
Abstract
Background
Surgical reconstruction of the posterior cruciate ligament (PCL) can be technically challenging given the proximity of the popliteal artery to the PCL tibial insertion. This "no-safe zone" makes some knee surgeons less confident and willing to perform this surgical procedure.
Surgical technique
We present a PCL tibial inlay reconstruction technique using a set of instruments involving three tools (a slot cut, a bone plug positioner, and an impactor).
Conclusion
This set of instruments allows a more reproducible posteromedial approach and to produce a PCL tibial slot in a posterior cruciate ligament inlay reconstruction with the patient supine in bicruciate ligament injury reconstruction.
Similar content being viewed by others



Introduction
Surgical reconstruction of the posterior cruciate ligament (PCL) can be technically challenging given the proximity of the popliteal artery to the PCL tibial insertion [1, 2]. This area, the “no-safe zone”, makes some knee surgeons less confident and willing to perform this surgical procedure [3,4,5]. Surgical reconstruction of the PCL can be performed using two main techniques: the tibial tunnel or the tibial inlay technique [6, 7]. The tibial tunnel technique approaches the PCL tibial insertion using a specific guide under arthroscopic control and, in some circumstances, fluoroscopic control. The PCL tibial inlay technique allows direct approach to the tibial insertion of the PCL [8,9,10]. Both methods seem to produce equivalent results [1, 2, 11]. Since 2002, we have used the PCL inlay open technique, positioning the patient prone to undertake a posteromedial expose the tibial insertion of the PCL (Fig. 1) [5, 13, 14].

Posteromedial approach with the patient prone: A the bone block of the bone-patellar tendon-bone graft (blue cyan arrow); B after fixation of the bone block at the insertion of the PCL on the tibia (white arrow)
We originally, used an open technique [5, 15, 16]. Since 2009, drilling of the PCL femoral tunnel has been performed arthroscopically, and the tibial insertion of the PCL has been approached in an open fashion with the patient supine [17, 18]. We developed a PCL tibial inlay system for a more reproducible posteromedial approach and bone plug positioning with the patient supine. This set of instruments involves three tools (a slot cut, a bone plug positioner, and an impactor) that allow to reproducibly produce a PCL tibial slot for bone plugs of placement of the PCL tendon-bone graft Fig. 2.

Lateral (A) and front (B) views of the Piedade tibial Inlay set of instruments: slot cut (osteotome), (2) positioner, and (3) impactor
Indication
Non-surgical management is normally indicated for grade I and II PCL injuries, but the surgery can be considered for grade II posterior instability. Surgery is considered mandatory for grade III (15-mm posterior knee displacement) PCL tears, and complex knee ligament injuries, including bicruciate injury, and PCL tears associated with peripheral components [6,7,8]. Obviously, decision-making should be based on thorough clinical assessment and stress radiographs (https://pubmed.ncbi.nlm.nih.gov/19464187/).
Surgical technique–no changing of patient decubitus
-
1.
With the patient supine and under spinal anaesthesia, the knee is kept at 90° flexion with a support on the lateral aspect of the proximal 1/3 of the thigh and another under the foot. After exsanguination, the tourniquet is inflated to 300 mmHg.
-
2.
A routine diagnostic arthroscopy of the knee is performed to confirm the diagnosis. If necessary, meniscal injuries are addressed.
-
3.
The PCL and anterior cruciate ligament (ACL) stumps are resected.
-
4.
The PCL and ACL femoral tunnels are drilled using an outside-in PCL guide positioned at the origin of the PCL and ACL in the femur, under arthroscopic control, respectively (Fig. 3A and B). Initially, the bone tunnel has a 6 mm diameter and will be adjusted later, according to the diameter of the harvested graft.
Fig. 3 
Femoral tunnel positioning of PCL (A) and (B) ACL (B) tunnels, and (C) ACL tibial tunnel under arthroscopic control
-
5.
Then, the central third of the quadriceps tendon with patella bone plug is harvested through a midline longitudinal 7-cm incision
-
6.
Through a 5-cm longitudinal incision on the pes anserinus, the gracilis and semitendinosus tendons are harvested with an open stripper, keeping them attached to their insertion on the tibia
-
7.
The diameter of the PCL and ACL femoral tunnels is adjusted after measuring the diameter of the final graft.
-
8.
Using the incision used to harvest the hamstring tendons, the ACL tibial tunnel is drilled at a 55° angle using a tibial guide under direct arthroscopic control (Fig. 3C)
-
9.
After all bone tunnels have been drilled, the length of ACL graft (double gracilis-semitendinosus tendon graft) is measured and the graft prepared using vicryl 2.0

Knee posteromedial approach with the patient supine
-
10.
The hip is kept in external rotation and the knee at 90 degrees of flexion (Fig. 4A and B)
Fig. 4 
Knee posteromedial approach: Lower limb positioning with external hip rotation, and the knee flexion (A) and intraoperative view of posteromedial approach of PCL tibial insertion in the right knee (B)
-
11.
An a L-inverted posteromedial incision curved incision is performed, with the horizontal branch of the L places in the knee flexion crease (Fig. 5A)
Fig. 5 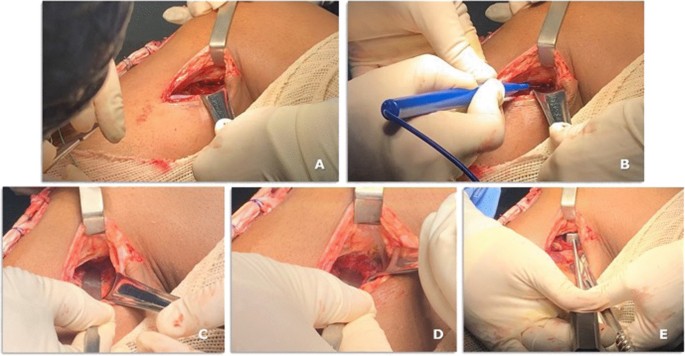
A case of bicruciate ligament reconstruction showing the posteromedial approach (A–D) and the Piedade PCL tibial INLAY bone slot cut is positioned on the PCL tibial insertion (E)
-
12.
The deep fascia is incised vertically (Fig. 5B)
-
13.
After blunt dissection between the medial border of the gastrocnemius muscle and semimembranosus tendon, the medial border of the gastrocnemius is retracted laterally and posteriorly to expose the posterior capsule (Fig. 5C–E).
-
14.
The capsule is opened using a medial vertical incision, and the PCL tibial insertion is visualized Fig. 5D
-
15.
Then, the Piedade PCL tibial inlay bone slot cut is positioned on the PCL tibial insertion, and a hammer is used to tap and produce a bone slot (10 mm long, 9 mm wide, and 10 mm deep) (Figs. 5E, 6A–C and, 7A).
-
16.
After removing the cortical bone of this slot (Fig. 6D), the Piedade PCL tibial inlay bone slot impactor is used to regularize the walls of the slot and its depth according to the dimensions of the harvested patella bone plug (Figs. 6E and 7B).
Fig. 6 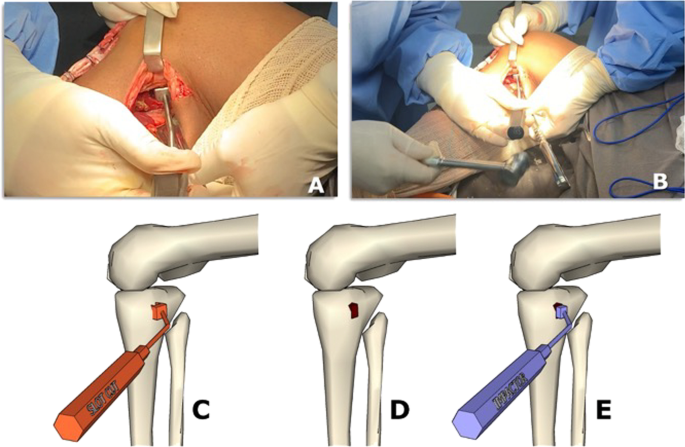
Producing the PCL tibial slot using the set of instruments: slot cut (A and B) and impactor (C and D) to control the depth of the slot according to the graft bone block. Note that the lower leg is externally rotated during this phase of the procedure
Fig. 7 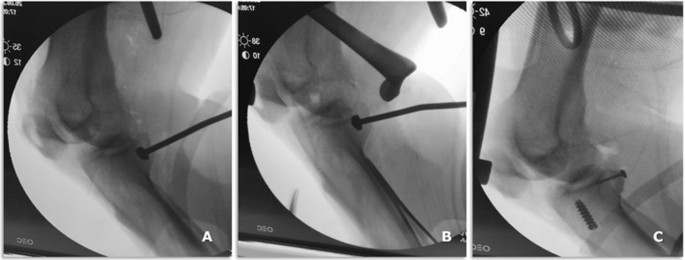
Intraoperative radiographic view of osteotome (A) and impactor (B) positioning on the PCL tibial bed and PCL and ACL graft fixation on the tibial side (C)
-
17.
Before passing the graft, a pull-out bone tunnel is added to the graft fixation by drilling a 2.5-mm tunnel just below the PCL bone slot from the posterior to the anterior aspect of the knee joint (Figs. 8A, 9)
Fig. 8 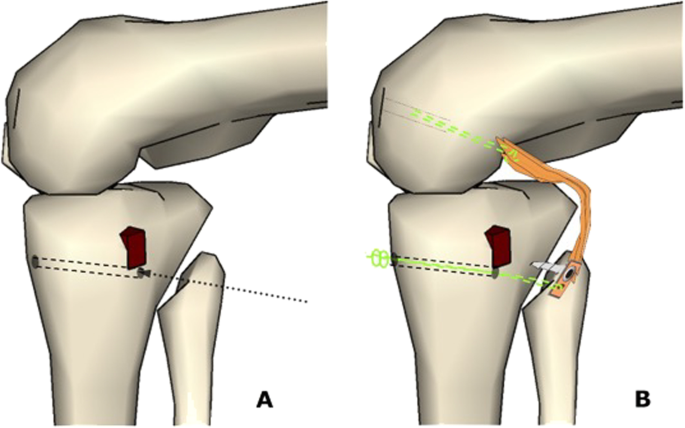
A Illustrates the 2.5 mm tunnel just below the PCL bone slot from the posterior to the anterior aspect of the knee joint, and B shows the passage of PCL graft controlled by Ethibond 5.0 thread in the transtibial and PCL femoral tunnels
Fig. 9 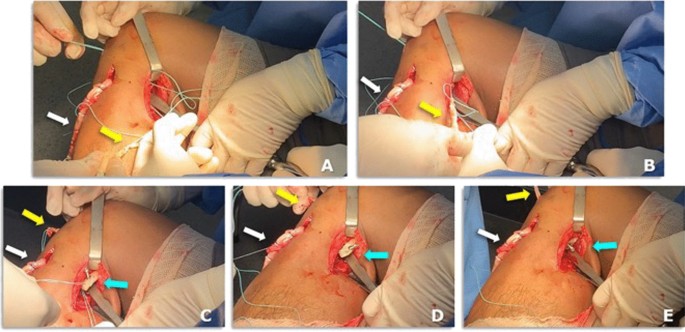
The PCL graft is shuttled into the knee joint through the tunnels using an Ethibond 5.0: A–E showing intraoperative views of the free end of PCL graft (yellow arrow), bone block with 3.5-mm cortical screw and washer of PCL graft (blue cyan arrow) and four stand of hamstring tendon of ACL graft (white arrow)
-
18.
Then, the free end of the quadriceps tendon bone graft is passed from the posterior aspect into the knee joint up to the femoral tunnel using Ethibond thread 5.0, while the patellar bone block is inserted in the tibial slot guided guide a Ethibond thread 5.0 that was passed from tunnel drilled from the posterior to the anterior aspect of the tibia to tension it (Fig. 8B).
-
19.
The patellar bone plug is positioned into the tibial slot using the PCL tibial inlay bone slot positioner, and further tension is applied using the Ethibond 5.0 suture to provide additional fixation (Fig. 8 B)
-
20.
Tibial fixation starts by bone plug impaction using the PCL tibial INLAY bone slot IMPACTOR; 3.5mm cortical screw and washer fixation (24 or 46 mm); capsule suturing and pull-out fixation are performed (Fig. 10A–C).
Fig. 10 
A PCL graft tensioning, impaction and fixation with a 3.5 mm cortical screw (24 or 26 mmm long) (B, C and D)
-
21.
The ACL graft is then shuttled into the knee joint through the tunnels using an Ethibond 5.0 suture, and the knee is flexed and extended 20 times to tension the graft.
-
22.
The ACL graft fixation starts on tibial side, using an interference screw 1 mm in diameter greater than the respective tunnel.
-
23.
With the knee positioned at 90 degrees of flexion, the PCL graft is fixed on the femoral tunnel femoral fixation of PCL graft using an interference screw 1 mm in diameter greater than the respective tunnel, making sure that the knee is kept in neutral rotation. A gentle anterior drawer manoeuvre is performed at this stage to keep the knee anteriorly displaced for PCL femoral tunnel fixation, making sure that the normal contralateral knee is used as reference.
-
24.
The ACL graft is fixed on the femoral side using an interference screw 1 mm in diameter greater than the respective tunnel (Fig. 11A and B)
Fig. 11 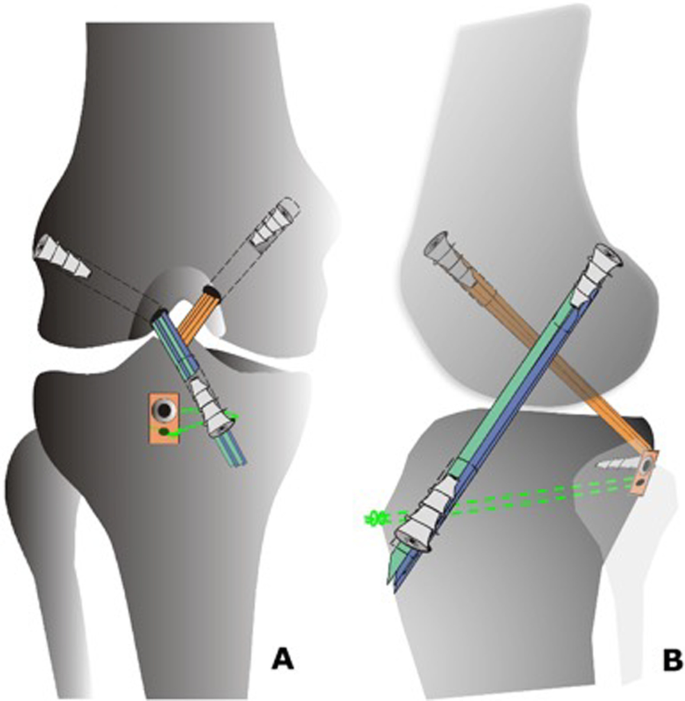
Drawing of bicruciate reconstruction after PCL and ACL fixation
-
25.
Clinical manoeuvres are performed to ensure that posterior and anterior knee stability have been restored and that a full range of motion of the knee is possible.
-
26.
The tourniquet is released, hemostasis is done, and the wound is sutured in a standard fashion
-
27.
The knee is bandaged in a routine fashion and immobilized in a full extension brace








Postoperative management
In the first two postoperative weeks, the knee is kept in full extension in a brace, and full weight-bearing is allowed keeping the knee immobilized in the brace. Using crutches is not mandatory, but patients feel more confident using them for the first 2 or 3 postoperative weeks. Cryotherapy and isometric exercises are introduced from the first postoperative day. The sutures are removed after two weeks. The brace is gradually unlocked after six weeks postoperatively, and motion is restricted to 45° in flexion until the six postoperative weeks.
After 12 weeks, the brace is completely removed, and rehabilitation focuses on progressively gaining full range of motion, which is expected to be achieved at around three months postoperatively.
Key points of this surgical technique
The knee posteromedial approach
-
Removing the lateral knee holder facilitates positioning of the leg, and allows access to the posterior aspect of the knee with the patient supine
-
The medial head of the gastrocnemius is retracted posteriorly and laterally so that the neurovascular structures were kept away from the surgical field
The Piedade PCL tibial inlay set of instruments
Allows to approach the PCL tibial insertion site to produce a suitable tibial slot, of depth adequate to the dimensions of the graft bone plug.
The central third of the quadriceps tendon graft should be
-
At least 13 cm long, including the patellar bone plug (2 cm long, 1 cm wide and 1 cm thick).
-
After harvesting the graft, two 2.5-mm drill holes are produced in the patella bone plug to be fixed by 3.5 mm cortical screw and washer on the PCL tibial bed.
PCL graft fixation on the tibial side
-
A 3.5-mm cortical screw is used in the proximal 2.5-mm tunnel in the patella bone plug, while in the distal 2.5-mm tunnel of in the patella bone plug a 5.0 Ethibond suture is used for pull-out fixation.
-
The patella bone plug will be fixed by bone impaction (1), 5.0 Ethibond pull-out (2), a 3.5-mm cortical screw, and capsular suturing.
Tunnel bone adjustment
-
We prefer starting with a 6-mm bone tunnel just after arthroscopic assessment of intra-articular injuries and adjust the tunnel diameter after preparing the graft.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available throughout the manuscript.
Abbreviations
- PCL:
-
Posterior cruciate ligament
- ACL:
-
Anterior cruciate ligament
References
Kew ME, Miller MD. Posterior cruciate ligament reconstruction in the multiple ligament injured knee. J Knee Surg. 2020;33(5):421–30.
Badet R, Demey G, Piedade SR. Reconstruction du ligament croise postérieur. In: Arthroscopie L, editor. Principes, objectifs et tunnelisation. 3rd ed. Paris: Elsevier; 2015. p. 1047–56.
Badet R, Verdonk P, Piedade SR. Technique in PCL reconstruction: mini posterior approach. In: Bonin M, Amendola A, Bellemans J, MacDonald S, Menetrey J, editors. The knee joint. Surgical: techniques and strategies. Paris: Springer; 2012. p. 411–5.
Martin RK, Melugin HP, Freychet B, Krych AJ, Stuart MJ, Levy BA. Posterior cruciate ligament all-inside reconstruction. Sports Med Arthrosc Rev. 2020;28(1):18–22.
Piedade SR, Mischan MM, Knee PCL. reconstruction: a tibial bed fixation (“inlay”) technique objective and subjective evaluation of a 30-cases series. Acta Ortop Bras. 2006;14(2):92–6.
Salim R, Nascimento FMD, Ferreira AM, Oliveira LFL, Fogagnolo F, Kfuri M. Tibial onlay posterior cruciate ligament reconstruction: surgical technique and results. J Knee Surg. 2018;31(3):284–90.
Therrien E, Pareek A, Song BM, Wilbur RR, Stuart MJ, Levy BA. All-inside PCL reconstruction. J Knee Surg. 2021;34(5):472–7.
Migliorini F, Pintore A, Vecchio G, Oliva F, Hildebrand F, Maffulli N. Hamstring, bone-patellar tendon-bone, quadriceps and peroneus longus tendon autografts for primary isolated posterior cruciate ligament reconstruction: a systematic review. Br Med Bull. 2022;142(1):23–33.
Migliorini F, Pintore A, Vecchio G, Oliva F, Hildebrand F, Maffulli N. Ligament advanced reinforcement system (LARS) synthetic graft for PCL reconstruction: systematic review and meta-analysis. Br Med Bull. 2022;143(1):57–68.
Lee DY, Kim DH, Kim HJ, Ahn HS, Lee TH, Hwang SC. Posterior cruciate ligament reconstruction with transtibial or tibial inlay techniques: a meta-analysis of biomechanical and clinical outcomes. Am J Sports Med. 2018;46(11):2789–97.
Zhang J, Zhang H, Zhang Z, Zheng T, Li Y. No difference in subjective and objective clinical outcomes between arthroscopic transtibial and open inlay posterior cruciate ligament reconstruction techniques in the treatment of multi-ligamentous knee injuries. Knee. 2021;30:18–25.
Bergfeld JA, Graham SM, Parker RD, Valdevit ADC, Kambic HE. A biomechanical comparison of posterior cruciate ligament reconstructions using single- and double bundle tibial inlay techniques. Am J Sports Med. 2005;33(7):976–81.
Badet R, Verdonk P, Piedade SR. Technique in PCL reconstruction: mini posterior approach. In: Bonin M, Amendola A, Bellemans J, MacDonald S, Menetrey J, editors. The knee. Joint surgical: techniques and strategies. Paris: Springer; 2012. p. 411–5.
Burks RT, Schaffer JJ. A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop Relat Res. 1990;254:216–9.
Inada MM, Piedade SR. Clinical outcomes after two-stage bicruciate knee ligament reconstruction. Acta Ortop Bras. 2021;29(1):7–11.
Gigliotakaes I, Inada MM, de Miranda JB, Cunha SA, Piedade SR. Isokinetic evaluation after two-stage bicruciate reconstruction. Acta Ortop Bras. 2014;22(1):21–4.
Stannard JP, McKean RM. Anatomic PCL reconstruction: the double bundle Inlay technique. Oper Tech Sports Med. 2009;17(3):148–55.
Richter D, Wascher DC, Schenck RC. A novel posteromedial approach for tibial Inlay PCL reconstruction in KDIIIM injuries. Avoiding prone patient positioning. Clin Orthop Relat Res. 2014;472:2680–26902009.
Acknowledgements
We thank Architect Ana Karina Piedade for developing the prototypes and the final version of the Piedade PCL tibial inlay set of instruments and INNOMED, Inc., for manufacturing these surgical instruments.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
SRP: conceptualization, supervision, revision; GML: writing; NM: writing; FM: writing. All authors have agreed to the final version to be published and agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
The present study was conducted in accordance with principles expressed in the Declaration of Helsinki. Signed informed consent for the intraoperative photos was obtained from the patient.
Consent for publication
All patients signed the consent to publish their data.
Competing interests
Prof. Nicola Maffulli is Editor in Chief of the Journal of Orthopaedic Surgery and Research.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Piedade, S.R., Laurito, G.M., Migliorini, F. et al. Posterior cruciate ligament reconstruction using PCL inlay technique with the patient supine in bicruciate ligament injury reconstruction. J Orthop Surg Res 18, 16 (2023). https://doi.org/10.1186/s13018-022-03495-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-022-03495-6