
Abstract
Background
This study aims to investigate the efficacy of five analgesic strategies combined with conventional physiotherapy program (CPT) in managing chronic shoulder pain.
Methods
Two authors independently screened studies, extracted data using a pre-formatted chart, and assessed bias using the Cochrane Risk of Bias tool. A network meta-analysis was performed by the Stata 17.0 and R 4.3.2 software.
Results
A total of 14 studies with 862 subjects were identified. These analgesic strategies included extracorporeal shock wave therapy (ESWT), suprascapular nerve block (SSNB), corticosteroid injection (CSI), hyaluronic acid injection (HAI), and kinesio taping (KT). ESWT plus CPT was the most efficient intervention in alleviating pain intensity and improving physical function. SSNB plus CPT was the optimal intervention in improving shoulder mobility. Compared to CPT alone, CSI + CPT only significantly improved the SPADI total score, but showed no difference in pain intensity or shoulder mobility. HAI + CPT showed no significant difference in improving pain intensity, physical function, or shoulder mobility compared to CPT alone. Adding KT to CPT did not yield additional benefits in improving shoulder mobility.
Conclusion
Overall, in managing chronic shoulder pain, ESWT + CPT was the most effective intervention for reducing pain intensity and improving physical function. SSNB + CPT was optimal for enhancing shoulder mobility. Future rigorous clinical trials with larger sample sizes and higher methodological rigor are strongly required to confirm the current results.
Similar content being viewed by others


Introduction
Shoulder pain is the third most common musculoskeletal complaint, with a lifetime incidence of up to 67%, significantly impacting patients’ quality of life and posing a massive socio-economic burden on the healthcare system [1, 2]. Chronic shoulder pain, defined as shoulder pain persisting for more than three months, has a significant impact on functional ability, psychosocial well-being, and metabolic stress [3]. Chronic shoulder pain is caused by multiple shoulder conditions including subacromial impingement syndrome, tendinopathy, rotator cuff tears, and adhesive capsulitis [2]. Subacromial impingement syndrome, primarily caused by subacromial pathology, is a leading contributor to shoulder pain [4]. Tendinopathy may arise due to repeated shoulder movements, particularly during overhead activities or heavy lifting [5]. Rotator cuff tears often lead to shoulder pain and functional impairment, necessitating treatment tailored to the severity, including conservative management or surgical repair [6]. Adhesive capsulitis is characterized by pain and stiffness, commonly associated with synovitis and contracture of the synovial capsule [7]. These shoulder conditions can cause chronic shoulder pain and are typically accompanied by stiffness, reduced range of motion, and limited participation [8].
The complex anatomy of the shoulder joint, the wide range of pathogenic factors, and the absence of standardized diagnostic criteria pose a significant dilemma for diagnose [9,10,11,12]. Consequently, the term “non-specific shoulder pain” is frequently used in both clinical practice and research studies [13]. A review has emphasized the need for future research targeting undivided subjects with “general” shoulder pain [14]. Besides, several such studies already yielding valuable clinical insights [15,16,17,18]. For example, a recent NMA compared the effectiveness of different exercise therapies in alleviating chronic shoulder pain [15]. Thus, performing a network meta-analysis based solely on chronic shoulder pain is reasonable.
Several conservative treatments of chronic shoulder pain have been proposed and assessed, such as non-steroidal anti-inflammatory drugs (NSAIDs), conventional physiotherapy program (CPT), and other analgesic strategies. NSAIDs are not always effective and may increase the risk of cardiovascular, gastrointestinal, liver or renal complications [9, 19]. CPT, the first line therapy, includes exercise therapy, physical factor therapy, joint mobilization, massage therapy, and stretching [20, 21]. It is helpful in alleviating pain, increasing muscle strength and joint stability, and facilitating function recovery [22, 23]. Additionally, CPT can rectify biomechanical issues by improving muscle extensibility, increasing range of motion, enhancing stability of the rotator cuff muscles, and correcting scapulohumeral rhythm [24, 25]. Recent evidence unveiled that there was no significant difference in reducing pain and improving physical function between physiotherapy and surgery for adults with shoulder pain [26,27,28]. These evidence also strengthen the necessity of CPT in the management of shoulder pain. Nevertheless, it also has some limitations. For instance, the efficacy of exercise may be compromised due to inherent challenges such as insufficient self-initiative and inadequate external supervision. Furthermore, manual therapy may transiently exacerbate pain and symptoms of patients with shoulder pain. Therefore, it is crucial to explore alternative treatments to complement or improve the therapeutic efficacy of CPT [29].
Besides NSAIDs and CPT, various analgesic strategies are widely used in clinical practice for treating chronic shoulder pain, such as extracorporeal shock wave therapy (ESWT), suprascapular nerve block (SSNB), corticosteroid injection (CSI), hyaluronic acid injection (HAI), and kinesio taping (KT). Numerous randomized controlled trials (RCTs) and reviews have demonstrated that these interventions can alleviate pain and improve joint function in individuals with shoulder pain [20, 21, 26,27,28, 30,31,32,33,34,35]. However, these interventions may be limited in their long-term efficacy as they offer only temporary pain relief and anti-inflammatory effects without rectifying fundamental biomechanical issues. Recurrence of symptoms post-intervention is common due to biomechanical issues, such as imbalance in the rotator cuff muscles, postural dysfunction, and changes in shoulder-thoracic kinematics.
Recent well-designed RCTs have proven that combining CPT with analgesic strategies results in better outcomes than CPT alone. Previous network meta-analyses (NMAs) have compared the efficacy of various shoulder joint drug injections for shoulder disorders. However, they have not compared the effectiveness of different analgesic strategies when combined with CPT. This gap hinders the selection and promotion of the optimal treatment protocols in clinical practice. Therefore, this study aims to conduct a systematic review and NMA to evaluate the efficacy of five analgesic strategies combined with CPT in treating chronic shoulder pain. The findings will provide evidence-based clinical recommendations.
Methods
Protocol and registration
This study was conducted by Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Network Meta-Analysis (PRISMA-NMA) [36]. A prospective protocol for the NMA has been reported on PROSPERO (CRD 42024519473).
Search strategy
We systematically searched Pubmed, Web of Science, Embase, and Cochrane Library from their inceptions to April 15, 2024. The search terms used were: “Shoulder Pain”, “Rotator Cuff Injury”, “shoulder impingement syndrome”, “adhesive capsulitis”, “frozen shoulder”, “shoulder girdle”, “physiotherapy”, “physical therapy”, “steroid”, “corticosteroid”, “extracorporeal shock wave therapy”, “kinesio taping”, “kinesiology taping”, “Suprascapular Nerve Block”, “suprascapular nerve blocks”, “hyaluronic acid”, “randomized”, “random”, “randomly”, and “randomised”. Additionally, the references cited in the included articles were traced to identify any further eligible studies. The specific search strategies are given in Table S1.
Inclusion criteria
-
I.
Type of study: RCTs with parallel design were included.
-
II.
Subjects: adults (≥ 18 years) were diagnosed with shoulder pain lasting at least 3 months, including rotator cuff tendinopathy, shoulder impingement syndrome, frozen shoulder, adhesive capsulitis, non-specific shoulder pain, and shoulder myofascial pain.
-
III.
Types of interventions: acceptable interventions were mainly various analgesic strategies combined with CPT. Analgesic strategies included CSI, HAI, SSNB, ESWT, and KT.
-
IV.
Comparison: CPT alone or intercomparison between interventions.
-
V.
Outcome measures: outcomes encompassed data on pain intensity assessed by Visual Analogue Scale (VAS) and Shoulder Pain and Disability Index pain (SPADI pain), physical function measured by SPADI disability and SPADI total, and shoulder mobility measured by shoulder range of motion (ROM).
Exclusion criteria
Studies that met any of the following criteria were strictly excluded: (1) studies specifically focused on patients with post-mastectomy shoulder pain; (2) studies published as conference abstracts, trial registry records, animal studies, reviews, meta-analyses, protocols, case reports, or letters; (3) incomplete trial data; (4) irrelevant trial outcome indicators; (5) inappropriate interventions; (6) insufficient patient information; (7) non-English studies.
Screening and data extraction
The retrieved articles were uploaded into Endnote X9 software, and then duplicates were removed. Two authors independently scrutinized the titles and abstracts for an initial screening, and conducted a meticulous full-text reading of selected RCTs for the final decision. The following data were collected and summarized by two authors using a pre-formatted chart: first author, publication year, country, study design, sample size, participant age, disease type, pain duration, intervention protocols (intervention modalities and duration), and outcome assessments (VAS, SPADI pain, SPADI total, SPADI disability, and shoulder ROM). Any discrepancies were resolved through collaboration with other authors. If complete data were not available, we contacted the corresponding author for missing information. When necessary, the mean and standard deviation were calculated using the Cochrane Handbook formulas based on the baseline and outcome data.
Risk of bias
Two authors independently performed quality assessment of the included studies via the Cochrane Collaboration’s tool. Seven items of bias were as follows: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Any disagreements were resolved by achieving a consensus. The risk of bias for each domain was rated as low, unclear, or high. Studies with low bias risk in three or more domains were rated moderate to high quality. Publication bias was evaluated using a comparison-adjusted funnel plot and Egger’s test.
Data synthesis and analysis
A frequentist NMA using random-effects model was adopted to pool direct and indirect evidence simultaneously. All analyses were achieved using Stata/MP statistical software version 17.0, R statistical software version 4.3.2, and RStudio statistical software version 22023.09.1–494 [37,38,39]. Mean difference (MD) with a 95% confidence interval (CI) was used to evaluate the effect size of the continuous variables. If a closed loop was formed, we examined statistical inconsistency between direct and indirect evidence using local (the node-splitting technique) and global (the design-by-treatment interaction technique) models [40]. If P > 0.05, it suggested that there was no statistically significant difference between the two kinds of evidence, and a consistency model analysis was used for analysis [41]. A network plot was created to show the relationships among the different interventions. The size of nodes reflects the sample size of each intervention, and the thickness of lines corresponds to the quantity of RCTs with direct comparisons. Then, a league table was created to present the outcome for all paired comparisons, incorporating both direct and indirect comparisons. Subsequently, the surface under the cumulative ranking surve (SUCRA) probabilities were computed to compare the efficacy of different treatment approaches for each outcome. And a larger SUCRA value suggests a better effect of the intervention. Then, cumulative probability line charts were created. Finally, the potential publication bias in NMA was examined using a comparison-adjusted funnel plot and Egger’s test. Egger’s test was performed using Rstudio, and if P > 0.05, it indicated that there was no significant publication bias.
Results
Study selection
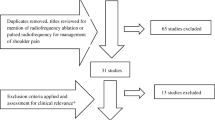
The preliminary search identified 1248 records, of which 527 duplicate records were removed. After reviewing titles and abstracts, 48 studies remained. After excluding 1 unavailable studies, the full texts of the reserved 47 studies were further evaluated for their eligibility. Following the screening criteria, 14 studies were selected for our NMA with a total of 862 patients [42,43,44,45,46,47,48,49,50,51,52,53,54,55]. The process of literature screening is shown in Fig. 1.

Flow diagram of studies selection
Study characteristics
A total of 14 eligible studies [42,43,44,45,46,47,48,49,50,51,52,53,54,55] and 6 interventions fulfilled the inclusion criteria and were included for analysis. The different interventions of included studies were defined in Table 1. The characteristics of the included RCTs are presented in Table 2. They were carried out in 6 different countries and published from 2011 to 2024. Egypt has contributed four articles, the highest number among all countries. The sample sizes spanned from 30 to 97. The average age of patients ranged from 30.47 to 71.3 years old. Participants in the included studies were diagnosed with chronic shoulder pain. Multiple studies reported the effectiveness of different interventions: 5 studies for “CSI + CPT” [42, 44, 51,52,53], 5 studies for “HAI + CPT” [43, 45, 46, 49, 55], 2 studies for “SSNB + CPT” [42, 51], 4 studies for “ESWT + CPT” [47, 50, 52, 54], 1 studies for “KT + CPT” [48], and 14 studies for “CPT” [42,43,44,45,46,47,48,49,50,51,52,53,54,55]. The duration of intervention in the included studies varied from 4 weeks to 12 weeks, including 4 weeks for 4 studies [47, 50, 52, 54], 6 weeks for 2 studies [44, 48], 8 weeks for 1 studies [53], and 12 weeks for 7 studies [42, 43, 45, 46, 49, 51, 55]. The indicators of pain intensity encompassed VAS score and SPADI pain score. VAS score was reported in 5 studies [47, 50, 51, 53, 55], and SPADI pain score was reported in 6 studies [42,43,44, 53,54,55]. The indicators of physical function encompassed SPADI disability score and SPADI total score. The SPADI disability score was reported in 6 studies [42,43,44, 53,54,55], while the SPADI total score was reported in 8 studies [42,43,44, 51,52,53,54,55]. The indicators of shoulder mobility included flexion, abduction, and external rotation ROM. The flexion ROM was measured in 8 studies [42, 47, 48, 50,51,52,53, 55]; the abduction ROM was reported in 8 studies [42, 47, 48, 50,51,52,53, 55], and the external rotation ROM was reported in 9 studies [42, 45,46,47, 49,50,51, 53, 55].
Quality assessment
Among all the included studies, eight (57.1%) studies [43, 47, 48, 50, 52,53,54,55] used a computer or a random number table and were rated as low risk in random sequence generation. Five studies [42, 44,45,46, 51] lacked a clear description of the random allocation method and were assessed as unclear risk. Five (35.7%) studies [48, 50, 52, 53, 55] used a sealed envelope to conceal assignment scheme and were judged as low risk in allocation concealment. The remaining nine studies [42,43,44,45,46,47, 49, 51, 54] presented uncertain risk due to a lack of clear description of the allocation concealment. In blinding participants and personnel, ten studies had unclear risk [42,43,44, 46,47,48, 50, 52,53,54], and four studies had high risk [45, 49, 51, 55]. Five RCTs [50, 52,53,54,55] blinded the outcome evaluators. One study [44] was rated as high attrition bias owing to a dropout rate exceeding 20%, while three studies had unclear risk, and ten studies [42, 43, 46, 48, 50,51,52,53,54,55] had low risk in this aspect. All included studies were assessed as low risk in reporting bias. Other bias were evaluated as unclear risk in all studies. In summary, six studies were rated as high quality [48, 50, 52,53,54,55], one studies [43] were rated as moderate quality, and seven studies were rated as low quality [42, 44,45,46,47, 49, 51]. The funnel plots were symmetrical, and the P values of Egger’s test were exceeding 0.05, suggesting the absence of publication bias among the studies. Risk of bias assessment of the studies is illustrated in Fig. 2.

Risk of bias. (A) Risk of bias summary; (B) Risk of bias graph
Network meta-analysis
Pain intensity
Five studies with 362 subjects assessed the efficacy of 5 interventions in reducing VAS score, and the network plot is depicted in Fig. 3A. The VAS score is commonly used to measure pain intensity, and a higher score signifies greater pain intensity. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.15; local: P > 0.05) (Table S2). Figure 4A is the league table of VAS, presenting the two-by-two comparison matrix for reducing VAS score. Compared with CPT, SSNB + CPT (MD: -0.56; 95% CI: -0.96 to -0.16) and ESWT + CPT (MD: -1.06; 95% CI: -1.40 to -0.71) had significant effects on reducing VAS score. ESWT + CPT was significantly more effective than CSI + CPT (MD: 0.84; 95% CI: 0.24 to 1.43). As shown in Fig. 4B, results of SUCRA analysis unveiled that ESWT + CPT had the highest probability of being best (95.1%), followed by SSNB + CPT (61.5%), HAI + CPT (57.8%), CSI + CPT (27.8%), and CPT (7.8%). We were unable to identify publication bias using a funnel plot or Egger’s test because the number of included studies in this outcome was less than 10.

The network plots. (A) VAS; (B) SPADI pain/SPADI disability; (C) SPADI total; (D) Flexion; (E) Abduction; (F) External rotation

Visual Analogue Scale score (VAS). (A) The league table of VAS. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD < 0 suggests that this intervention is more effective in reducing VAS score compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of VAS
A total of 6 with 316 patients were included to compare the effects of 5 interventions on SPADI pain score in subjects with shoulder pain, and the network plot is shown in Fig. 3B. The SPADI questionnaire is a standardized tool used to assess pain and functional limitations in individuals with shoulder problems. It consists of two subscales: the Pain subscale and the Disability subscale. A higher SPADI pain score signifies more severe pain intensity. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.84; local: P > 0.05) (Table S2). Figure 5A is the league table of SPADI pain, presenting the two-by-two comparison matrix for reducing SPADI pain score. Compared with CPT, SSNB + CPT (MD: -12.60; 95% CI: -19.79 to -5.41) and ESWT + CPT (MD: -30.53; 95% CI: -36.94 to -24.12) had significant effects on reducing SPADI pain score. ESWT + CPT was significantly more effective than CSI + CPT (MD: 27.61; 95% CI: 19.32 to 35.90), HAI + CPT (MD: 29.84; 95% CI: 20.21 to 39.46), and SSNB + CPT (MD: 17.93; 95% CI: 8.30 to 27.56). As shown in Fig. 5B, the findings of SUCRA analysis indicated that ESWT + CPT had the highest probability of being best (100.0%), followed by SSNB + CPT (74.6%), CSI + CPT (38.8%), HAI + CPT (22.3%), and CPT (14.3%). We were unable to identify publication bias using a funnel plot or Egger’s test because the number of included studies in this outcome was less than 10.

SPADI pain. (A) The league table of SPADI pain. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD < 0 suggests that this intervention is more effective in reducing SPADI pain score compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of SPADI pain
Physical function
A total of 6 with 316 subjects were included to compare the effects of 5 interventions on SPADI disability score in patients with shoulder pain, and the network plot is shown in Fig. 3B. A higher SPADI disability score indicates more severe disabilities. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.14; local: P > 0.05) (Table S2). Figure 6A is the league table of SPADI disability, presenting the two-by-two comparison matrix for reducing SPADI disability score. ESWT + CPT was significantly more effective than HAI + CPT (MD: 23.87; 95% CI: 1.03 to 46.71) and CPT (MD: -25.25; 95% CI: -42.96 to -7.54). As shown in Fig. 6B, outcomes of SUCRA analysis unveiled that ESWT + CPT had the highest probability of being best (96.2%), followed by SSNB + CPT (55.6%), CSI + CPT (52.4%), HAI + CPT (28.1%), and CPT (17.6%). Funnel plot and Egger’s test were not performed because the number of included studies in this outcome was less than 10.

SPADI disability. (A) The league table of SPADI disability. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD < 0 suggests that this intervention is more effective in reducing SPADI disability score compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of SPADI disability
Eight studies with 473 subjects assessed the efficacy of 5 interventions in reducing SPADI total score, and the network plot is shown in Fig. 3C. A higher total SPADI score indicates poorer shoulder function. The design-by-treatment interaction model did not detect any inconsistency (P = 0.32). However, small percentages of local inconsistency were observed between some comparisons in SPADI total (1/6 loops) (Table S2). The league table of SPADI total is shown in Fig. 7A which exhibits the two-by-two comparison matrix for reducing SPADI total score. Compared with CPT, CSI + CPT (MD: -8.50; 95% CI: -16.21 to -0.78) and ESWT + CPT (MD: -17.07; 95% CI: -28.32 to -5.82) had significant effects on reducing SPADI total score. As shown in Fig. 7B, results of SUCRA analysis unveiled that ESWT + CPT had the highest probability of being best (94.6%), followed by CSI + CPT (62.6%), SSNB + CPT (54.6%), HAI + CPT (24.0%), and CPT (14.2%). The symmetrical funnel plot and Egger’s test (P = 0.61) indicated that there was no significant publication bias (Fig. 7C).

SPADI total. (A) The league table of SPADI total. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD < 0 suggests that this intervention is more effective in reducing SPADI total score compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of SPADI total; (C) The funnel plots of SPADI total
Shoulder mobility
Eight studies with 529 subjects examined the efficacy of 6 interventions in improving flexion ROM, and the network plot is shown in Fig. 3D. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.56; local: P > 0.05) (Table S2). The league table of flexion is shown in Fig. 8A, which presents the two-by-two comparison matrix for improving flexion ROM. Compared with CPT, SSNB + CPT (MD: 15.20; 95% CI: 1.56 to 28.85), and ESWT + CPT (MD: 14.37; 95% CI: 3.06 to 25.68) had significant effects on improving flexion ROM. As shown in Fig. 8B, results of SUCRA analysis indicated that SSNB + CPT had the highest probability of being best (81.2%), followed by ESWT + CPT (78.1%), CSI + CPT (49.4%), HAI + CPT (43.5%), KT + CPT (30.3%), and CPT (17.5%). The symmetrical funnel plot and Egger’s test (P = 0.74) indicated that there was no significant publication bias (Fig. 8C).

Flexion. (A) The league table of flexion. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD > 0 suggests that this intervention is more effective in reducing flexion ROM compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of flexion; (C) The funnel plots of flexion
Eight studies with 529 subjects assessed the efficacy of 6 interventions in improving abduction ROM, and the network plot is shown in Fig. 3E. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.67; local: P > 0.05) (Table S2). Figure 9A is the league table of abduction, showing the two-by-two comparison matrix for improving abduction ROM. Compared with CPT, SSNB + CPT (MD: 22.02; 95% CI: 4.70 to 39.35), and ESWT + CPT (MD: 16.58; 95% CI: 1.69 to 31.46) had significant effects on improving abduction ROM. As shown in Fig. 9B, outcomes of SUCRA analysis revealed that SSNB + CPT had the highest probability of being best (84.5%), followed by ESWT + CPT (70.2%), HAI + CPT (45.5%), CSI + CPT (44.2%), KT + CPT (40.8%), and CPT (14.9%). The symmetrical funnel plot and Egger’s test (P = 0.77) indicated that there was no significant publication bias (Fig. 9C).

Abduction. (A) The league table of abduction. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD > 0 suggests that this intervention is more effective in reducing abduction ROM compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of abduction; (C) The funnel plots of abduction
Nine studies with 620 subjects evaluated the efficacy of 5 interventions in improving external rotation ROM, and the network plot is shown in Fig. 3F. Both the design-by-treatment interaction model and the node-splitting method did not detect any inconsistency (global: P = 0.71; local: P > 0.05) (Table S2). Figure 10A is the league table of abduction, displaying the two-by-two comparison matrix for improving external rotation ROM. Compared with CPT, SSNB + CPT (MD: 16.48; 95% CI: 8.08 to 24.88), and ESWT + CPT (MD: 12.46; 95% CI: 4.32 to 20.60) showed significant improvement in external rotation ROM. SSNB + CPT was significantly more effective than CSI + CPT (MD: -11.32; 95% CI: -19.67 to -2.97) and HAI + CPT (MD: -15.41; 95% CI: -25.74 to -5.08). Compared with HAI + CPT, ESWT + CPT (MD: -11.39; 95% CI: -21.48 to -1.31) had significant effects on improving external rotation ROM. As shown in Fig. 10B, results of SUCRA analysis confirmed that SSNB + CPT had the highest probability of being best (93.5%), followed by ESWT + CPT (78.4%), CSI + CPT (45.0%), HAI + CPT (21.7%), and CPT (11.4%). The symmetrical funnel plot and Egger’s test (P = 0.94) indicated that there was no significant publication bias (Fig. 10C).

External rotation. (A) The league table of external rotation. MD with a 95% CI was used to evaluate the effect size. The comparisons in the lower left triangle should be read in a left-to-right manner. MD > 0 suggests that this intervention is more effective in reducing external rotation ROM compared to other interventions. Data marked with an asterisk (*) indicates significant group differences (P < 0.05); (B) Cumulative probability line chart of external rotation; (C) The funnel plots of external rotation
Discussion
To the best of our knowledge, this is the first systematic review and NMA to examine the therapeutic effects of five analgesic strategies combined with CPT for chronic shoulder pain. NMA can compare multiple treatments by combining direct and indirect evidence and perform relative ranking. According to the results of NMA, ESWT + CPT ranked highest in alleviating pain intensity and improving physical function compared to other interventions + CPT; SSNB + CPT was the best intervention in improving shoulder mobility. Compared to CPT alone, ESWT + CPT significantly improved pain intensity, physical function, and shoulder mobility; SSNB + CPT significantly improved pain intensity and shoulder mobility; CSI + CPT significantly improved the SPADI total score in patients with chronic shoulder pain, but showed no difference in pain intensity or shoulder mobility. HAI + CPT showed no significant difference in improving pain intensity, physical function, or shoulder mobility compared to CPT alone. The addition of KT to CPT had no significant effect on improving shoulder mobility.
Chronic shoulder pain is caused by diverse pathologies like tendon tears, tendinopathy, ligament instability, bursitis, and arthropathy, posing significant challenges for clinical management [17]. Effective management requires integrating multiple intervention methods, as comprehensive approaches often have more effective and longer-lasting effects than single treatments. CPT is a multimodal approach that includes exercise therapy, physical factor therapy, joint mobilization, massage therapy, and stretching [59]. Exercise is a central component of CPT and is strongly recommended as the initial approach for alleviating pain, enhancing mobility, and improving function in patients with subacromial shoulder pain [24, 60]. Based on surveys, in the rehabilitation of musculoskeletal shoulder issues, the following principles are commonly applied: patients are permitted to experience mild discomfort (rated below 5/10 on a VAS) during exercise sessions, which should include some resistance. Further, the expected duration of exercise spans 12 weeks [61, 62]. However, exercise often causes discomfort and hinders patients from fully engaging in the rehabilitation program. Pain relief facilitates patients to engage CPT, consequently enhancing overall effectiveness. Consequently, the combined application of analgesic strategies and CPT is gaining popularity in the management of chronic shoulder pain.
We found that ESWT + CPT ranked highest in alleviating pain intensity and improving physical function compared to other interventions + CPT. The greater effectiveness of the combined approach can be attributed to the fact that physical therapists use ESWT before addressing biomechanical issues with CPT. CPT can increase subacromial space, enhance movement control, restore normal scapulohumeral rhythm, improve proprioception, and ultimately improve shoulder joint function [22, 23]. Pain can restrict shoulder joint mobility by inducing arthrogenic muscle inhibition [63]. Therefore, preemptively addressing pain prior to initiating exercise programs can enhance effectiveness in reducing pain-related functional impairments over the short and medium-term [64]. There are two main hypotheses explaining the analgesic effect of ESWT. One of the mechanisms, known as the hyper-stimulation theory, suggests that ESWT induces the release of analgesic molecules by activating the descending inhibitory system, thereby alleviating pain [65]. Secondly, ESWT may lower the concentration of substance P levels in the target tissue and dorsal root ganglia, thereby impairing the pain transmission to the brainstem. Furthermore, the interstitial and extracellular responses caused by the shock wave can produce multiple biological effects, including vascularization, protein biosynthesis, cell proliferation, neuroprotection, and chondroprotection [66]. These biological effects result in long-term improvements in pain and function. A recent RCT demonstrated that in patients with chronic shoulder pain, ESWT + exercise exhibited greater efficacy in reducing pain intensity compared to rehabilitation alone, which was consistent with our outcome [67].
Compared to CPT alone, SSNB + CPT significantly improved pain reduction and shoulder mobility, but no significant differences were observed in improving physical function. Recent research has shown that continuous SSNB combined with intensive rehabilitation is an effective treatment for patients with chronic adhesive capsulitis unresponsive to conventional therapies [68]. Parashar et al. also suggested that combining SSNB with non-invasive rehabilitation was more effective for treating idiopathic frozen shoulder than non-invasive rehabilitation alone, aligning with our findings [69].The suprascapular nerve supplies sensory fibers to around 70% of the shoulder joint and directly innervates the supraspinatus and infraspinatus muscles [70]. SSNB can alleviate pain and improve shoulder joint motion by blocking the suprascapular nerve [71]. Previous research on adhesive capsulitis showed that the effects of SSNB surpassed the pharmacological effects of anesthetics, potentially due to desensitization from reduced peripheral nociceptive input or decreased central sensitivity [72, 73]. In terms of improving physical function. researchers found that SSNB significantly improved disability scores in the treatment of chronic shoulder pain compared to placebo [72, 74, 75]. However, our study yielded an opposite result, possibly due to limited evidence from only one included study in the NMA. Thus, more studies are strongly required to confirm the efficacy of SSNB + CPT in improving physical function compared to CPT alone.
Compared to CPT alone, CSI + CPT significantly improved the SPADI total score in patients with chronic shoulder pain, but showed no difference in pain intensity or shoulder mobility. A prior study found that subacromial injection of betamethasone and xylocaine was no more effective than xylocaine alone in improving shoulder mobility or alleviating impingement signs in patients with chronic rotator cuff tendinosis, which was consistent with our finding [76]. More recently, a meta-analysis indicated that CSI provide only small and transient pain relief for a limited number of patients with rotator cuff tendinopathy, and do not alter the natural progression of the disease [77]. A systematic review reported that a single CSI in conjunction with home exercise may be beneficial for patients with frozen shoulder lasting less than 6 months [78]. Therefore, there is currently no conclusive evidence supporting the effectiveness of CSI in managing chronic shoulder pain. Given the potential side effects of CSI, such as the risk of tendon damage with repeated use, caution should be taken when combining with physical therapy [79].
In our NMA, we found that compared to CPT alone, HAI + CPT had no significant effect on improving pain intensity, physical function, or shoulder mobility in patients with chronic shoulder pain. HA, a non-sulfated glycosaminoglycan, is thought to protect tissues from environmental damage and to promote regeneration and repair in articular cartilage, synovial tissue, and synovial fluid [80]. A multicenter RCT found no significant difference between HAI and phosphate-buffered saline in treating chronic shoulder pain related to glenohumeral osteoarthritis, which was consistent with our finding [81]. Similarly, in the management of chronic subacromial bursitis, a previous study also found no difference between the HAI group and the saline group in improving SPADI scores [82]. However, Blaine et al. found that HAI was both effective and well-tolerated in treating persistent shoulder pain that was unresponsive to other standard nonoperative interventions [83]. Jiménez et al. indicated that subacromial HAI was notably effective for patients with reduced subacromial space or cuff tears, but showed limited effectiveness in those with acromioclavicular osteoarthritis [84]. The evidence regarding the effectiveness of HAI for chronic shoulder pain is contradictory, highlighting the need for high-quality basic science studies and RCTs to better assess its efficacy.
Our analysis showed that for patients receiving CPT treatment, the combination of KT did not yield additional benefits in improving shoulder mobility. KT, an elastic therapeutic tape, is widely used for a variety of musculoskeletal disorders. Some researchers believed that KT could increase the non-noxious stimulus through the skin, thereby lessening the input of painful stimulus induced by complex pathogenic factors. KT is also considered to elevate fascia and soft tissues, creating additional space and reducing localized pressure, ultimately improving circulation and lymphatic drainage [35]. However, two prior systematic reviews indicated that current evidence does not recommend the application of KT in clinical practice [35, 85]. Likewise, a recent meta-analysis also suggested that KT for rotator cuff disease has uncertain efficacy in improving active ROM when compared to sham taping [86]. These evidence all aligned with our findings.
To the best of our knowledge, this is the first study to evaluate the therapeutic effects of five analgesic strategies combined with CPT for patients with chronic shoulder pain. As chronic shoulder pain requires multidisciplinary management, comparing these combined approaches is more in line with clinical practice. We performed a comprehensive ranking of ESWT + CPT, SSNB + CPT, CSI + CPT, HAI + CPT, and KT + CPT to identify the best combined approaches for improving pain intensity, physical function, and shoulder mobility in patients with chronic shoulder pain. There were still several limitations in this study. Firstly, our study aims to compare interventions from a broad perspective, thus omitting detailed specific interventions such as CPT. Likewise, several factors such as injection site, injection dose, energy levels, and intervention durations are also ignored, possibly inducing some bias. Secondly, the methodological quality of these included studies is not high. Pain and functional improvement, as subjective indicators, may introduce bias in the results. Thirdly, we included only English-language papers, possibly leading to linguistic bias. Finally, the findings should be interpreted cautiously due to the limited number of clinical trials for head-to-head comparisons between these interventions.
Conclusion
Overall, in managing chronic shoulder pain, ESWT + CPT was the most effective intervention for reducing pain intensity and improving physical function. SSNB + CPT was optimal for enhancing shoulder mobility. Compared to CPT alone, CSI + CPT only significantly improved the SPADI total score, but showed no difference in pain intensity or shoulder mobility. HAI + CPT had no significant difference in improving pain intensity, physical function, or shoulder mobility compared to CPT alone. Adding KT to CPT did not yield additional benefits in improving shoulder mobility. Due to the existing limitations of this study, our findings should be interpreted cautiously. Future clinical trials with larger sample sizes and higher methodological rigor are strongly required to confirm the current results.
Data availability
No datasets were generated or analysed during the current study.
References
Greving K, Dorrestijn O, Winters JC, Groenhof F, van der Meer K, Stevens M, et al. Incidence, prevalence, and consultation rates of shoulder complaints in general practice. Scand J Rheumatol. 2012;41(2):150–5. https://doi.org/10.3109/03009742.2011.605390.
Luime JJ, Koes BW, Hendriksen IJ, Burdorf A, Verhagen AP, Miedema HS, et al. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand J Rheumatol. 2004;33(2):73–81. https://doi.org/10.1080/03009740310004667.
Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP classification of Chronic Pain for the International classification of diseases (ICD-11). Pain. 2019;160(1):19–27. https://doi.org/10.1097/j.pain.0000000000001384.
Diercks R, Bron C, Dorrestijn O, Meskers C, Naber R, de Ruiter T, et al. Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop. 2014;85(3):314–22. https://doi.org/10.3109/17453674.2014.920991.
Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009;43(6):409–16. https://doi.org/10.1136/bjsm.2008.051193.
Hill JR, Olson JJ, Sefko JA, Steger-May K, Teefey SA, Middleton WD et al. Does Surgical intervention alter the natural history of degenerative rotator cuff tears? Comparative analysis from a prospective longitudinal study. Journal of shoulder and elbow surgery 2024;S1058-2746(24):00509–3. https://doi.org/10.1016/j.jse.2024.05.056
Berner JE, Nicolaides M, Ali S, Pafitanis G, Preece J, Hopewell S, et al. Pharmacological interventions for early-stage frozen shoulder: a systematic review and network meta-analysis. Rheumatology (Oxford). 2024;keae176. https://doi.org/10.1093/rheumatology/keae176.
Dias D, Neto MG, Sales SDSR, Cavalcante BDS, Torrierri P Jr, Roever L, et al. Effect of mobilization with Movement on Pain, disability, and Range of Motion in patients with Shoulder Pain and Movement Impairment: a systematic review and Meta-analysis. J Clin Med. 2023;12(23):7416. https://doi.org/10.3390/jcm12237416.
Walker J. Shoulder pain: pathogenesis, diagnosis and management. Nurs Stand. 2014;28(22):51–60. https://doi.org/10.7748/ns2014.01.28.22.51.e8145.
Schwerla F, Hinse T, Klosterkamp M, Schmitt T, Rütz M, Resch KL. Osteopathic treatment of patients with shoulder pain. A pragmatic randomized controlled trial. J Bodyw Mov Ther. 2020;24(3):21–8. https://doi.org/10.1016/j.jbmt.2020.02.009.
Gismervik SØ, Drogset JO, Granviken F, Rø M, Leivseth G. Physical examination tests of the shoulder: a systematic review and meta-analysis of diagnostic test performance. BMC Musculoskelet Disord. 2017;18(1):41. https://doi.org/10.1186/s12891-017-1400-0.
Hanchard NC, Lenza M, Handoll HH, Takwoingi Y. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. Cochrane Database Syst Rev. 2013;2013(4):CD007427. https://doi.org/10.1002/14651858.cd007427.pub2.
Peek AL, Miller C, Heneghan NR. Thoracic manual therapy in the management of non-specific shoulder pain: a systematic review. J Man Manip Ther. 2015;23(4):176–87. https://doi.org/10.1179/2042618615y.0000000003.
Schellingerhout JM, Verhagen AP, Thomas S, Koes BW. Lack of uniformity in diagnostic labeling of shoulder pain: time for a different approach. Man Ther. 2008;13(6):478–83. https://doi.org/10.1016/j.math.2008.04.005.
Silveira A, Lima C, Beaupre L, Chepeha J, Jones A. Shoulder specific exercise therapy is effective in reducing chronic shoulder pain: a network meta-analysis. PLoS ONE. 2024;19(4):e0294014. https://doi.org/10.1371/journal.pone.0294014.
Smith N, Liew Z, Johnson S, Ellard DR, Underwood M, Kearney R. A systematic review of the methods and drugs used for performing suprascapular nerve block injections for the non-surgical management of chronic shoulder pain. Br J Pain. 2021;15(4):460–73. https://doi.org/10.1177/2049463721992091.
Chang KV, Hung CY, Wu WT, Han DS, Yang RS, Lin CP. Comparison of the effectiveness of suprascapular nerve Block with Physical Therapy, Placebo, and Intra-articular Injection in Management of Chronic Shoulder Pain: a Meta-analysis of Randomized controlled trials. Arch Phys Med Rehabil. 2016;97(8):1366–80. https://doi.org/10.1016/j.apmr.2015.11.009.
Jurak I, Delaš K, Erjavec L, Stare J, Locatelli I. Effects of Multidisciplinary Biopsychosocial Rehabilitation on Short-Term Pain and Disability in Chronic Low Back Pain: a systematic review with Network Meta-Analysis. J Clin Med. 2023;12(23):7489. https://doi.org/10.3390/jcm12237489.
Ejnisman B, Andreoli CV, Soares BG, et al. Interventions for tears of the rotator cuff in adults. Cochrane Database Syst Rev. 2004;1CD002758. https://doi.org/10.1002/14651858.pub2.
Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. Chronic shoulder pain: part II. Treat Am Fam Physician. 2008;77(4):493–7.
Haik MN, Alburquerque-Sendín F, Moreira RF, Pires ED, Camargo PR. Effectiveness of physical therapy treatment of clearly defined subacromial pain: a systematic review of randomised controlled trials. Br J Sports Med. 2016;50(18):1124–34. https://doi.org/10.1136/bjsports-2015-095771.
McDevitt AW, Young JL, Cleland JA, Hiefield P, Snodgrass SJ. Physical therapy interventions used to treat individuals with biceps tendinopathy: a scoping review. Braz J Phys Ther. 2024;28(1):100586. https://doi.org/10.1016/j.bjpt.2023.100586.
Marinko LN, Chacko JM, Dalton D, Chacko CC. The effectiveness of therapeutic exercise for painful shoulder conditions: a meta-analysis. J Shoulder Elb Surg. 2011;20(8):135–9. https://doi.org/10.1016/j.jse.2011.05.013.
Pieters L, Lewis J, Kuppens K, Jochems J, Bruijstens T, Joossens L, et al. An update of systematic reviews examining the effectiveness of conservative physical therapy interventions for subacromial shoulder pain. J Orthop Sports Phys Ther. 2020;50(3):131–41. https://doi.org/10.2519/jospt.2020.8498.
Zhong Z, Zang W, Tang Z, Pan Q, Yang Z, Chen B. Effect of scapular stabilization exercises on subacromial pain (impingement) syndrome: a systematic review and meta-analysis of randomized controlled trials. Front Neurol. 2024;15:1357763. https://doi.org/10.3389/fneur.2024.1357763.
Holmgren T, Hallgren HB, Oberg B, Adolfsson L, Johansson K. Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: randomised controlled study. Br J Sports Med. 2014;48(19):1456–7. https://doi.org/10.1136/bjsports-2014-e787rep.
Lähdeoja T, Karjalainen T, Jokihaara J, Salamh P, Kavaja L, Agarwal A, et al. Subacromial decompression surgery for adults with shoulder pain: a systematic review with meta-analysis. Br J Sports Med. 2020;54(11):665–73. https://doi.org/10.1136/bjsports-2018-100486.
Kukkonen J, Joukainen A, Lehtinen J, Mattila KT, Tuominen EK, Kauko T et al. Treatment of Nontraumatic Rotator Cuff Tears: A Randomized Controlled Trial with Two Years of Clinical and Imaging Follow-up published correction appears in J Bone Joint Surg Am. 2016;98(1):e1. J Bone Joint Surg Am 2015;97(21):1729–1737. https://doi.org/10.2106/JBJS.N.01051
Smith BE, Hendrick P, Smith TO, Bateman M, Moffatt F, Rathleff MS, et al. Should exercises be painful in the management of chronic musculoskeletal pain? A systematic review and meta-analysis. Br J Sports Med. 2017;51(23):1679–87. https://doi.org/10.1136/bjsports-2016-097383.
Saltychev M, Äärimaa V, Virolainen P, Laimi K. Conservative treatment or surgery for shoulder impingement: systematic review and meta-analysis. Disabil Rehabil. 2015;37(1):1–8. https://doi.org/10.3109/09638288.2014.907364.
Huang YC, Leong CP, Tso HH, Chen MJ, Liaw MY, Hsieh HC, et al. The long-term effects of hyaluronic acid on hemiplegic shoulder pain and injury in stroke patients: a randomized controlled study. Medicine. vol 2018;97(35):e12078. https://doi.org/10.1097/MD.0000000000012078.
Dahan TH, Fortin L, Pelletier M, Petit M, Vadeboncoeur R, Suissa S. Double blind randomized clinical trial examining the efficacy of bupivacaine suprascapular nerve blocks in frozen shoulder. J Rheumatol. 2000;27(6):1464–9.
Rezasoltani Z, Esmaily H, Dadarkhah A, Rousta M, Mohebbi R, Vashaei F. Low molecular-weight Hyaluronic Acid Versus Physiotherapy for the treatment of Supraspinatus Tendinopathy: a randomized comparative clinical trial. J Am Acad Orthop Surg. 2021;29(19):e979–92. https://doi.org/10.5435/JAAOS-D-20-01014.
Liao CD, Xie GM, Tsauo JY, Chen HC, Liou TH. Efficacy of extracorporeal shock wave therapy for knee tendinopathies and other soft tissue disorders: a meta-analysis of randomized controlled trials. BMC Musculoskelet Disord. 2018;19(1):278. https://doi.org/10.1186/s12891-018-2204-6.
Williams S, Whatman C, Hume PA, Sheerin K. Kinesio taping in treatment and prevention of sports injuries: a meta-analysis of the evidence for its effectiveness. Sports Med. 2012;42(2):153–64. https://doi.org/10.2165/11594960-000000000-00000.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. https://doi.org/10.1136/bmj.n160.
White IR. Network meta-analysis. STATA J. 2015;15(4):951–85. https://doi.org/10.1177/1536867X1501500403.
Chaimani A, Salanti G. Visualizing assumptions and results in network metaanalysis: the network graphs package. STATA J. 2015;15(4):905–50. https://doi.org/10.1177/1536867X1501500402.
Shim SR, Kim SJ. Intervention meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019008. https://doi.org/10.4178/epih.e2019008.
Higgins JP, Jackson D, Barrett JK, Lu G, Ades AE, White IR. Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res Synth Methods. 2012;3(2):98–110. https://doi.org/10.1002/jrsm.1044.
Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS ONE. 2013;8(10):e76654. https://doi.org/10.1371/journal.pone.007665.
Abdelshafi ME, Yosry M, Elmulla AF, Al-Shahawy EA, Adou Aly M, Eliewa EA. Relief of chronic shoulder pain: a comparative study of three approaches. Middle East J Anaesthesiol. 2011;21(1):83–92.
Hsieh LF, Hsu WC, Lin YJ, Chang HL, Chen CC, Huang V. Addition of intra-articular hyaluronate injection to physical therapy program produces no extra benefits in patients with adhesive capsulitis of the shoulder: a randomized controlled trial. Arch Phys Med Rehabil. 2012;93(6):957–64. https://doi.org/10.1016/j.apmr.2012.01.021.
Maryam M, Zahra K, Adeleh B, Morteza Y. Comparison of corticosteroid injections, physiotherapy, and combination therapy in treatment of frozen shoulder. Pak J Med Sci. 2012;28(4):648–51.
Di Giacomo G, De Gasperis N. The role of hyaluronic acid in patients affected by glenohumeral osteoarthritis. J Biol Regul Homeost Agents. 2015;29(4):945–51.
Di Giacomo G, de Gasperis N. Hyaluronic Acid Intra-articular injections in patients affected by moderate to severe glenohumeral osteoarthritis: a prospective Randomized Study. Joints. 2017;5(3):138–42. https://doi.org/10.1055/s-0037-1605389.
Duymaz T, Sindel D. Comparison of Radial extracorporeal shock Wave Therapy and Traditional Physiotherapy in Rotator Cuff Calcific Tendinitis Treatment. Arch Rheumatol. 2019;34(3):281–7. https://doi.org/10.5606/ArchRheumatol.2019.7081.
de Oliveira FCL, Pairot de Fontenay B, Bouyer LJ, Desmeules F, Roy JS. Kinesiotaping for the Rehabilitation of Rotator Cuff-Related Shoulder Pain: a Randomized Clinical Trial. Sports Health. 2021;13(2):161–72. https://doi.org/10.1177/1941738120944254.
Di Giacomo G, de Gasperis N. Glenohumeral osteoarthritis treatment with a single hyaluronic acid administration: clinical outcomes. J Biol Regul Homeost Agents. 2021;35(2):657–61. https://doi.org/10.23812/20-457-L.
Yehia RM, ElMeligie MM. Effectiveness of extracorporeal shockwave therapy for frozen shoulder in perimenopausal diabetic women. Biomed Hum Kinet. 2022;14(1):109–16. https://doi.org/10.2478/bhk-2022-0014.
Mardani-Kivi M, Nabi BN, Mousavi MH, Shirangi A, Leili EK, Ghadim-Limudahi ZH. Role of suprascapular nerve block in idiopathic frozen shoulder treatment: a clinical trial survey. Clin Shoulder Elb. 2022;25(2):129–39. https://doi.org/10.5397/cise.2021.00661.
ElGendy MH, Mazen MM, Saied AM, ElMeligie MM, Aneis Y. Extracorporeal shock Wave Therapy vs. Corticosteroid Local Injection in Shoulder Impingement Syndrome: A Three-Arm Randomized Controlled Trial. Am J Phys Med Rehabil. 2023;102(6):533–40. https://doi.org/10.1097/PHM.0000000000002158.
Hsieh LF, Kuo YC, Huang YH, Liu YF, Hsieh TL. Comparison of corticosteroid injection, physiotherapy and combined treatment for patients with chronic subacromial bursitis - A randomised controlled trial. Clin Rehabil. 2023;37(9):1189–200. https://doi.org/10.1177/02692155231166220.
Khalifa HA, Darwish MH, El-Tamawy MS, Elazizy HM, Abu Ella IA, Abo-Zaid NA, et al. The influence of radial extracorporeal shock wave therapy on shoulder pain and structural abnormalities in stroke patients. Arch Med Sci. 2022;19(6):1731–8. https://doi.org/10.5114/aoms/151477.
Wu SY, Hsu PC, Tsai YY, Huang JR, Wang KA, Wang JC. Efficacy of combined ultrasound-guided hydrodilatation with hyaluronic acid and physical therapy in patients with adhesive capsulitis: a randomised controlled trial. Clin Rehabil. 2024;38(2):202–15. https://doi.org/10.1177/02692155231200089.
Kamel SI, Rosas HG, Gorbachova T. Local and systemic side effects of Corticosteroid injections for Musculoskeletal indications. AJR Am J Roentgenol. 2024;222(3):e2330458. https://doi.org/10.2214/AJR.23.30458.
Ogden JA, Alvarez RG, Levitt R, Marlow M. Shock wave therapy (Orthotripsy) in musculoskeletal disorders. Clin Orthop Relat Res. 2001;387:22–40. https://doi.org/10.1097/00003086-200106000-00005.
Moya D, Ramón S, Schaden W, Wang CJ, Guiloff L, Cheng JH. The role of extracorporeal Shockwave Treatment in Musculoskeletal disorders. J Bone Joint Surg Am 2018(3);100:251–63. https://doi.org/10.2106/JBJS.17.00661
Chester R, Shepstone L, Daniell H, Sweeting D, Lewis J, Jerosch-Herold C. Predicting response to physiotherapy treatment for musculoskeletal shoulder pain: a systematic review. BMC Musculoskelet Disord. 2013;14:203. https://doi.org/10.1186/1471-2474-14-203.
Struyf F, Meeus M. Current evidence on physical therapy in patients with adhesive capsulitis: what are we missing? Clin Rheumatol. 2014;33(5):593–600. https://doi.org/10.1007/s10067-013-2464-3.
Bury J, Littlewood C. Rotator cuff disorders: a survey of current (2016) UK physiotherapy practice. Shoulder Elb. 2018;10(1):52–61. https://doi.org/10.1177/1758573217717103.
Struyf F, De Hertogh W, Gulinck J, Nijs J. Evidence-based treatment methods for the management of shoulder impingement syndrome among dutch-speaking physiotherapists: an online, web-based survey. J Manipulative Physiol Ther. 2012;35(9):720–6. https://doi.org/10.1016/j.jmpt.2012.10.009.
Mao HY, Hu MT, Yen YY, Lan SJ, Lee SD. Kinesio Taping relieves Pain and improves isokinetic not isometric muscle strength in patients with knee Osteoarthritis-A systematic review and Meta-analysis. Int J Environ Res Public Health. 2021;18(19):10440. https://doi.org/10.3390/ijerph181910440.
Raeesi J, Negahban H, Kachooei AR, Moradi A, Ebrahimzadeh MH, Daghiani M. Comparing the effect of physiotherapy and physiotherapy plus corticosteroid injection on pain intensity, disability, quality of life, and treatment effectiveness in patients with Subacromial Pain Syndrome: a randomized controlled trial. Disabil Rehabil. 2023;45(25):4218–26. https://doi.org/10.1080/09638288.2022.2146215.
Saggini R, Di Stefano A, Saggini A, Bellomo RG. CLINICAL APPLICATION OF SHOCK WAVE THERAPY IN MUSCULOSKELETAL DISORDERS: PART I. J Biol Regul Homeost Agents. 2015;29(3):533–45.
Simplicio CL, Purita J, Murrell W, Santos GS, Dos Santos RG, Lana JFSD. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J Clin Orthop Trauma. 2020;11:S309–18. https://doi.org/10.1016/j.jcot.2020.02.004.
Shao H, Zhang S, Chen J, Wen A, Wu Z, Huang M, et al. Radial extracorporeal shockwave therapy reduces pain and promotes proximal tendon healing after rotator cuff repair: randomized clinical trial. Ann Phys Rehabil Med. 2023;66(4):101730. https://doi.org/10.1016/j.rehab.2023.101730.
Martens G, Fontaine R, Goffin P, Raaf M, Tasset H, Lecoq JP, et al. Continuous suprascapular nerve blockade to potentiate intensive rehabilitation for refractory adhesive shoulder capsulitis: a cohort study. Int Orthop. 2024;48(2):495–503. https://doi.org/10.1007/s00264-023-05999-0.
Parashar A, Goni V, Neradi D, Guled U, Rangasamy K, Batra YK. Comparing three modalities of treatment for frozen shoulder: a prospective, Double-Blinded, Randomized Control Trial. Indian J Orthop. 2020;55(2):449–56. https://doi.org/10.1007/s43465-020-00201-8.
Hou Y, Wang Y, Sun X, Lou Y, Yu Y, Zhang T. Effectiveness of suprascapular nerve block in the treatment of Hemiplegic Shoulder Pain: a systematic review and Meta-analysis. Front Neurol. 2021;12:723664. https://doi.org/10.3389/fneur.2021.723664.
Sun C, Ji X, Zhang X, Ma Q, Yu P, Cai X, et al. Suprascapular nerve block is a clinically attractive alternative to interscalene nerve block during arthroscopic shoulder surgery: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2021;16(1):376. https://doi.org/10.1186/s13018-021-02515-1.
Shanahan EM, Ahern M, Smith M, Wetherall M, Bresnihan B, FitzGerald O. Suprascapular nerve block (using bupivacaine and methylprednisolone acetate) in chronic shoulder pain. Ann Rheum Dis. 2003;62(5):400–6. https://doi.org/10.1136/ard.62.5.400.
Klç Z, Filiz MB, Çakr T, Toraman NF. Addition of suprascapular nerve block to a physical therapy program produces an Extra Benefit to Adhesive Capsulitis: a Randomized Controlled Trial. Am J Phys Med Rehabil. 2015;94:912–20. https://doi.org/10.1097/PHM.0000000000000336.
Shanahan EM, Gill TK, Briggs E, Hill CL, Bain G, Morris T. Suprascapular nerve block for the treatment of adhesive capsulitis: a randomised double-blind placebo-controlled trial. RMD Open. 2022;8(2):e002648. https://doi.org/10.1136/rmdopen-2022-002648.
Shanahan EM, Smith MD, Wetherall M, Lott CW, Slavotinek J, FitzGerald O, et al. Suprascapular nerve block in chronic shoulder pain: are the radiologists better? Ann Rheum Dis. 2004;63(9):1035–40. https://doi.org/10.1136/ard.2003.015909.
Alvarez CM, Litchfield R, Jackowski D, Griffin S, Kirkley A. A prospective, double-blind, randomized clinical trial comparing subacromial injection of betamethasone and xylocaine to xylocaine alone in chronic rotator cuff tendinosis. Am J Sports Med. 2005;33(2):255–62. https://doi.org/10.1177/0363546504267345.
Mohamadi A, Chan JJ, Claessen FM, Ring D, Chen NC. Corticosteroid injections give small and transient Pain Relief in Rotator Cuff Tendinosis: a Meta-analysis. Clin Orthop Relat Res. 2017;475(1):232–43. https://doi.org/10.1007/s11999-016-5002-1.
Maund E, Craig D, Suekarran S, Neilson A, Wright K, Brealey S, et al. Management of frozen shoulder: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2012;16(11):1–264. https://doi.org/10.3310/hta16110.
Dean BJ, Franklin SL, Murphy RJ, Javaid MK, Carr AJ. Glucocorticoids induce specific ion-channel-mediated toxicity in human rotator cuff tendon: a mechanism underpinning the ultimately deleterious effect of steroid injection in tendinopathy? Br J Sports Med. 2014;48(22):1620–6. https://doi.org/10.1136/bjsports-2013-093178.
Liang J, Jiang D, Noble PW. Hyaluronan as a therapeutic target in human diseases. Adv Drug Deliv Rev. 2016;97:186–203. https://doi.org/10.1016/j.addr.2015.10.017.
Kwon YW, Eisenberg G, Zuckerman JD. Sodium hyaluronate for the treatment of chronic shoulder pain associated with glenohumeral osteoarthritis: a multicenter, randomized, double-blind, placebo-controlled trial. J Shoulder Elb Surg. 2013;22(5):584–94. https://doi.org/10.1016/j.jse.2012.10.040.
Hsieh LF, Lin YJ, Hsu WC, Kuo YC, Liu YC, Chiang YP, et al. Comparison of the corticosteroid injection and hyaluronate in the treatment of chronic subacromial bursitis: a randomized controlled trial. Clin Rehabil. 2021;35(9):1305–16. https://doi.org/10.1177/02692155211007799.
Blaine T, Moskowitz R, Udell J, Skyhar M, Levin R, et al. Treatment of persistent shoulder pain with sodium hyaluronate: a randomized, controlled trial. A multicenter study. J Bone Joint Surg Am. 2008;90(5):970–9. https://doi.org/10.2106/jbjs.f.01116.
Jiménez I, Marcos-García A, Muratore-Moreno G, Romero-Pérez B, Álvarez-León EE, Medina J. [Subacromial sodium hyaluronate injection for the treatment of chronic shoulder pain: a prospective series of eighty patients]. Acta Ortop Mex. 2018;32(2):70–5.
Parreira Pdo C, Costa Lda C, Hespanhol LC Jr, Lopes AD, Costa LO. Current evidence does not support the use of Kinesio Taping in clinical practice: a systematic review. J Physiother. 2014;60(1):31–9. https://doi.org/10.1016/j.jphys.2013.12.008.
Gianola S, Iannicelli V, Fascio E, Andreano A, Li LC, Valsecchi MG, et al. Kinesio taping for rotator cuff disease. Cochrane Database Syst Rev. 2021;8(8):CD012720. https://doi.org/10.1002/14651858.CD012720.pub2.
Acknowledgements
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Henan Province Science and Technology Research Project [grant number 242300420107], 2023 Henan Special Research Project of TCM on “Double First-Class” Construction [grant number HSRP-DFCTCM-2023-1-21], Henan Province Science and Technology Research Project [grant number 232102310466], and Campus-level project of Henan University of Chinese Medicine [grant number 2024JX62].
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception. Yasu Zhang and Qian Gao designed the search strategies. Fangjie Yang and Mengyang Pan screened eligible studies. Xinmin Li and Jing Wang collected and summarized the data. Fangjie Yang, Zhenfei Duan, Chunlin Ren, and Pengxue Guo analyzed the data. Fangjie Yang and Xinmin Li wrote initial draft of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical Approval and Consent to participate are not applicable. The study protocol was registered at PROSPERO (CRD 42024519473).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, F., Li, X., Wang, J. et al. Efficacy of different analgesic strategies combined with conventional physiotherapy program for treating chronic shoulder pain: a systematic review and network meta-analysis. J Orthop Surg Res 19, 544 (2024). https://doi.org/10.1186/s13018-024-05037-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-05037-8