
Abstract
Objective
This study analyzes the safety and efficacy of percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) treatments for Stage III Kummell’s disease without neurological symptoms, comparing the advantages and disadvantages of these two minimally invasive surgical methods.
Methods
A retrospective analysis was conducted on 53 patients with non-neurological Stage III Kummell’s disease treated with PVP and PKP at our hospital from December 2018 to January 2023. Patients were divided into PVP (25 cases) and PKP (28 cases) groups based on the surgical method. There were no significant differences in general preoperative data between the two groups (all p > 0.05), ensuring comparability. The study compared surgical duration, volume of bone cement injected, distribution pattern of bone cement, rate of bone cement leakage, and preoperative, postoperative, and final follow-up scores of Visual analogue scale(VAS) and Oswestry disability index(ODI). Additionally, relative anterior height of the injured vertebrae, and Cobb angle of deformity, along with their changes at preoperative, postoperative, and final follow-up stages were calculated and analyzed.
Results
No significant preoperative differences were observed between the groups (p > 0.05). The PKP group had longer surgeries, higher cement volumes (p < 0.001), and lower leakage rates (p < 0.05), with primarily chunky cement distributions versus mixed distributions in the PVP group. No complications other than cement leakage occurred. VAS and ODI scores showed no significant changes at various time points (p > 0.05) but improved significantly from preoperative (p < 0.001). Both groups saw improved vertebral heights and Cobb angles post-surgery (p < 0.05), with more significant improvements in the PKP group (p < 0.05). Over time, both groups experienced gradual vertebral height loss and increased Cobb angles, more pronounced in the PKP group (p < 0.05). At the final follow-up, there were no statistical differences in vertebral height and Cobb angle between the two groups (p > 0.05).
Conclusion
The study evaluates the safety and efficacy of PVP and PKP for Stage III Kummell’s disease without neurological symptoms, comparing the merits of both minimally invasive techniques.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
With the continuous advancements in modern medicine, clinicians’ understanding of Kummell’s disease(KD) has significantly deepened. In the context of an aging population, both the diagnosis and incidence rates of KD are progressively increasing. KD is characterized by delayed vertebral collapse and progressive kyphosis following minor trauma [1], typically a sequel to osteoporotic vertebral compression fractures (OVCF) in the elderly, predominantly affecting the high-stress thoracolumbar region, usually involving a single vertebral segment [2, 3]. According to Li et al., KD is classified into three stages based on imaging and symptoms: Stage I involves less than 20% vertebral height loss with back pain but no neurological symptoms; Stage II exceeds 20% loss, primarily presenting with back pain; Stage III includes posterior vertebral cortex rupture, possibly with or without spinal compression, manifesting as back pain or neurological damage [4].
Regarding the treatment of KD, most scholars advise against conservative methods, favoring surgical interventions instead [5, 6]. KD patients are predominantly elderly, and minimally invasive surgeries that minimize trauma and expedite recovery are deemed ideal. Previous studies have shown that PVP and PKP achieve favorable clinical outcomes for Stage I and II KD patients [6]. However, for Stage III Kummell’s disease without neurological deficits, there is significant controversy regarding whether PVP and PKP surgeries can restore vertebral stability, the safety of these procedures given posterior vertebral rupture, and which surgical approach is more suitable for patients with Stage III KD without neurological impairment. To address this, we conducted a retrospective analysis of the safety and efficacy of PVP and PKP in treating Stage III KD without neurological symptoms, comparing the advantages and disadvantages of these minimally invasive techniques to inform clinical practice.
Methods
Patient selection
Patients treated with PKP or PVP surgery for Stage III KD without neurological impairment from December 2018 to January 2023 at the First Clinical Medical College of Three Gorges University were selected as subjects for this study. This study was approved by the hospital’s ethics committee, with the approval number: 2023-209-01. Inclusion Criteria: (1) Diagnosis of Stage III Kummell’s disease based on clinical symptoms and imaging findings: In the CT images, an intervertebral cleft (IVC) is present, showing a fracture at the posterior edge of the vertebra. In MRI, there is low signal intensity on T1-weighted images, while on T2-weighted images, the cleft filled with gas or fluid exhibits either low or high signal intensity; (2) Bone density meeting the diagnostic criteria for osteoporosis as measured by dual-energy X-ray absorptiometry; (3) No symptoms of neurological impairment; (4) Involvement of only one responsible vertebra. Exclusion Criteria: (1) Patients with pathological vertebral fractures, spinal metastases, spinal tuberculosis, or other severe internal diseases; (2) Patients with severe cardiopulmonary dysfunction, coagulation disorders, or psychiatric conditions that would prevent tolerance of surgery; (3) Patients with a history of spinal surgery; (4) Patients with incomplete imaging data or lost to follow-up.
Grouping
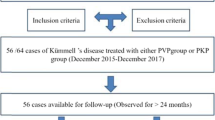
By applying exclusion and inclusion criteria, patients with Stage III KD without neurological symptoms were identified. Some underwent PVP surgery while others received PKP surgery. Based on the type of surgery, eligible patients were divided into the PKP and PVP groups, and preoperative and postoperative data were collected for both groups (Fig. 1).

Flowchart of study design
Surgical methods
The surgeries for both groups were performed by the same team of doctors, and all were conducted via a unilateral approach.
PKP method: (1) The patient is positioned prone on the operating table. Using C-arm fluoroscopy, the projection of the pedicle is located and marked, followed by disinfection and draping of the operative area. (2) A small incision of about 0.4 cm is made at the marked point under local anesthesia with 2% lidocaine. Under fluoroscopic guidance, a pedicle needle is inserted into the vertebral body to establish a working channel. 3.After successfully establishing the working channel, a balloon catheter was used to enter the injured vertebral intravertebral vacuum cleft (IVC) along the channel. The balloon pressure was maintained below 15 atm, using the balloon’s expansion to restore vertebral height to satisfaction and create a cavity for bone cement injection. The bone cement (polymethylmethacrylate cement) was prepared and, when it reached a stringy state, slowly injected into the vertebra under C-arm fluoroscopy using a 3.5 mm bone cement injector until the IVC was filled. After the bone cement had slightly set, the injection tube was removed, the puncture needle was withdrawn, the area was disinfected with iodophor, and the wound was dressed and bandaged.
PVP method: Similar to the PKP procedure but lacking the balloon expansion of the vertebra. After establishing the bone cement injection channel, the cement is injected directly until the entire vertebral fissure is filled. Once the bone cement has slightly set, the injection tube is withdrawn, the puncture needle is removed, the area is disinfected with iodophor, and the wound is dressed and bandaged.
Postoperative treatment
Postoperative treatment measures were identical for both groups. Patients were required to lie supine for 4–6 h immediately after surgery and wear lumbar support for appropriate mobility the day following surgery. For 1–2 months postoperatively, strict adherence to wearing lumbar support for ground activities was enforced, along with long-term regular treatment for osteoporosis after discharge. Since our hospital includes only Vitamin D, calcium carbonate, and bisphosphonates in the social medical insurance for osteoporosis treatment, the postoperative osteoporosis treatment plan was the same for both groups. Patients regularly used medications such as Vitamin D, calcium carbonate, and bisphosphonates for osteoporosis management.
Observational indicators
Clinical Efficacy Indicators: (1) VAS scores is used to assess the degree of pain in the lumbar/back or thoracic/back regions before surgery, one day post-surgery, and at the last follow-up. A score of 0 indicates no pain, while 10 represents the most severe pain. Scores of 0–3 are rated as excellent; 4–6 as good; and 7–10 as poor. ODI scores measures the severity of functional impairment before surgery, one day post-surgery, and at the last follow-up, with higher scores indicating more severe disability [7, 8]. (2) Surgical duration, (3) Volume of bone cement injected. (4) Distribution patterns of bone cement, including cluster type (clustered distribution within the vertebra with smooth edges), sponge type (uniformly diffused throughout the vertebra resembling a sponge), and mixed type (distribution between cluster and sponge types). (5) Rate of bone cement leakage.
Radiological Indicators: (1) Relative anterior height of the vertebra: Anterior height of the affected vertebra relative to the average height of the vertebrae above and below it, expressed as a percentage, measured on standing X-rays before surgery, one day post-surgery, and at the last follow-up [9]; (2) Cobb angle of the affected vertebra on standing X-ray before surgery, one day post-surgery, and at the last follow-up [9]( Fig. 2). To reduce measurement errors, each patient’s measurements are independently taken by two experienced spine surgeons and then averaged.

a: Anterior height of the vertebra above the injured vertebra. b: Anterior height of the injured vertebra. c: Anterior height of the vertebra below the injured vertebra; Cobb’s angle: Cobb’s angle in the sagittal plane of the injured vertebra (°)
Statistical methods
Data analysis was conducted using SPSS software, version 25.0. For quantitative data, the Shapiro-Wilk (SW) test was first used to assess normality. If data were normally distributed (p > 0.05), they were presented as mean ± standard deviation and compared using independent sample t-tests. If data were not normally distributed (p < 0.05), they were expressed as median (interquartile range) and compared using non-parametric rank-sum tests. Categorical data were expressed as percentages and analyzed using chi-square tests and Fisher’s exact test. A p-value of < 0.05 was considered statistically significant.
Results
Preoperative general data
A total of 53 patients were included based on the aforementioned criteria, with 25 in the PVP group and 28 in the PKP group. Both groups were followed up for an average of approximately 2 years, predominantly comprising elderly females. Vertebral injuries were mostly concentrated in the thoracolumbar region, with an average disease duration of about 4 months. The two groups showed comparability in terms of age, gender, injured segment, follow-up duration, bone mineral density (BMD), body mass index (BMI), preoperative VAS score, preoperative Oswestry Disability Index (ODI), and radiological indicators (all p > 0.05, detailed in Tables 1 and 2, and 3).
Clinical effect
All patients safely underwent surgery without serious complications such as nerve damage or acute pulmonary embolism. The duration of surgery and the volume of bone cement injected were significantly less in the PVP group than in the PKP group (p < 0.05). The distribution of bone cement was predominantly mixed in the PVP group (56%) and clumped in the PKP group (64.3%), with significant differences in distribution between the groups (p < 0.05). The leakage rate of bone cement was 40% in the PVP group, including one case where the cement leaked into the spinal canal, while it was 10.7% in the PKP group. There were no clinical symptoms in either group, and the leakage rate was lower in the PKP group (p < 0.05) (Table 4). The VAS scores both one day post-operatively and at the final follow-up were significantly reduced from preoperative scores within both groups (p < 0.001), with little change in scores from the first day post-operatively to the final follow-up (p > 0.05). There were no significant statistical differences in VAS scores between the groups either before surgery, one day after, or at the last follow-up (p > 0.05). Both PVP and PKP showed significant therapeutic effects in improving VAS scores, but there was no significant difference in efficacy between the groups. Similar changes were observed in the ODI scores as well (Table 2; Fig. 3).

Groups A and B represent the preoperative, postoperative, and final follow-up VAS and ODI scores for the two groups of patients (ns: no statistical difference. **: p < 0.001)
Radiological outcomes
Both groups showed improvement in the relative height of the anterior edge of the injured vertebra(%) and the sagittal Cobb angle one day post-surgery and at the last follow-up compared to pre-surgery (p < 0.05). Over time, there was a trend of gradual loss in vertebral height and an increase in Cobb angle. Post-surgery, improvements in vertebral height and Cobb angle were more significant in the PKP group compared to the PVP group (p < 0.05). However, the loss of vertebral height and increase in Cobb angle at the last follow-up were also more pronounced in the PKP group compared to the PVP group (p < 0.001). No significant statistical differences were found between the groups in the relative anterior height and sagittal Cobb angle of the injured vertebra pre-surgery and at the last follow-up (p > 0.05) (Table 3; Fig. 4).

A and B represent the relative anterior height of the vertebra and the displaced Cobb angle before surgery, after surgery, and at the final follow-up (ns: no significant statistical difference, *: p < 0.05)
Case presentation
Both PKP and PVP surgeries effectively improved the vertebral height and local Cobb angle of the injured vertebra. PKP showed a more significant early correction capability compared to PVP, but an increase in the Cobb angle at the final follow-up was also more pronounced compared to PVP (Figs. 5 and 6). In the PVP group, there was one instance of bone cement leakage into the spinal canal, although no neurological symptoms occurred (Fig. 7).

A 70-year-old female patient. Images A-C show preoperative MRI T1WI, MRI T2WI, and CT scans revealing gas-fluid levels in the T11 vertebra and a posterior vertebral fracture, diagnosed as Stage III Kummell’s disease without neurological injury. The patient underwent PVP surgery. Images D-F are lateral X-rays of the injured vertebra before surgery, one day post-surgery, and at the last follow-up, showing improvements in vertebral height and Cobb angle compared to pre-surgery. Although there was bone cement leakage, no clinical symptoms were exhibited

A 65-year-old female patient. Images A-C show preoperative MRI T2WI, MRI T1WI, and CT scans revealing gas-fluid levels in the T12 vertebra, with a fracture at the posterior edge of the vertebra but no neurological symptoms, diagnosed as Stage III Kummell’s disease without neurological injury. The patient underwent PKP surgery. Images D-F are lateral X-rays of the injured vertebra before surgery, one day post-surgery, and at the last follow-up, showing significant improvements in vertebral height and Cobb angle compared to pre-surgery. However, the Cobb angle increased at the last follow-up compared to immediately post-surgery

A 65-year-old female patient with Stage III Kummell’s disease (images A-C). After undergoing PVP surgery, bone cement leaked into the spinal canal, but it did not cause any corresponding clinical symptoms (images D-F)
Discussion
The clinical pathogenesis and etiology of KD remain unclear, thus many terms are used clinically, such as unhealed vertebral compression fractures, spinal pseudoarthrosis, delayed bone necrosis, post-fracture vertebral collapse, and intravertebral vacuum cleft (IVC) signs. The widely accepted mechanism involves ischemic necrosis of the vertebral body following trauma [10, 11]. Previous studies have shown that KD predominantly affects elderly women, with injuries mainly located in the thoracolumbar region [6], consistent with the findings of this study. Diagnosis primarily relies on radiological signs, and Ranjan et al. [12]. found that only a minority of cases have a typical history of KD. The intravertebral vacuum cleft (IVC), appearing as a non-radiopaque shadow in horizontal, linear, or crescent shapes, which is more prominently seen in anteroposterior views, this is considered a characteristic radiological feature of KD. CT is more sensitive to air in the IVC, while MRI is more sensitive to fluid; overall, MRI is the most effective tool for diagnosing IVC signs [13, 14]. The unknown mechanisms of the disease and the lack of detailed clinical classification, particularly for type III KD with posterior vertebral edge fractures, continue to make the treatment of stage III KD controversial. Some studies suggest that due to the susceptibility of vertebral posterior wall collapse and fracture during PVP and PKP surgeries, open surgery with internal fixation is preferred [15]. However, a meta-analysis by Lu et al. [16]. comparing the clinical efficacy of PKP alone and combined with short segment internal fixation for stage III KD without neurological damage found no significant difference in treatment outcomes or cement leakage rates. Given that KD patients are typically older and often suffer from severe osteoporosis and other underlying conditions, open surgeries pose a higher risk due to longer operation times, more bleeding, and longer bed rest, with the possibility of needing a second surgery due to loosening of internal fixations. Therefore, minimally invasive surgical treatments like PVP and PKP, which involve shorter operation times, less bleeding, and shorter bed rest, may be the preferred treatment for stage III KD without neurological damage.
This study found that both PVP and PKP surgeries effectively alleviated patients’ pain symptoms, significantly reducing the VAS scores for lumbar and back pain and the Oswestry Disability Index (ODI) scores compared to pre-surgery, with no significant statistical differences between the groups at any time points. This may be attributed to the stabilization of the fractured vertebra by the bone cement, which prevents abnormal movement due to intravertebral pseudoarthrosis or microfractures, restores vertebral height, improves spinal kyphosis, and alters intravertebral pressure [6, 16]. However, some patients still experienced residual lower back pain post-surgery, possibly related to surrounding soft tissue damage and incomplete correction of the kyphotic deformity. The PKP surgery took longer than the PVP surgery, mainly due to the additional step of balloon expansion, which is the biggest difference between the two methods. Our study observed that the average volume of bone cement injected in the PVP group was 2.7 ± 0.7 ml, which was less than the 3.5 ± 0.8 ml in the PKP group (p < 0.05), related to the increased space created by the balloon expansion within the vertebra. However, research shows that the volume of bone cement injected does not significantly correlate with symptom relief; injecting as little as 1.5 ml of bone cement can achieve satisfactory clinical outcomes, and excessive cement injection increases the risk of cement leakage, adjacent vertebral fractures, and subsequent vertebral collapse [17]. Therefore, it is unnecessary to overly focus on the volume of bone cement injected in clinical practice. Additionally, we have observed that for some patients with vertebral compression fractures, relieving pain was possible through vertebral biopsy without bone cement injection, suggesting that altering intravertebral pressure may play a role, though further research is needed to confirm these findings. In this study, differences were observed in the distribution of bone cement between the PKP and PVP groups. The PKP group primarily had a clustered distribution (64.3%), while the PVP group primarily had a mixed distribution (56%). This may be due to the presence of dense bone around the KD vertebral fissures, with some cement flowing through the gaps in the dense bone into the more porous bone, thus resulting in a mixed distribution for PVP. In contrast, PKP surgery involves balloon expansion, which compresses the surrounding porous bone, leading to poorer dispersion of the bone cement and a predominantly clustered distribution, as also noted in previous studies [17].
There were no postoperative complications other than cement leakage in the two groups of patients in this study, and none of the patients with cement leakage in either group developed clinical symptoms. Many studies have shown that balloon expansion in PKP compresses the surrounding porous bone, further sealing the fracture and thus reducing the rate of cement leakage compared to PVP [18, 19], a finding also noted in this study with leakage rates of 40% in PVP and 10.7% in PKP with PKP significantly lower than PVP (p < 0.05). Cement leakage remains a challenge in both PVP and PKP, potentially leading to catastrophic outcomes, especially in Stage III KD with posterior vertebral fractures, where the risk of cement leaking into the spinal canal significantly increases. This study noted one case of cement leakage into the spinal canal during PVP surgery, fortunately without severe clinical symptoms (Fig. 7), leading some scholars to advocate for open surgery in Stage III KD [15]. To reduce the rate of cement leakage, many new techniques such as mesh sacs, staggered cement injection, and graded cement modulation have emerged [20,21,22]. Reducing leakage rates is a crucial direction for the future development of PVP and PKP. This study indicates that PKP has a lower cement leakage rate and higher safety compared to PVP. However, Dai and Chang [17, 23], in a retrospective and a prospective study respectively, found no significant differences in cement leakage rates between PKP and PVP in treating asymptomatic KD, possibly because their cases primarily involved Stage I and II KD, which have a lower risk of cement leakage, and had a smaller sample size. No statistical differences were observed between PKP and PVP leakage rates, and this study also suffers from a small sample size, necessitating further large-scale research.
In terms of correcting spinal kyphotic deformities and restoring vertebral height, both the PKP and PVP groups showed significant improvements compared to preoperative conditions (p < 0.05), as reported in most previous studies [20, 23, 24]. However, we found that the immediate postoperative correction (1 day after surgery) was more pronounced in the PKP group, but the long-term corrective effects (at the final follow-up) were similar between both groups without significant statistical differences (p > 0.05). Over time, both PKP and PVP gradually lost their corrective effects, with PKP showing greater loss (p < 0.05), possibly related to the distribution of bone cement. In the PKP group, the cement predominantly had a clustered distribution, which as Gao [25] and others in a study of 841 cases have noted, uneven cement distribution increases stress on surrounding spongy bone, causing instability at the cement-bone interface, leading to shifts in the cement and resulting in the loss of vertebral height and increased local Cobb angle. Clinically, scraping off the hardened bone surfaces within vertebral fissures to increase cement dispersion and reduce the shift-induced height loss may help, but further research is needed to confirm the efficacy of such procedures. Although there was a slight loss of vertebral height in both groups during the study, no statistically significant differences were observed between the vertebral heights at the last follow-up and post-surgery (p > 0.05). Throughout the follow-up period, both PKP and PVP maintained vertebral stability to a certain extent. Furthermore, we believe that for elderly patients, the emphasis should not be overly placed on achieving perfect orthopedic outcomes. Instead, focus should be on relieving clinical symptoms of pain and functional impairment, as well as on the safety of the surgery. Overall, for Stage III Kummell’s disease without neurological symptoms, both PKP and PVP have achieved good clinical outcomes, with comparable efficacy, minimal trauma, and quick recovery, making them preferred surgical options for elderly patients. PKP, although more expensive, has a lower rate of cement leakage and is safer than PVP. We emphasize that both efficacy and safety are crucial, particularly the safety of surgeries in elderly patients, recommending PKP if economically feasible.
Nevertheless, this study has limitations, including its retrospective nature and small sample size, which might introduce bias. To validate our findings, further large-scale, multicenter, randomized controlled trials are necessary. Additionally, as follow-up duration extends, differences in long-term corrective outcomes between the groups may emerge, necessitating further follow-up studies.
Conclusions
According to the results of this study, both PVP and PKP achieved good clinical outcomes and safety for Stage III Kummell’s disease without neurological symptoms. There was little difference in the clinical efficacy between the two methods. However, PKP had a lower rate of bone cement leakage and higher safety compared to PVP. Therefore, if economic conditions allow, PKP is recommended for patients.
Data availability
Data cannot be shared openly but are available on request from authors
Abbreviations
- PVP:
-
Percutaneous vertebroplasty
- PKP:
-
Percutaneous kyphoplasty
- VAS:
-
Visual analogue scale
- KD:
-
Kummell’s disease
- OVCF:
-
Osteoporotic vertebral compression fractures
- IVC:
-
Intravertebral vacuum cleft
- BMD:
-
Bone mineral density
- BMI:
-
Body mas index
- atm:
-
Standard atmospheric pressure
References
Kummell H. Die rarefizierende ostitis Der wirbelkorper [J]. Dtsch Med 1895; 21: 180–1.
Niu J, Song D, Zhou H, et al. Percutaneous kyphoplasty for the treatment of osteoporotic vertebral fractures with intravertebral fluid or air: a comparative study [J]. Clin Spine Surg. 2016;30:367–73.
Li KC, Wang TU, Kun FC. Staging of Kümmell’ s disease. J Musculoskelet Res. 2004;8:43–55.
Li H, Liang CZ, Chen QX. Kummell’s disease, an uncommon and complicated spinal disorder: a review. J Int Med Res. 2012;40(2):406–14.
Jong-Hwa PJWP, Jun JH, et al. Kümmell’s Disease treated with Percutaneous Vertebroplasty: Minimum 1 Year Follow-Up.[J]. Korean J Neurotrauma. 2017;13:119–23.
Zhang B, Chen G, Yang X, Fan T, Chen Z. Percutaneous kyphoplasty versus percutaneous vertebroplasty for neurologically intact osteoporotic Kummell’s disease: a systematic review and metaanalysis. Glob Spine J. 2022;12(2):308–22.
Khan M, Kushchayev SV. Percutaneous vertebral body augmentations: the state of art. Neuroimaging Clin N Am. 2019;29(4):495–513.
Zhang Y, Shi L, Tang P, Zhang L. Comparison of the Efficacy between two micro-operative therapies of old patients with osteoporotic vertebral Compression fracture: a Network Meta-Analysis. J Cell Biochem. 2017;118(10):3205–12.
Chen J, Luo A, Wang C. The use of spiral cement injector for Percutaneous Vertebroplasty to treat Kümmell Disease: a retrospective study. World Neurosurg. 2024;186:e235–42.
Prakash, Prabhu LV, Saralaya VV, et al. Vertebral body integrity: a review of various anatomical factors involved in the lumbar region. Osteoporos Int. 2007;18(7):891–903.
Kim Yoon-Chung, Kim Young-Hoon,Ha Kee-Yong, Pathomechanism of intravertebral clefts in osteoporotic compression fractures of the spine[. J] Spine J. 2014; 14: 659–66.
Ranjan M, Mahadevan A, Prasad C, et al. Kümmell’s disease - uncommon or underreported disease: a clinicopathological account of a case and review of literature. J Neurosci Rural Pract. 2013;4(4):439–42.
Wu AM, Chi YL, Ni WF. Vertebral compression fracture with intravertebral vacuum cleft sign: pathogenesis, image, and surgical intervention. Asian Spine J. 2013;7(2):148–55.
Lim Jeongwook C, Seung-Won Y, Jin-Young, et al. Posttraumatic Delayed Vertebral Collapse: Kummell’s Disease [J] J Korean Neurosurg Soc. 2018;61:1–9.
Li KC, Li AF, Hsieh CH, Liao TH, Chen CH. Another option to treat Kümmell’s disease with cord compression. Eur Spine J. 2007;16(9):1479–87.
Lu W, Wang L, Xie C, et al. Analysis of percutaneous kyphoplasty or short-segmental fixation combined with vertebroplasty in the treatment of Kummell disease. J Orthop Surg Res. 2019;14(1):311.
Chang JZ, Bei MJ, Shu DP, et al. Comparison of the clinical outcomes of percutaneous vertebroplasty vs. kyphoplasty for the treatment of osteoporotic Kümmell’s disease:a prospective cohort study. BMC Musculoskelet Disord. 2020;21(1):238.
Wang Yajian L, Bo S, Zhenwei et al. Comparative Efficacy of Three Minimally Invasive Procedures for Kümmell’s Disease: A Systematic Review and Network Meta-Analysis.[J].Front Surg. 2022; 9: 893404.
Ee GW, Lei J, Guo CM, et al. Comparison of clinical outcomes and radiographic measurements in 4 different treatment modalities for osteoporotic Compression fractures: retrospective analysis. J Spinal Disord Tech. 2015;28(6):E328–35.
Zhang B, Chen G, Yang X, Fan T, Chen Z. Percutaneous Kyphoplasty Versus Percutaneous Vertebroplasty for Neurologically Intact Osteoporotic Kümmell’s Disease: a systematic review and Meta-analysis. Global Spine J. 2022;12(2):308–22.
Duan ZK, Zou JF, He XL, Huang CD, He CJ. Bone-filling mesh container versus percutaneous kyphoplasty in treating Kümmell’s disease. Arch Osteoporos. 2019;14(1):109.
He CJ, Liu GD. Comparison of the efficacy and safety of bone filling mesh container and simple percutaneous balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Pain Physician. 2018;21:259–67.
Dai SQ, Qin RQ, Shi X, Yang HL. Percutaneous vertebroplasty versus kyphoplasty for the treatment of neurologically intact osteoporotic Kümmell’s disease. BMC Surg. 2021;21(1):65.
Feng XY-HC, Zhang, Liang, et al. Percutaneous kyphoplasty treatment evaluation for patients with Kümmell disease based on a two-year follow-up. [J] Exp Ther Med. 2018;16:3617–22.
Gao X, Du J, Zhang Y, et al. Predictive factors for bone cement displacement following percutaneous vertebral augmentation in Kümmell’s Disease. J Clin Med. 2022;11(24):7479.
Funding
This study did not receive any direct financial support.
Author information
Authors and Affiliations
Contributions
SC and HC provided the experimental design. The collection of experimental data and manuscript writing were conducted by SC and DY. ZZ and CZ analyzed and interpreted the data. SC and HAMZA completed the translation of the manuscript. HC made the final revisions.LH evaluated the statistical methods. All authors contributed to the final version of the manuscript and agreed to its publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We received ethical approval from the Ethics Committee of the First Clinical Medical College of Three Gorges University. All patient medical information was anonymized, thus waiving the requirement for informed consent. Our study was conducted in accordance with the principles of the Declaration of Helsinki.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, S., Yang, D., Zhuo, C. et al. Comparative analysis of percutaneous vertebroplasty and kyphoplasty in the treatment of Stage III Kummell’s disease without neurological symptoms: a retrospective study. J Orthop Surg Res 19, 515 (2024). https://doi.org/10.1186/s13018-024-05019-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-05019-w