an introducer sheath.
For the use of REBOA, the aorta is divided in three anatomical zones. Occlusion in zone I, from the left subclavian artery (LSA) to the celiac trunk (CT), is used for abdominal hemorrhage control or as pressure support in cardiopulmonary resuscitation for cardiac arrest of various etiology. Zone III, the infrarenal aorta, is targeted in case of pelvic or junctional inguinofemoral (groin) bleeding. Zone II comprises the visceral artery branches and is currently considered a no-go zone that should be actively avoided.
In general, catheter advancement and balloon positioning are guided by fluoroscopy to prevent the risk of balloon inflation in the aortic arch, zone II or the iliac arteries. Incorrect placement could lead to suboptimal bleeding control or cause iatrogenic cerebral, visceral or lower extremity ischemia. However, imaging is not always readily available at bed-side or in pre-hospital civilian and military combat settings. The dependence on radiographic imaging for safe balloon positioning limits the more widespread use of REBOA in these austere situations where it could eminently serve as a life-saving bridge to definitive hemorrhage control.
Different alternatives for balloon navigation have been investigated. These include substitute imaging techniques as portable ultrasonography [1,2,3,4,5] and alternative modalities as radiofrequency and magnetic tracking methods [6, 7]. Besides reports about successful ‘blind’ insertion [8,9,10,11], multiple methods have been proposed to enable imaging- and tracking-free REBOA. These include the use of external anatomical landmarks [12,13,14,15,16,17], linear prediction models based on torso length (TL) [18, 19], standardized fixed-distance catheter lengths based on large sample means [17, 20, 21] and mathematical multivariable prediction formulas [22, 23]. The mid-sternum landmark is a dependable bony reference point for zone I placement with 100% correlation rate and acceptable safety-margins [12, 13, 17]. In contrast, using the umbilicus for zone III would cause erroneous (partial) iliac artery balloon placement in 67–98% [14, 17, 18].
The use of an external landmark or fixed-distance insertion length seem useful for zone I considering its long length, but not suitable for zone III. No optimal zone III introduction depths have been determined yet. The available studies are based on different populations and propose inconclusive, divergent insertion lengths. Therefore, the need for a simple, fast and reliable insertion method to liberate REBOA from radiographic imaging remains.
The primary aim was to determine standardized variable-distance catheter insertion lengths based on the combination of sex and age. These variables are easy to determine and estimate on-scene. The secondary aim was to evaluate sex and age-related differences in aorto-iliofemoral morphology in a representative sample of the civilian population. Establishing broadly applicable variable-distance insertion lengths could contribute to safe REBOA use in austere settings.
Method
Study population
To obtain a representative convenience sample of the general civilian population, all non-trauma patients receiving a contrast-enhanced computed tomography scan of the abdomen, pelvic region and groins at the emergency department of a peripheral teaching hospital between Augustus 2019 and December 2022 were eligible for inclusion. For definitive in- or exclusion, all scans were assessed on contrast-enhancement quality and presence of image slices of the abdominal aorta from above the celiac trunk towards both femoral bifurcations. Patients with a history of (F)EVAR or prosthetic aortic graft were excluded.
Central luminal line measurement method
The software program 3Mensio Vascular™ (Pie Medical Imaging BV, Maastricht, The Netherlands) was used to create a 3D-reconstruction of the aorta and iliofemoral trajectories and construct a central luminal line (CLL) within this vasculature (Fig. 1). By measuring along the central axis of the aorto-iliofemoral lumen, zone lengths and intravascular distances from the femoral arterial access points (FAAP) to the zone boundaries could be determined. The right and left CFA at the mid-femoral head level were chosen as the FAAP and starting points for the distance measurements [17,18,19, 23]. The REBOA-zones were defined by the major aortic branches which represent the zone boundaries. Zone III length was the distance between the aortic bifurcation (AB, inferior boundary of zone III) and the distal origin of the lowest main renal artery (RA, superior boundary of zone III). Zone II extended from the lower RA to the CT. Zone I ranged from the proximal origin of the CT (inferior boundary of zone I) to the distal origin of the LSA (superior boundary of zone I). Aortic diameters and the depth of the left CFA, defined as the shortest distance from the skin, were also measured. Two authors (JvdV and BV) performed the measurements.

Representative images of the intravascular distances measurement method with a 3D-reconstruction of the aorta and iliofemoral trajectory (a), construction of a central luminal line (b & c) and the stretched vessel configuration in coronal (d) and sagittal (e) anatomical plane with zone III (blue shaded region) and II (orange shaded region). The dotted lines represent the mid-femoral head (red), aortic bifurcation (green), distal origin of lowest renal artery (blue) and proximal origin of celiac trunk (orange) levels
Calculating fixed-distance catheter insertion lengths
For all subgroups, mean CLL-distances from the bilateral FAAP to all zone boundaries and mid-zone III with accompanying 95% (2 SD) confidence interval limits were calculated. Hereby the optimal mean catheter insertion lengths for zone III balloon positioning and potentially safe regions could be determined for all subgroups. Our analyzed scans did not include the thoracic aorta. To calculate the optimal zone I insertion length for our sample, the shortest absolute zone I length from all previously published studies was used to minimize the risk of LSA occlusion.
Subsequently, we simulated the introduction of the 40-mm long ER-REBOA™ (PryTime Medical™ Devices, Inc., Boerne, Texas) to determine malposition percentages. The calculated catheter insertion lengths corresponded with the middle of the balloon with 20-mm balloon extension in both cranial and caudal direction. Previously proposed insertion lengths were applied to our sample to compare out-of-zone placement rates [17, 20, 21, 23, 24].
Statistical analysis
Deidentified patient characteristics, total body height and -weight and distance measurements were registered in a Microsoft Excel® spreadsheet, version 16.66.1 (Microsoft, Redmond, Washington, USA). (Combined) sex-and age-based subgroups were created. Four age-groups were arbitrarily chosen; 18–30, 30–50, 50–70 and 70–90 years. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS®), version 29 (IBM corporation, Armonk, New York, USA) and GraphPad Prism®, version 9.5.0 (GraphPad Software Inc., San Diego, California, USA). Inter- and intra-observer reliability and consistency testing was performed at the start and end of the data collection for 30 patients each time using the intraclass correlation efficient and Cronbach’s alpha. Missing data were computed based on available age, body height and -weight data of other patients.
Data normality testing was done with histograms and Shapiro–Wilk tests. Continuous (quantitative) data were presented using mean ± standard deviation (SD) or median with interquartile range (IQR). Differences in measured distances between the two sexes regardless of age were compared with an unpaired Student’s t-test or Mann-Whitney U test. Comparison between (combined sex and) age-based subgroups was done with the one-way ANOVA with Bonferroni correction for multiple testing or the Kruskall-Wallis test. For each subgroup, bootstrap analysis with 10,000 sample simulations was performed to determine the proportion of patients for whom balloon placement at the calculated mean insertion length would have resulted in a ‘too high’ or ‘too low’ out-of-zone placement [25, 26]. For analyses, a p value < 0.05 was considered significant.
Results
Population demographics
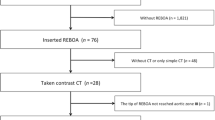
In total, 1354 non-trauma patients (694 females) were included after excluding 64 individuals because of various reasons (Table 1 & supplemental Fig. 1). Missing body height and weight data were computed for 264 patients (19.5%). Inter-observer reliability testing asserted there was no significant difference between the two measurers.
General sex- and age-based length variability
Up to the diaphragm, sex and age-based length variability and aortic elongation mainly occurs in zone II and the iliofemoral trajectory. Regardless of sex or insertion side, comparing the youngest with the oldest age group, the age-related mean distance increase from the FAAPs to the aortic bifurcation was 12 mm (male 15, female 9), to the lowest RA 13 mm (male 18, female 9) and to the CT 21 mm (male 26, female 18). Zone III showed a consistent length of ± 89 mm (male 91, female 87) regardless of age. Zone II, with a length of 37–49 mm, showed an age-related increase of 8 mm in both sexes, which translates to a 20–25% increase over the years (Tables 2 and 3 & supplemental Table 1). On average, the right iliofemoral vasculature was 7 mm longer compared with the left side regardless of sex or age.
Sex-based insertion lengths for zone III
After correction for multiple testing, all measured distances within the specific age-groups differed significantly between the sexes. For males, regardless of age, the optimal zone III catheter insertion length as calculated from the right and left CFA was 259 mm (95% CI 257.3-260.8) and 252 mm (95% CI 250.1-253.5), respectively. For females, regardless of age, the optimal insertion length from the right CFA was 247 mm (95% CI 245.0-247.9) and 240 mm (95% CI 238.2-240.9) from the left CFA (Table 1).
Age-based insertion lengths for zone III
Mean mid-zone III distances from the bilateral FAAPs showed significant differences between the four arbitrarily chosen age groups regardless of sex, except between the 30-50- and 50-70-years age groups. As measured from the right side, the optimal catheter insertion length for the age group of 18–30 years was 244 mm, for 30–70 years 252 mm and for 70–90 years 257 mm. From the left side, the optimal catheter insertion lengths were 237, 243–246 and 249 mm, respectively (supplemental Table 1).
Combined sex- and age-based insertion lengths for zone III
Significant differences were observed when comparing between sexes, age groups and insertion sides. Longer distances were consistently observed in males, elderly and on the right side (Tables 2, 3 and 4). For males, a 17 mm age-related increase of mean mid-zone III distance was observed between the youngest and oldest age group from both insertion sides. On the right side, optimal insertion lengths were 247, 255, 260 and 264 mm, respectively. On the left side these were 239, 243, 253 and 256 mm, respectively.
For females, a bilateral 9 mm increase of mean mid-zone III distance was observed over time. On the right side the distances were 242, 246, 244 and 251 mm while on the left side 234, 239, 238 and 243 mm, respectively. Sex-based elongation differences became larger with increased age. A maximum of 30 mm difference in mean zone III distance exists between the subgroups (Table 4; Fig. 2). For both sexes, not all age-based insertion lengths differed significantly from each other (supplemental Table 2).

Simulation of a 4-cm long balloon placement with 20 mm extension in cranial and caudal direction (transparent grey region) based on combined sex- and age-based variable-distance catheter insertion lengths (black line) for insertion from the right (a & c) and left (b & d) FAAPs. Individual superior (blue & yellow symbols) and inferior (green & orange symbols) zone III boundaries for females (a & b) and males (c & d) are plotted
Standardized fixed-distance insertion length for zone I
The minimum and maximum distance from the FAAPs to the inferior boundary of zone I were 280 and 460 mm, respectively. The shortest measured zone I length from all previously published studies was 190 mm. Hypothetically, the minimal absolute distance from the FAAPs to the LSA would therefore be 470 mm. For our sample, the optimal catheter insertion length would be 430 mm (20 mm cranial and caudal extension). This would cause a ‘too low’ error with partial zone II occlusion in maximal 1.8% of patients with at least a 2 cm proximal error margin to the LSA and 0% LSA occlusion.
Depth of common femoral artery
The mean distance from skin to the left CFA was 34.7 (SD 17.1) mm. In all age-groups, higher values were observed in females. Depth of the femoral artery was directly proportional to BMI (r = 0.654, R2 = 0.428, p < 0.001). 591 patients (43.6%) were in the overweight range (BMI 25–30) and 294 patients (21.7%) had obesity (BMI > 30).
Comparison with previous studies
High out-of-zone error-rates up to 89% were observed when applying previously proposed fixed-distance zone III catheter insertion lengths to our different subgroups. Our variable-distance insertion lengths would lead to combined out-of-zone error-rates between 13 and 33%. Sub analysis showed that sex- or age-based only lengths caused higher error-rates in the youngest age-groups, but similar malposition rates in older age-groups compared with combined sex- and age-based lengths (supplemental file).
Discussion
The optimal zone I catheter insertion length would be 430 mm. Optimal zone III insertion lengths showed up to 30 mm difference, ranging between 234 and 264 mm. Currently, the JTSCPG recommends introduction depths from the CFA of 460 mm for zone I and 280 mm for zone III, regardless of insertion side or patient characteristics as age, sex and TL. Although a one-size-fits-all strategy may be the most practical, a high percentage of patients would receive incorrect balloon positioning when using a solitary fixed-distance insertion length for zone III. This could result in inadequate hemorrhage control or iatrogenic limb and organ ischemia.
For those at risk of hemodynamic collapse, immediate action is required to achieve blood pressure stabilization and prevent exsanguination. In austere settings, REBOA could be the only viable option to maintain sufficient cardiac and cerebral perfusion. Bringing REBOA closer to the point-of-injury could prove lifesaving as endovascular alternative to external aortic clamping through thoracotomy [27]. In our recently published Delphi study, the panel recommended the initiation of a randomized clinical trial investigating REBOA use in civilian pre-hospital settings [28]. To robustly implement REBOA in (remote) pre-hospital trauma care, abolishing the need for additional imaging equipment and requiring minimal patient information is necessary.
Previously proposed standardized lengths
Fixed-distance catheter insertion lengths seem usable for zone I, but nor for zone III balloon positioning. Through analysis of 280 CT-scans of an equally mixed-sex civilian cohort (mean age 39 years), Pezy et al. defined a common segment in zone III between 236 and 256 mm as measured from the upper border of the pubic symphysis with a general predicted prevalence of 95% [20]. In 59 REBOA-patients Meyer et al. observed a median zone III insertion length of 29 (range 21–36) cm. Pezy’s predicted safe regions would have been located at least partially out of their measured zone boundaries in 50%.
Borger et al. included 250 patients (151 males, mean age 69 years) to compare age- and sex-based differences in central vasculature [17]. Measuring from the mid-section of the right CFA, they found mean mid-zone III distances of 274 (SD 28.0) mm for males and 251 (SD 23.3) mm for females. Divided in age-groups, mean mid-zone III distances were 251 (20–50 years), 263 (51–70 years) and 264 (71–94 years) mm regardless of sex. Applying the JTSCPG zone III introduction depth, accurate positioning occurred in only 38.0% with mainly ‘too low’ errors. Olsen et al. found similar lengths in a study with 100 patients (62 males, mean age 78 years). Distance from the left CFA (3 cm below mid-inguinal point) to mid-zone III was 27 (SD 2.0) cm for males and 25 (SD 1.8) cm for females [21]. An optimal 95% safe region would be located between 26 and 27 cm, but would still have led to six out-of-zone placements. In 177 males (median age 23 years, Afghan nationals and deployed US military personnel) Morrison et al. measured median mid-zone III distances from the right and left CFA at the mid-femoral head level of 232 (IQR 21) and 228 (IQR 22) mm, respectively [19]. Ethnicity had no effect on prediction accuracy.
Eliason et al. evaluated 1525 CT-scans of male and female trauma patients (1114 males, median age 31 years) [23]. The proposed fixed-distance insertion length for zone III was 28 cm when inserted from both FAAPs at the mid-femoral head level. Despite using a relatively simple equation to adjust for individual TL, the 33.3% out-of-zone placement rate could only be reduced to 26.3%. For zone III, variable-distance insertion lengths ranged from 22.5 cm to 32.5 cm, increasing 0.5 cm for 1 cm increase in TL. A 35% out-of-zone error-rate for zone III positioning was seen when simulating the then applicable JTSCPG depth of 27 cm.
These studies did not evaluate nor compare combined sex and age-based subgroups, propose divergent lengths and show accuracy discrepancies. Applying the generally longer introduction depths than those found in the current study would lead to high out-of-zone error-rates with extraordinary outliers for certain subgroups in our sample. Although not all of our subgroup mid-zone III lengths differed significantly, sex- or age-based only introduction depths would lead to higher erroneous zone II error-rates with possible RA or CT occlusion in younger patients. A more patient-tailored introduction method facilitates improved REBOA placement accuracy.
Zone III length, CFA depth & iliofemoral length variability
We found a rather consistent mean zone III length of approximately 89 mm. Previously reported lengths were between 83 and 104 mm with no mentioned significant sex differences. Only Borger et al. previously differentiated between age-groups and reported a significant difference between the two youngest and the oldest age-groups; 88, 96 and 104 mm, respectively. We observed a mean CFA depth of 34.7 mm, although with high individual variability. Similarly, Stannard and Eliason et al. observed median depths of 35 (29–41) mm and 37 (27–43) mm, while Pezy et al. reported a mean depth of 24 (10) mm. In accordance with previous studies, reporting differences between 4 and 9 mm, we found a significantly longer iliofemoral trajectory on the right side with an overall length difference of 7 mm regardless of sex or age.
Practical usability & feasibility
When possible, correct balloon position should always be confirmed. However, it has not been clarified yet whether (partial) zone II occlusion causes significant long-term detrimental side-effects compared to zone I or even zone III occlusion as is commonly believed [29, 30]. Since erroneous zone II occlusion would provide better bleeding-control than iliac artery occlusion, ‘too low’ errors should at least be avoided to prevent suboptimal bleeding-control combined with the needless risk of iatrogenic limb ischemia or possible dissection due to overinflation. Partial occlusion, either by partial and intermittent inflation or using innovative balloons, could potentially mitigate ischemia-related complications [31,32,33,34,35,36]. Partial zone II occlusion, most frequently limited to RA occlusion, seems practically unavoidable for a small percentage of the population, even when using variable zone III insertion lengths. Future studies should evaluate if and how erroneous zone II positioning is tolerated by investigating the possible local and systemic adverse effects of CT, superior mesenteric artery and RA occlusion.
In contrast to most studies, we took the balloon length in consideration for calculation and comparison of out-of-zone error-rates. These rates were much higher when including the balloon length. Extraordinarily high error-rates were seen when mutually comparing and applying the previously proposed insertion lengths and landing zones that do not take into account the age and sex-based variability. We observed up to almost a balloon length difference in mean mid-zone III distances between our subgroups. Therefore, we advocate that introduction depths should indeed be adjusted for sex and age as firstly proposed by Borger et al. to ensure more precise positioning in the youngest patients [17]. By applying different colored segments on conventional ABO-catheters, corresponding with specific subgroups, our variable-distance catheter insertion model could be simply implemented in daily practice.
Limitations
There are limitations to this study. Firstly, we aimed to prevent selection bias by including all patients receiving a CT-scan within a pre-determined time period regardless of age, sex and scan-indication. However, due to the location of the hospital in a semi-rural area we have not been able to include a wide variety of race or ethnicity. Secondly, the accuracy of determining the FAAP precisely at the mid-femoral head level cannot be matched in real-life. While we anticipate that this will not cause problems for zone I considering its long length, it could cause extra out-of-zone errors when targeting zone III. Thirdly, a stretched-vessel-configuration does not fully reflect the catheter pathway in tortuous vasculature. Lastly, the depth of the CFA varied greatly within the sample. In daily practice this will also be affected by the needle insertion angle and puncture site location. To achieve accurate balloon positioning, this depth must be taken into consideration and added to the insertion length. Ultrasonography could be used for both tissue thickness determination as well as FAAP localization.
By investigating a large, heterogenous group, we have gained better understanding of aorto-iliofemoral morphology. A more patient-tailored insertion-method seems feasible, but could also lead to a more complex model. A balance must be found between the number of subgroups and acceptable error-rates. Insertion models irrespective of body height or torso length are more straightforward. Our reproducible strategy only requires on-scene sex-determination and age-estimation without the need for time-consuming measurements or arduous calculations. Future studies are required to validate the proposed catheter insertion lengths and determine the degree of possible partial zone II occlusion.
Conclusion
We characterized the morphology of the abdominal aorta and identified optimal REBOA catheter insertion lengths for zone I and III balloon occlusion in a sample of the general civilian population. This is the first combined sex and age-based comparison of aortic intravascular distances. Significantly longer distances were seen in males, elderly and on the right side. Optimal zone III insertion lengths ranged between 234 and 264 mm. As the length of zone III is very consistent, length variability and elongation below the diaphragm seems to originate in the iliofemoral trajectory and zone II. The universal zone I insertion length is 430 mm. Standardized variable-distance catheter insertion lengths based on sex and age could facilitate safer fluoroscopy-free REBOA in pre-hospital and resource limited settings.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- REBOA:
-
Resuscitative endovascular balloon occlusion of the aorta
- NCTH:
-
Non-compressible truncal hemorrhage
- AOB:
-
Aortic occlusion balloon
- CFA:
-
Common femoral artery
- LSA:
-
Left subclavian artery
- CT:
-
Celiac trunk
- TL:
-
Torso length
- (F)EVAR:
-
(Fenestrated) endovascular aneurysm repair
- CLL:
-
Central luminal line
- FAAP:
-
Femoral arterial access point
- AB:
-
Aortic bifurcation
- RA:
-
Renal artery
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- BMI:
-
Body mass index
- JTSCPG:
-
Joint Trauma System Clinical Practice Guideline
- ABO:
-
Aortic balloon occlusion
References
Brede JR, Lafrenz T, Klepstad P, et al. Feasibility of Pre-hospital resuscitative endovascular balloon occlusion of the Aorta in Non-traumatic out-of-hospital cardiac arrest. J Am Heart Assoc. 2019;8(22). https://doi.org/10.1161/JAHA.119.014394.
Chaudery M, Clark J, Morrison JJ, Wilson MH, Bew D, Darzi A. Can contrast-enhanced ultrasonography improve Zone III REBOA placement for prehospital care? J Trauma Acute Care Surg. 2016;80(1):89–94. https://doi.org/10.1097/TA.0000000000000863.
Chen K, Zhang G, Li F, et al. Application of ultrasound-guided balloon occlusion in cesarean section in 130 cases of sinister placenta previa. J Interv Med. 2020;3(1):41–4. https://doi.org/10.1016/j.jimed.2020.01.006.
Ogura T, Lefor AK, Nakamura M, Fujizuka K, Shiroto K, Nakano M. Ultrasound-guided resuscitative endovascular balloon occlusion of the Aorta in the Resuscitation Area. J Emerg Med. 2017;52(5):715–22. https://doi.org/10.1016/j.jemermed.2017.01.014.
Riazanova OV, Reva VA, Fox KA, et al. Open versus endovascular REBOA control of blood loss during cesarean delivery in the placenta accreta spectrum: a single-center retrospective case control study. Eur J Obstet Gynecol Reprod Biol. 2021;258:23–8. https://doi.org/10.1016/j.ejogrb.2020.12.022.
Rezende-Neto JB, Ravi A, Semple M. Magnetically trackable resuscitative endovascular balloon occlusion of the aorta: a new non-image-guided technique for resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2020;88(2):e87–91. https://doi.org/10.1097/ta.0000000000002437.
Wessels LE, Wallace JD, Bowie J, Butler WJ, Spalding C, Krzyzaniak M. Radiofrequency Identification of the ER-REBOA: confirmation of Placement without Fluoroscopy. Mil Med. 2019;184(3–4):E285–9. https://doi.org/10.1093/milmed/usy187.
Lendrum R, Perkins Z, Chana M, et al. Pre-hospital resuscitative endovascular balloon occlusion of the aorta (REBOA) for exsanguinating pelvic haemorrhage. Resuscitation. 2019;135:6–13. https://doi.org/10.1016/j.resuscitation.2018.12.018.
Stensaeth KH, Sovik E, Haig IN, Skomedal E, Jorgensen A. Fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta (REBOA) for controlling life threatening postpartum hemorrhage. PLoS ONE. 2017;12(3):e0174520. https://doi.org/10.1371/journal.pone.0174520.
Manning JE. Feasibility of blind aortic catheter placement in the prehospital environment to guide resuscitation in cardiac arrest. J Trauma Acute Care Surg. 2013;75(2 Suppl 2):S173–7. https://doi.org/10.1097/TA.0b013e318299d9ee.
De Schoutheete JC, Fourneau I, Waroquier F, et al. Three cases of resuscitative endovascular balloon occlusion of the aorta (REBOA) in austere pre-hospital environment: technical and methodological aspects. World J Emerg Surg. 2018;13:1–11.
Linnebur M, Inaba K, Haltmeier T, et al. Emergent non-image-guided resuscitative endovascular balloon occlusion of the aorta (REBOA) catheter placement: a cadaver-based study. J Trauma Acute Care Surg. 2016;81(3):453–7. https://doi.org/10.1097/TA.0000000000001106.
Okada Y, Narumiya H, Ishi W, Iiduka R. Anatomical landmarks for safely implementing resuscitative balloon occlusion of the aorta (REBOA) in zone 1 without fluoroscopy. Scand J Trauma Resusc Emerg Med. 2017;25(1). https://doi.org/10.1186/s13049-017-0411-z.
Matsumoto S, Funabiki T, Kazamaki T, et al. Placement accuracy of resuscitative endovascular occlusion balloon into the target zone with external measurement. Trauma Surg Acute Care Open. 2020;5(1). https://doi.org/10.1136/tsaco-2020-000443.
Sato R, Kuriyama A, Takaesu R, et al. Resuscitative endovascular balloon occlusion of the aorta performed by emergency physicians for traumatic hemorrhagic shock: a case series from Japanese emergency rooms. Crit Care. 2018;22(1):103. https://doi.org/10.1186/s13054-018-2032-y.
Weng D, Qian A, Zhou Q, Xu J, Xu S, Zhang M. A new method using surface landmarks to locate resuscitative endovascular balloon occlusion of the aorta based on a retrospective CTA study. Eur J Trauma Emerg Surg. 2022;48(3):1945–53. https://doi.org/10.1007/s00068-021-01686-0.
van der Borger B, Vrancken S, van Dongen T, Wamsteker T, Rasmussen T, Hoencamp R. Comparison of aortic zones for endovascular bleeding control: age and sex differences. Eur J Trauma Emerg Surg. 2022;48(6):4963–9. https://doi.org/10.1007/s00068-022-02033-7.
Stannard A, Morrison JJ, Sharon DJ, Eliason JL, Rasmussen TE. Morphometric analysis of torso arterial anatomy with implications for resuscitative aortic occlusion. J Trauma Acute Care Surg. 2013;75(2 Suppl 2):S169–72. https://doi.org/10.1097/TA.0b013e31829a098d.
Morrison JJ, Stannard A, Midwinter MJ, Sharon DJ, Eliason JL, Rasmussen TE. Prospective evaluation of the correlation between torso height and aortic anatomy in respect of a fluoroscopy free aortic balloon occlusion system. Surgery. 2014;155(6):1044–51. https://doi.org/10.1016/j.surg.2013.12.036.
Pezy P, Flaris AN, Prat NJ, et al. Fixed-Distance Model for Balloon Placement during Fluoroscopy-Free resuscitative endovascular balloon occlusion of the Aorta in a Civilian Population. JAMA Surg. 2017;152(4):351–8. https://doi.org/10.1001/jamasurg.2016.4757.
Olsen MH, Thonghong T, Søndergaard L, Møller K. Standardized distances for placement of REBOA in patients with aortic stenosis. Sci Rep. 2020;10(1). https://doi.org/10.1038/s41598-020-70364-9.
MacTaggart JN, Poulson WE, Akhter M, et al. Morphometric roadmaps to improve accurate device delivery for fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2016;80(6):941–6. https://doi.org/10.1097/TA.0000000000001043.
Eliason JL, Derstine BA, Horbal SR, et al. Computed tomography correlation of skeletal landmarks and vascular anatomy in civilian adult trauma patients: implications for resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2019;87(1S):S138–45. https://doi.org/10.1097/TA.0000000000002247.
Glaser J, Stigall K, Morrison J et al. The Joint Trauma System Clinical Practice Guideline (JTSCPG). Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) for Hemorrhagic Shock (CPG ID: 38). 2020. http://jts.amedd.army.mil/assets/docs/cpgs/JTS_Clinical_Practice_Guidelines_(CPGs)/REBOA_for_Hemorrhagic_Shock_06_Jul_2017_ID38.pdf
Efron B. Bootstrap methods: another look at the Jackknife. Ann Statist. 1992;7(1):1–26. https://doi.org/10.1007/978-1-4612-4380-9_41.
Haukoos JS, Lewis RJ. Advanced statistics:Bootstrapping confidence intervals for statistics with difficult distributions. Acad Emerg Med. 2005;12(4):360–5. https://doi.org/10.1197/j.aem.2004.11.018.
Cralley AL, Vigneshwar N, Moore EE, et al. Zone 1 endovascular balloon occlusion of the aorta vs resuscitative thoracotomy for patient resuscitation after severe hemorrhagic shock. JAMA Surg. 2023;158(2):140. https://doi.org/10.1001/jamasurg.2022.6393.
van de Voort JC, Kessel B, van der Borger BLS, DuBose JJ, Hörer TM, Hoencamp R. Consensus on resuscitative endovascular balloon occlusion of the aorta (REBOA) in civilian (pre-hospital) trauma care: a Delphi study. J Trauma Acute Care Surg Published Online January. 2024;26. https://doi.org/10.1097/TA.0000000000004238.
Dogan EM, Hörer TM, Edström M, et al. Resuscitative endovascular balloon occlusion of the aorta in zone I versus zone III in a porcine model of non-traumatic cardiac arrest and cardiopulmonary resuscitation: a randomized study. Resuscitation. 2020;151:150–6. https://doi.org/10.1016/j.resuscitation.2020.04.011.
Halvachizadeh S, Mica L, Kalbas Y, et al. Zone-dependent acute circulatory changes in abdominal organs and extremities after resuscitative balloon occlusion of the aorta (REBOA): an experimental model. Eur J Med Res. 2021;26(1). https://doi.org/10.1186/s40001-021-00485-y.
Russo RM, Neff LP, Lamb CM et al. Partial resuscitative endovascular balloon occlusion of the aorta in swine model of hemorrhagic shock. J Am Coll Surg. 2016;223:359–68. https://doi.org/10.1016/j.jamcollsurg.2016.04.037
Russo RM, White JM, Baer DG, Partial REBOA. A systematic review of the preclinical and clinical literature. J Surg Res. 2021;262:101–14. https://doi.org/10.1016/j.jss.2020.12.054.
Sadeghi M, Hörer TM, Forsman D, et al. Blood pressure targeting by partial REBOA is possible in severe hemorrhagic shock in pigs and produces less circulatory, metabolic and inflammatory sequelae than total REBOA. Injury. 2018;49(12):2132–41. https://doi.org/10.1016/j.injury.2018.09.052.
Sadeghi M, Hurtsén AS, Tegenfalk J, et al. End-tidal Carbon Dioxide as an Indicator of partial REBOA and distal organ metabolism in Normovolemia and hemorrhagic shock in anesthetized pigs. Shock. 2021;56(4):647–54. https://doi.org/10.1097/SHK.0000000000001807.
Polcz JE, Ronaldi AE, Madurska M, et al. Next-generation REBOA (resuscitative endovascular balloon occlusion of the aorta) device precisely achieves targeted Regional optimization in a Porcine Model of hemorrhagic shock. J Surg Res. 2022;280:1–9. https://doi.org/10.1016/j.jss.2022.06.007.
White JM, Ronaldi AE, Polcz JE, et al. A New Pressure-Regulated, partial REBOA device achieves targeted distal perfusion. J Surg Res. 2020;256:171–9. https://doi.org/10.1016/j.jss.2020.06.042.
Funding
This study was funded by the Dutch Army Health Insurance Foundation (Stichting Ziektekostenverzekering Krijgsmacht, SZVK) and the Dutch Ministry of Defense (project number 19–0068). No other support was provided.
Author information
Authors and Affiliations
Contributions
JvdV, BBvdB and RH conceptualized the study and wrote the study protocol. JvdV and BV performed the data extraction. JvdV and BV performed the statistical analysis. JvdV drafted the sections of the manuscript. All authors critically revised the draft manuscript and contributed to the subsequent revisions and the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
The study protocol was reviewed by the Alrijne Hospital Medical Ethical Committee and approved under number NWMO 22–32. The study protocol complied with the Declaration of Helsinki.
Consent
This retrospective, non-interventional study (protocol number NWMO 22–32) was approved by the Medical Ethical Committee of the Alrijne Hospital which ruled that this study was deemed exempt for ethical approval by/under Dutch law and that for the use of available scans and data no explicit approval or informed consent from patients was necessary. This study complies with the Declaration of Helsinki.
Disclaimer
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Dutch Ministry of Defense or any other agency of the Dutch government. Several authors are employees of the Dutch government.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van de Voort, J.C., Verbeek, B.B., van der Burg, B.L.B. et al. Exploring aortic morphology and determining variable-distance insertion lengths for fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta (REBOA). World J Emerg Surg 19, 29 (2024). https://doi.org/10.1186/s13017-024-00557-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13017-024-00557-4