
Abstract
Non-protein target drugs, especially RNA-based gene therapies for treating hereditary diseases, have been recognized worldwide. As cancer is an insurmountable challenge, no miracle drug is currently available. With the advancements in the field of biopharmaceuticals, research on cancer therapy has gradually focused on non-protein target-targeted drugs, especially RNA therapeutics, including oligonucleotide drugs and mRNA vaccines. This review mainly summarizes the clinical research progress in RNA therapeutics and highlights that appropriate target selection and optimized delivery vehicles are key factors in increasing the effectiveness of cancer treatment in vivo.
Similar content being viewed by others


Introduction
Cancer treatment remains a challenge worldwide. Although overall survival is improved by surgical removal of tumor tissues, chemotherapy, and radiotherapy, recurrence and metastasis of cancers cannot be avoided [1]. Moreover, chemotherapy has serious adverse effects, such as systemic toxicity and multiple drug resistance, which require the development of novel and effective therapeutic drugs [2].
Small molecule agents and antibodies that can target intracellular or extracellular proteins in tumor cells have become increasingly popular because of their strong antitumor effects [3, 4]. However, they fail to block some transcription factors and oncoproteins, such as RAS [5], one of the most frequently mutated proteins in cancer. Therefore, non-protein-targeted drugs have emerged to address this dilemma. In particular, RNA-based drugs, which are important components of gene therapy, are the most notable and serve as potential therapeutics that can specifically target and silence any gene target [6]. The molecular weight of therapeutic RNAs is generally 7–20 kDa, which is much greater than that of small-molecule drugs (< 1 kDa) but less than that of antibodies (> 100 kDa). Full-length mRNA vaccines are also large (> 100 kDa) [7].
Owing to the development of and improvements in RNA technology, certain synthesized oligonucleotide drugs and macromolecular RNA drugs, such as antisense oligonucleotides (ASOs), small-interfering RNAs (siRNAs), and mRNA vaccines (Table 1), have been approved for marketing worldwide [8]. Additionally, an increasing number of oligonucleotide drugs (such as ASOs, siRNAs, and miRNAs) and mRNA drugs are entering clinical trials worldwide [9].
RNA-based drugs have played a important role in various diseases, ranging from genetic diseases to viral infections, and clinical studies on RNA-based therapeutics have yielded satisfactory results. Therefore, RNA molecules under development are potential candidates and powerful tools for cancer treatment [10]. This paper summarizes the research progress of the non-protein target drugs, mainly RNA-based drugs in cancer treatment in recent years, including oligonucleotide drugs (ASOs, siRNA, microRNA), and mRNA vaccines, and puts forward suggestions on the challenges brought by this class of new drugs, and fully exerts their therapeutic potential.
This paper summarizes the recent research progress on non-protein-targeted drugs, mainly RNA-based drugs, including oligonucleotide drugs (ASOs, siRNA, and microRNA) and mRNA vaccines, in cancer treatment and enumerates the current challenges faced by researchers studying this new class of drugs.
Oligonucleotide therapeutics
Approximately 40 years ago, Paul Zamecnik and Mary Stephenson successfully used synthetic oligonucleotides to block the translation of viral RNA [11]. Currently, owing to the benefits of Watson–Crick base-pairing rules and maturation of RNA technologies, oligonucleotides can be used to treat diseases by binding to specific DNA or RNA sequences or proteins and interfering with target gene expression.
Oligonucleotide therapeutics are drugs consisting of 10–50 nucleotides in length, including ASOs, siRNAs, and microRNAs (miRNAs), and can regulate the post-transcriptional level and are expected to target special proteins that are otherwise difficult to target directly [12]. Hence, oligonucleotide therapeutics are considered the third pillar of drug development, after small-molecule drugs and antibodies [13]. Drug constructs based on the genomic sequences of target genes are simple to design, and drug candidates only require the identification of the target regions in the RNA associated with the disease process. The key is to design sequences that are highly specific to the target RNA and avoid hybridization with unexpected but homologous “bystander” RNAs. ASOs, siRNAs, and miRNAs are currently the most extensively studied drugs for treating malignant tumors. Here, we provide an overview of recent clinical research progress.
Antisense oligonucleotide (ASO)
In 1978, Zamecnik and Stephenson used a 13-nucleotide ASO targeting the sequence of the Rous sarcoma virus to inhibit viral replication in vitro. This was the first study to report the therapeutic application of ASOs [11]. Subsequently, some commercial companies have focused on antisense therapeutics; thus, progress on oligonucleotide chemistry and formulations and the distribution and safety of ASOs have achieved satisfactory results (Table 2).
ASOs are chemically synthesized oligonucleotides, typically 1–30 nucleotides in length, that bind to RNA following Watson–Crick base-pairing rules. The length of the ASOs allows them to bind uniquely to only one target RNA. Although the first two marketed ASO medications, Fomivirsen and Mipomersen [14], have been discontinued, there are still seven approved ASO drugs for medical use in the market [15, 16], mainly for treating diseases, such as Duchenne muscular dystrophy (DMD) [17], spinal muscular atrophy, familial amyloid polyneuropathy [18, 19], and familial chylomicronemia syndrome.
Proteins of the B-cell lymphoma 2 (Bcl-2) family play a role in the regulation of apoptosis and confer resistance to traditional cytotoxic chemotherapy and monoclonal antibodies, making Bcl-2 an attractive target for therapeutic intervention in cancers. Oblimersen sodium (Genasense™, G3139) is an antisense oligonucleotide that hybridizes to the first six codons of the open reading frame of the Bcl-2 mRNA, resulting in Bcl-2 mRNA degradation and induction of apoptosis [20]. There have been many clinical trials on oblimersen, combined with chemotherapy drugs, such as carboplatin [21, 22], paclitaxel [23], docetaxel [24,25,26,27], and irinotecan [28], for treating solid tumors. In a phase I/II trial, the combination of oblimersen and the prodrug irinotecan was well tolerated in patients with metastatic colorectal cancer; one patient experienced a partial response, and another 10 patients had stable disease lasting for 2.5–10 months (NCT00004870) [28]. Safety data from clinical trials further support the clinical development of oblimersen in combination with cytotoxic agents.
BP1001 is a liposome-incorporated antisense oligodeoxynucleotide designed to inhibit the expression of growth factor receptor-bound protein-2 (Grb-2), an essential oncoprotein in cancer cell signaling [29]. In a phase I clinical study (NCT01159028), BP1001 was well tolerated both as monotherapy and in combination with low-dose ara-C (LDAC) [30].
As a therapeutic target, clusterin is overexpressed in many cancers, inhibiting cell death pathways and modulating pro-survival and transcriptional networks [31]. OGX-011 (custirsen) is a second-generation antisense clusterin inhibitor. To determine the clinical activity of OGX-011, a randomized phase II study, in combination with docetaxel/prednisone, was conducted in patients with metastatic castration-resistant prostate cancer. Treatment with OGX-011 and docetaxel was well tolerated and associated with improved survival, as OGX-011 enhanced the tumor-killing ability of docetaxel by increasing the sensitivity of tumor cells to the drug [32]. OGX-011 may also be a new treatment strategy for patients with castration-resistant prostate cancer (CRPC) [33].
Heat shock protein 27 (Hsp27) is a stress-induced multifunctional chaperone that promotes cancer development through its proliferative and antiapoptotic functions. Hsp27 causes therapeutic resistance in prostate and other cancers, and its targeted inhibition sensitizes cancer cells to hormones and chemotherapy. OGX-427 (Apatoren) is a 2′-methoxyethyl-modified ASO that inhibits Hsp27 expression. Hsp27 participates in endoplasmic reticulum (ER) homeostasis, and the knockdown of Hsp27 using OGX-427 induces ER stress [34]. In a phase I clinical trial, the safety profile of OGX-427 in patients with advanced cancer showed that OGX-427 was tolerated at the highest dose (1000 mg) (NCT00487786) [35].
The signal transduction and transcriptional activator 3 (STAT3) is an attractive target for many cancers. However, translating the utility of its inhibition from bench to bedside is challenging. AZD9150 (Danvatirsen, ISIS 481464), a generation 2.5 ASO, is a specific inhibitor of STAT3. Compared with generation 2.0 and previous ASOs, generation 2.5 ASOs have a higher affinity and greater intrinsic potency owing to an 8′–10′ phosphorothioate-modified deoxynucleotide “gap” flanked on either end, with 2–3 cEt nucleotides [36]. AZD9150 specifically inhibits STAT3 and induces apoptosis in various leukemia cell lines [37]. AZD9150 showed a good efficacy and safety profile in patients with heavily pretreated lymphoma and solid tumors who have undergone extensive pretreatment [38]. AZD9150 also decreased tumorigenicity and increased the chemosensitivity of neuroblastoma cells by inhibiting endogenous STAT3 and STAT3 target genes [39]. The STAT3 transcription network is an important driver of the suppressive tumor microenvironment, thus preventing checkpoint-blockade activity. In two phase I clinical studies (NCT01563302 and NCT01839604), AZD9150 monotherapy induced an immune-mediated antitumor response, suggesting that AZD9150, in combination with checkpoint-inhibitor therapy, is expected to enhance antitumor immunity [40].
LErafAON is a novel formulation of liposome-entrapped ASO targeting the Raf proto-oncogene, which encodes a factor known to play a critical role in regulating cancer cell proliferation, survival, and differentiation [41]. The preparation of LErafAON showed high liposome entrapment efficiency and stability at room temperature [42]. A phase I clinical trial evaluating its tolerability and recommended dose, in combination with radiation therapy (NCT00024648), was conducted [43]. Pharmacokinetic analysis revealed the persistence of detectable circulating rafAON at 24 h in 7 of 10 patients in the highest two-dose cohorts. Thus, liposomal formulations may promote better intratumoral AON delivery and inhibit degradation in vivo.
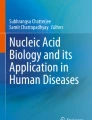
Hypoxia-inducible factor-1 (HIF-1) is a transcription factor that plays key roles in angiogenesis, survival, metastasis, drug resistance, and glucose metabolism. High levels of HIF-1 are associated with poor prognosis and treatment resistance in patients with solid tumors; thus, HIF-1 is an attractive target for cancer therapy. EZN-2968 (also known as RO7070179) is a third-generation ASO that specifically targets HIF-1α, a subunit of HIF-1. EZN-2968 hybridizes with HIF-1α mRNA and blocks HIF-1α protein expression in preclinical models [44]. EZN-2968 was well tolerated at the described dosage and schedule, and most toxicities reported were class 1 or 2, with no accidental toxicity [45] (Fig. 1).

The schematic diagram of antisense oligonucleotides clinically designed for tumor targets, such as Bcl-2, Grb2, CLU, Hsp27, STAT3, c-Raf, HIF-1α, AR, and XIAP (bold font)
Small interfering RNA (siRNA)
Since the discovery of RNA interference (RNAi) and its subsequent application in gene knockdown in mammalian cells, siRNA therapeutics has made remarkable progress and have become promising tools against various diseases [46, 47].
As a type of noncoding double-stranded RNA (dsRNA) molecule, siRNAs are only 18–25 base pairs in length, with or without two overhanging phosphorylated bases at the 3′ end of each strand [48, 49]. As the name suggests, siRNA interferes with the expression of specific genes with complementary nucleotide sequences through mRNA degradation after transcription. Generally, siRNAs can bind to a protein complex called the RNA-induced silencing complex (RISC) in the cytoplasm. Upon binding to RISC, the guide strand is directed to the target mRNA, and the phosphodiester bond at the mRNA nucleotides 10 and 11 paired with the antisense strand is cleaved [50].
To date, four siRNA drugs (patisiran, givosiran, lumasiran, and inclisiran) have been approved for marketing to treat diseases such as TTR, acute hepatic porphyria, primary hyperoxaluria type 1, and hypercholesterolemia [51]. Patisiran [52], an siRNA drug for treating polyneuropathy in adults caused by hereditary transthyretin amyloidosis, was the first United States Food and Drug Administration (FDA)- and European Medicines Agency-approved RNAi-based therapy.siRNA drugs have potential advantages in cancer treatment compared with traditional drugs. First, as a useful therapeutic tool, siRNA can knock down genes that directly or indirectly cause abnormal proliferation of cancer cells. Thus, it is possible to treat gene-based cancers. Second, with extensive siRNA libraries available, targets for selective and specific drug development can be rapidly identified and optimized, and such target identification helps elucidate the role of specific genes in tumorigenesis. Third, the synthesis and manufacturing costs of siRNA drugs are relatively low compared to those of their antibody rivals [53]. Furthermore, optimized siRNA drugs can provide convenient dosing regimens, such as inclisiran, for biannual treatment. These advantages strongly support the notion that siRNA is among the most critical therapeutic tools for the treatment of cancers, and many siRNA drugs have been tested in clinical trials (Table 3).
CALAA-01, a polymer-based nanoparticle containing siRNA targeting the M2 subunit of ribonucleotide reductase (RRM2), was the first experimental RNAi-based drug screened against solid tumors by Calando Pharmaceuticals in 2008 [54]. Phase I clinical trials showed that CALAA-01 was quickly eliminated in the blood after intravenous administration and the clearance is associated with body weight [55].
Another siRNA drug, Atu027, is encapsulated inside a lipid nanoparticle (LNP) to target the protein kinase N3 (PKN3), an essential gene for cancer growth and metastasis [56, 57]. Clinical trial results showed that Atu027 serves a new treatment strategy for solid tumors and has good safety and activity profile in patients with advanced or metastatic pancreatic adenocarcinoma when combined with the standard chemotherapeutic gemcitabine (NCT00938574) [58].
Since the Kirsten rat sarcoma (KRAS) protein binds very closely to nucleotides, which makes it nearly impossible to identify competing nucleotide analogs, the KRAS protein has been considered undruggable for many years. Khvalevsky et al. developed a local prolonged siRNA delivery system, siG12D LODER, against mutated KRAS. This siRNA drug provides an alternative approach for controlling KRAS expression in pancreatic cancer[59]. A phase I study showed the tolerability, safety, and efficacy of siG12D LODE in patients diagnosed with pancreatic cancer and reported no obvious toxicity. Currently, siG12D LODER is undergoing phase II clinical trials [60].
TKM-080301 is an LNP formulation containing the siRNA-targeting polo-like kinase-1 (PLK1) gene. PLK1 is overexpressed in hepatocellular carcinoma (HCC), and inhibition of PLK1 activity can rapidly induce mitotic arrest and apoptosis in cancer cells. TKM-080301 improved the overall survival of patients with advanced HCC [61, 62].
SiRNA-EphA2-DOPC is an siRNA drug encapsulated in neutral 1,2-dioleoyl-sn-glycero-3-phosphatidylcholine (DOPC) liposomes, which targets the ephrin type-A receptor 2 [63]. EphA2 is overexpressed in several cancer cells. Preclinical results revealed that siRNA-EphA2 DOPC had no dose-dependent adverse effects in primates, and phase I clinical trials of siRNA-EphA2 DOPC are currently under recruitment [64].
The MYC oncogene family, which consists of C-MYC, MYCN, and MYCL, whose products regulate the transcription of at least 15% of the entire genome and participate in the growth of many solid tumor malignancies [65]. The siRNA drug DCR-MYC, designed by Dicerna Pharma, is a novel synthetic dsRNA in a stable lipid particle suspension that targets MYC in HCC, solid tumors, and multiple myeloma [66]. Phase I studies showed that DCR-MYC regulates tumor size in patients with solid tumors (NCT02110563).
Glioblastoma (GBM) is one of the most difficult cancers to treat because of the blood–brain and blood-tumor barriers. NU-0129, based on the spherical nucleic acid platform, is an siRNA drug designed to target the GBM oncogene Bcl2Like12 (Bcl2L12), which can cross the blood–brain barrier and may be a new precision medicine approach for GBM treatment. In an early phase I trial, Bcl2L12 protein levels in tumor tissues were reduced after intravenous administration of NU-0129 [67].
MicroRNA (miRNA)
miRNA, a type of small noncoding RNAs encoded by endogenous genes approximately 19–25 nucleotides in size, participates in the regulation of post-transcriptional gene expression [68]. miRNA biogenesis occurs in the nucleus, where gene transcription is strictly regulated. Normally, once miRNAs bind to RISC to form miRISC, the relative gene expression is fine-tuned by blocking translation or cleaving the mRNA via RISC-based mechanisms, similar to those used by siRNA [69]. Thus, RSIC assembly is a key process in performing miRNA functions.
Although siRNA and miRNA are both noncoding RNAs with similar roles in gene silencing and regulation, siRNA is perfectly complementary to a single gene at a specific location, whereas one miRNA has multiple targets and can regulate the expression of hundreds or thousands of genes through imperfect base pairing; a gene can be regulated by several different miRNAs [70]. Thus, the clinical applications and therapeutic potential of these two are different (Fig. 2).

The different regulatory mechanisms of siRNA and miRNA
In 2002, miRNAs were first suggested to participate in cancer progression owing to the deletion and low expression of miR-15 and miR-16 clusters in chronic lymphocytic leukemia [71]. Over the past two decades, the association between miRNAs and various cancers has been extensively studied. miRNAs play a non-negligible role in cancer regulation, and several miRNA-based therapies are underway for different cancers. There are two strategies for miRNA-based therapeutics: miRNA mimics and miRNA inhibitors, depending on whether miRNA should be replaced or downregulated to manipulate the amount of mRNA target in the cell [72]. miRNA mimics are synthetic double-stranded oligonucleotides that can overexpress the corresponding endogenous miRNA sequence and mimic the function of the target miRNA, resulting in the downregulation of cancer cells proliferation, thereby promoting mRNA inhibition. Owing to the tumor-suppressor role of miRNAs, miRNA mimics could potentially serve as therapeutic agents for cancer management [73]. Unlike miRNA mimics, miRNA inhibitors, also known as anti-miRs, are designed as complementary single-stranded RNA analogs based on the generation of ASOs to target endogenous miRNAs. Anti-miRNAs can specifically block the upregulated expression of miRNAs associated with cancer development [74, 75].
As a potential tumor-suppressive miRNA, miR-34a is lacking in stem cells and advanced tumors. MRX34 is an LNP that can bind to miR-34a mimics[76]. MRX34 could enhance the effect of radiation therapy by inhibiting DNA repair in a non-small cell lung cancer (NSCLC) mouse model [77].
As a therapeutic target, miR-155 is a well-studied miRNA in many hematological malignancies and is mainly associated with poor prognosis in lymphoma and leukemia [78]. Cobomarsen (MRG-106), an inhibitor of miR-155, is currently undergoing clinical trials and can suppress the downstream targets or survival pathways of miR-155, including JAK/STAT, MAPK/ERK, and PI3K/AKT in vitro [79].
Remlarsen (MRG-201) was designed to mimic the activity of miR-29 and is currently being studied to determine whether it can limit the formation of fibrous scar tissues in keloids. Huang et al. found that high expression of miR-29 could regulate the STAT3 signaling pathway to inhibit the proliferation, invasion, and metastasis of uterine leiomyoma in vitro; thus, miR-29 might be a new target for treating uterine leiomyoma [80]
Several miRNA drugs have also undergone preclinical trials. For example, the miR-122 mimic could improve the sensitivity of breast cancer cells to chemotherapy drugs, such as alpelisib and trametinib, and reduce the emergence of drug resistance [81]. When the miR-151a mimic was transfected into a drug-resistant glioblastoma cell line, the cells showed miR-151a-induced enhancement of chemosensitivity to temozolomide by modulation of XRCC4-mediated DNA repair [82]. The expression level of miR-634 in gastric cancer was significantly lower than that in normal adjacent tissues, and the proliferation, migration, and invasion abilities of gastric cancer cell lines were inhibited upon transfection of the miR-634 mimic [83].
Both siRNAs and miRNAs are meaningful gene-silencing tools, and four siRNA drug candidates have been approved for marketing. However, many miRNA drugs were mostly terminated owing to safety issues, and no drug candidates have entered phase III clinical trials. Consequently, it is difficult to identify miRNAs that regulate specific genes, as they can lead to unexpected side effects. Addressing the specificity of miRNA drugs can advance the application of miRNAs in clinical settings (Table 4).
Messenger RNA (mRNA) vaccine
mRNA, known as messenger RNA, is a single-stranded RNA complementary to the antisense DNA. It carries genetic information and directs protein synthesis in the cytoplasm [84]. As an intermediary of the central dogma of molecular biology, mRNA plays a vital role in protein production. Since Wolf et al. first successfully introduced in vitro transcription (IVT) mRNA in animals in 1900 [85], mRNA-based therapeutics, such as mRNA vaccines, have made significant progress in preventing infectious diseases and tumor immunotherapy over the past decade. In particular, because of the relatively low risk of insertion mutagenesis and lack of need to enter the nucleus for functionality, mRNA vaccines have become a hotspot in the prevention and treatment of coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 [86]. On August 23, 2021, tozinameran (Comirnaty, BNT162b2), developed by Pfizer-BioNTech, became the first mRNA vaccine officially approved for commercialization by the FDA to prevent COVID-19 among individuals aged ≥ 16 years old [87, 88]. Subsequently, the mRNA vaccine elasomeran (Spikevax, mRNA-1273), developed by Moderna, was approved for marketing [89]. These two mRNA vaccines have promoted the development of mRNA-based therapy and served as a blueprint for mRNA vaccines in cancer treatment.
Compared to other vaccines, mRNA vaccines have many advantages, such as good safety, high efficacy, shorter development cycle, and lower cost [90]. First, mRNA can be directly translated into proteins in the cytoplasm, whereas plasmid DNA and viral vectors are at risk of mutations caused by gene insertion or infection. Second, cells do not need to be involved in producing mRNA vaccines using IVT mRNA technology, thus avoiding contamination by proteins or viruses; mRNA vaccines can therefore be rapidly and economically mass-produced. In addition, based on current research data, patients showed good tolerance to mRNA vaccines, allowing repeated inoculation of mRNA vaccines.
With the development of mRNA vaccines, mRNA cancer vaccines have gradually become a research focus over the last five years (Table 5). Since cancer progression is correlated with immune response, mRNA cancer vaccines also show significant advantages in cancer immunotherapy. Through artificial design, mRNA cancer vaccines can deliver and express cancer antigens and activate innate immunity [91, 92]. Moreover, with the help of IVT mRNA technology, mRNA cancer vaccines can be used to advance personalized tumor immunotherapy. Therefore, mRNA cancer vaccines have great potential for use in antitumor therapy.mRNA cancer vaccines work by using related delivery vectors and adjuvants to deliver mRNA fragments encoding tumor antigen proteins or immunomodulatory molecules directly targeting cells. Once the tumor antigen is recognized by human immune cells, the body triggers an antitumor immune response [93]. mRNA cancer vaccines can be divided into two categories: mRNA direct cancer vaccines and mRNA dendritic cell (DC) vaccines. Using granulocyte–macrophage colony-stimulating factor (GM-CSF) as an adjuvant, mRNA direct cancer vaccines induce tumor-specific T-cell responses for tumor rejection by encoding cancer antigens, such as tumor-associated antigens (TAAs) and tumor-specific antigens. In contrast, mRNA DC vaccines obtain mRNA using IVT technology. After transfection into DCs, mRNA is translated into antigens in the cytoplasm to activate DCs, and activated DCs can present TAAs and stimulate the immune system response against tumors. Currently, there is sufficient promising preclinical evidence and many ongoing clinical trials on mRNA vaccines for cancer treatment [94] (Fig. 3).

The schematic diagram of mRNA direct cancer vaccine and mRNA dendritic cell (DC) vaccine excitation of immune cells to kill tumor cell
TriMixDC is an autologous monocyte-derived DC electroporated with mRNA encoding a mixture of three immune-modulating molecules, including active TLR-4, CD40 ligand, and CD70 [95], which can stimulate T cells. TriMixDC-MEL, obtained by co-electroporation of TriMixDC with an mRNA encoding melanoma-associated antigens, showed favorable safety, strong immunogenicity. It produced a durable tumor response in 4 of 15 patients with advanced melanoma after intravenous and intradermal combined administration (NCT01066390) [96]. When combined with the immune-checkpoint blocker ipilimumab to overcome immune tolerance, the median progression-free survival and overall survival rates improved in patients with advanced melanoma treated with TriMixDC-MEL, and robust CD8+ T-cell responses were detected (NCT01302496) [97].
CV9103 and CV9104 are both mRNA-based vaccines based on RNActive® technology. CV9103 encodes four specific antigens present in cancer cells: prostate-specific antigen (PSA), prostate-specific membrane antigen (PSMA), prostate stem cell antigen (PSCA), and six-transmembrane epithelial antigen of the prostate (STEAP). The follow-up vaccine CV9104 encodes six antigens, i.e., PSA, PSMA, PSCA, STEAP, mucin 1, and prostatic acid phosphatase (PAP), which are overexpressed in prostate cancer cells compared to those in healthy tissues [98]. These antigens are appropriate targets for intervention and can induce adaptive immunity in humans. In a phase I/II clinical trial, CV9103 displayed safety and activated immunogenicity in patients with advanced prostate cancer, and one patient showed a confirmed PSA response [99]. However, the subsequent trial with CV9104 for prostate cancer was terminated because there was no significant improvement in overall survival compared to that in patients treated with placebo [100].
CV9201 is another mRNA vaccine based on RNActive®, which encodes five NSCLC antigens, including melanoma antigen family C1 (MAGE-C1), MAGE family C2, New York esophageal squamous cell carcinoma 1 (NY-ESO-1), trophoblast glycoprotein (5T4), and survivin. CV9201 showed an acceptable tolerability profile and evidence of immune activation in a phase I/IIa dose-escalation experiment (NCT00923312) [101]. CV9202 is also a self-adjuvanted mRNA vaccine encoding six NSCLC-associated antigens, namely NY-ESO-1, MAGE-C1, MAGE-C2, survivin, 5T4, and MUC-1, which induce targeted immune responses. A phase Ib clinical trial demonstrated that treatment with CV9202 combined with radiotherapy in 26 patients with stage IV NSCLC was well tolerated, and antigen-specific immune responses were detected in 84% of patients (NCT01915524) [102]. Further clinical trials on CV9202 evaluating its safety and preliminary efficacy, combined with the immune checkpoint inhibitors durvalumab (anti-PD-L1) or remelimumab (anti-CTLA-4), have been conducted (NCT03164772) [103].
BNT111 is an intravenously administered tetravalent liposomal RNA vaccine encoding four TAAs: NY-ESO-1, melanoma-associated antigen A3 (MAGE-A3), tyrosinase, and transmembrane phosphatase with tensin homology. These antigens show restricted normal tissue expression, high immunogenicity, and high prevalence in melanoma. When entering the body, BNT111 is taken up by antigen-presenting cells (APCs), translocated to the cytoplasm, and translated into four tumor-associated proteins, ultimately triggering antigen-specific CD8+ and CD4+ T cell responses. A first-in-human dose-escalation phase I clinical study showed that BNT111 exhibited good safety and induced durable objective immune responses in patients with advanced melanoma (NCT02410733) [104]. An open-label, randomized, multicenter phase II trial is currently ongoing to evaluate the safety, tolerability, and efficacy of BNT111, in combination with cemiplimab, in patients with unresectable stage III or IV melanoma with anti-PD-1-refractory or relapse after anti-PD-1 therapy (NCT04526899).
Autogene cevumeran, also called RO7198457, consists of RNA-Lipoplex (RNA-LPX) and is an individualized neoantigen-specific therapy (iNeST) that can potentially stimulate and expand neoantigen-specific CD4+ and CD8+ T cells, leading to antitumor responses. Currently, four clinical trials are underway or under recruitment. One is a first-human phase I study designed to evaluate the safety, tolerability, immune response, and pharmacokinetics of RO7198457 as a single agent or in combination with the anti-PD-L1 antibody atezolizumab in participants with locally advanced or metastatic tumors (NCT03289962). A randomized phase II study of RO7198457 in combination with pembrolizumab was conducted in patients with previously untreated advanced melanoma (NCT03815058).
Challenges
Despite considerable progress in RNA-based therapeutics, two major challenges remain for clinical application: selecting the best drug target from a large number of possible targets and optimizing the delivery of RNA drugs to individual tumors [105]. The choice of targets and delivery routes can enhance drug efficacy while minimizing side effects in normal tissues and increasing drug safety.
Target
Cancer is caused by a variety of complex factors, including genetic lesions. Many small-molecule therapeutics directly target key genetic genes for cancer treatment. In RNA-based drug development, we should seriously consider potential genetic targets and concentrate on those that are difficult to target using small molecules. For example, the MYC oncogene family is frequently deregulated in most human cancers and is associated with poor prognosis and unfavorable patient survival [65]. One of the potential ways to treat cancer is to inhibit MYC expression; however, owing to the disorderly structure of the MYC protein, there is currently no small-molecule inhibitor with good activity and high selectivity that directly targets MYC [106].
KRAS is among the most common oncogenes in solid tumors. However, few KRAS-targeted drugs are currently available. Currently, only Lumakras (Sotorasib, Amgen), approved by the FDA on May 28, 2021, is used to treat patients with a proto-oncogene KRAS G12C-mutated NSCLC, the first targeted drug approved for KRAS mutations [107]. Therefore, these oncogenes can be preferred targets against which oligonucleotide drugs can be developed.
Cancer is a multifactorial disease that involves multiple genes. Thus, targeting only one associated gene may be insufficient. Combination therapies that simultaneously target multiple affected genes can be a viable approach in the future. Oligonucleotide therapeutics are particularly amenable to combination therapy because the same drug modality can be applied to target multiple cancer drivers [12].
Although neoantigens have shown great potential in cancer immunotherapies, identifying suitable cancer neoantigens that can be targeted by mRNA vaccines remains a challenge. Alternative splicing occurs widely in tumors and has been proven to contribute to the generation of candidate neoantigens [108]. However, abnormal alternative splicing occurs in many tumors, which may lead to the translation of abnormal transcripts into tumor-specific proteins. High-throughput technologies enable systematic characterization of alternative splicing and may identify alternative splicing-derived cancer neoantigens from RNA-seq data. It is also possible to design personalized mRNA vaccines based on alternative splicing-derived cancer neoantigens [109].
Delivery
Currently, delivery is among the greatest barriers to the widespread application of RNA-based therapeutics. In particular, safe, efficient, and targeted delivery of oligonucleotide drugs and mRNA vaccines remains a major challenge [16, 110] (Table 6). First, naked and unmodified RNAs are poorly stable, easily degraded by multiple circulating ribonucleases (RNases) and hydrolases, and rapidly cleared by renal clearance upon systemic injection. Second, as a hydrophilic negatively charged macromolecule, oligonucleotide drugs have limited ability to penetrate cell membranes, making it difficult to enter the cytoplasm or nucleus. In addition, ASO and siRNA sequences may have off-target effects, leading to non-specific gene knockdown and activation of the innate immune system via Toll-like receptors. Thus, optimized RNA drug delivery systems can protect RNA structures from degradation, increase targeting capacity, and reduce toxic side effects.
With the development of feasible technologies that improve the druggability of RNA molecules, various viral and non-viral delivery systems have emerged. Currently, there are three key viral vectors for gene therapy: adenovirus (AdV), adeno-associated virus (AAV), and lentivirus [111]. Over the past two decades, they have achieved preclinical and clinical successes. AAV was first identified in laboratory AdV preparations in the mid-1960s [112]. Recombinant AAV is also a leading platform for in vivo delivery of gene therapies [113].
However, viral vectors pose toxicity issues and are unsafe for humans owing to their inflammatory and immunogenic effects, which limit their clinical translation [114]. Compared with viral vectors, non-viral vectors have a wider range of application, and they have overcome some issues, including high cost, immunogenicity, and toxictity [115]. Therefore, relatively safe non-viral vectors, such as lipid-based delivery systems, polymer-based nanoparticles, and inorganic nanoparticles, are rapidly evolving [116].
Lipid-based delivery systems, such as micelles, liposomes, and LNP, can be easily synthesized through chemical reactions [117, 118]. The efficiency of delivering RNA therapy to the liver is greatly improved by distinct chemical structures and more reasonable lipid molecular design. LNPs are one of the most widely used non-viral delivery systems for oligonucleotide drugs and mRNA vaccines, and their advantages include ease of production, biodegradability, protection of the embedded RNA from RNase degradation and renal clearance, promotion of cellular uptake, and endosomal escape [119, 120]. Recently, LNP has received global attention as an important component of mRNA vaccines, playing a key role in effectively protecting and transporting mRNA into cells. Polymers are the second largest class of nucleic acid-delivery vehicles after lipids. Cationic polymers form stable complexes with anionic nucleic acids, providing a versatile, scalable, and easily adaptable platform for efficient nucleic acid delivery while minimizing the immune response and cytotoxicity [121]. The efficiency of RNA delivery into cells can be altered by adjusting polymer polarity, degradation, and molecular weight. Dendrimers are another type of polymer that deliver RNA [122]. These macromolecules are centered on a core molecule and synthesize highly branched polymers via repetitive growth reactions. Modifying the dendrimer structure can protect nucleotides from enzymatic degradation.
With the development of nanomaterials, inorganic nanocarriers provide a unique platform for the effective delivery of nucleic acid drugs to tumor cells due to their high stability, good biocompatibility, low immunogenicity, and mass production, such as gold nanoparticles (AuNPs) [123, 124], silica nanoparticles [125], and carbon nanotubes. AuNPs are [126] a classical inorganic nanocarrier with good chemical stability and biocompatibility [127]. Nucleic acid chains are covalently attached to the AuNP core via mercaptan groups. The abovementioned NU-0129 is a siRNA drug designed based on AuNPs to target the oncogene Bcl2L12 in GBM treatment. Silica is another type of biodegradable, safe, and stable carrier nanomaterial. Mesoporous silica nanoparticles (MSNs) have attracted great interest for their easy functionalization, biocompatibility, high specific surface area, and biodegradability [128]. MSNs can effectively deliver drugs to cells and easily escape from endosomes, thereby enhancing anti-tumor effects [129]. Bertucci et al. co-delivered anti-miR-221 PNA and temozolomide to induce drug-resistant glioma cell apoptosis by using MSNs [130].
Viral vectors are more effective but more immunogenic than non-viral delivery systems. Non-viral gene vectors are generally versatile, simple, cost-effective, and potentially safer alternatives but may lack adequate clinical efficacy. Therefore, when selecting a delivery vehicle for an RNA drug, it is necessary to consider many aspects and select the most suitable one to maximize efficacy and minimize side effects.
Conclusion
RNAs can be used both as a target and a drug. The successful development of various new oligonucleotide drugs and mRNA COVID-19 vaccines has resulted in an increasing number of RNA-based drugs that show great promise for clinical translation. RNA therapy offers an innovative approach to new drugs for cancer treatment, with several important advantages, including high specificity for the target, modular development by replacing RNA sequences, predictability in terms of pharmacokinetics and pharmacodynamics, and relative safety. However, some challenges are associated with this therapy, including the selection of suitable targets, innovation, and optimization of delivery systems.
Although these non-protein-targeted drugs have certain limitations, the market potential of RNA therapeutics in the treatment of tumors and other diseases cannot be ignored, along with the continuous breakthrough of core technologies, such as chemical modification and delivery systems. The successful commercialization of oligonucleotide drugs and mRNA vaccines has promoted a wave of nucleic acid drug research and development, and large-scale production and economic benefits have now become the main focus point. Non-protein-targeted drugs can overcome the limitations of the druggability of small molecule and antibody drugs and are thus expected to become the third major drug type.
With a deeper understanding of the multiple types and functions of RNA, the ability to generate modified RNAs with higher stability and drug activity, and nanotechnology-based vectors capable of targeted delivery of these RNAs into cells, the development of targeted RNA therapeutic options with multiple specificities is expected to change the landscape of cancer treatment in humans.
References
Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021[J]. CA: Cancer J Clin. 2021;71(1):7.
Chatterjee N, Bivona TG. Polytherapy and targeted cancer drug resistance[J]. Trends In Cancer. 2019;5(3):170–82.
Imai K, Takaoka A. Comparing antibody and small-molecule therapies for cancer[J]. Nat Rev Cancer. 2006;6(9):714–27.
Wu Q, Qian W, Sun X, et al. Small-molecule inhibitors, immune checkpoint inhibitors, and more: FDA-approved novel therapeutic drugs for solid tumors from 1991 to 2021[J]. J Hematol Oncol. 2022;15(1):143.
Moore AR, Rosenberg SC, Mccormick F, et al. RAS-targeted therapies: is the undruggable drugged?[J]. Nat Rev Drug Discovery. 2020;19(8):533–52.
Lundstrom K. RNA-based drugs and vaccines[J]. Expert Rev Vaccines. 2015;14(2):253–63.
Yu A-M, Tu M-J. Deliver the promise: RNAs as a new class of molecular entities for therapy and vaccination[J]. Pharmacol Ther. 2022;230:107967.
Zogg H, Singh R, Ro S. Current advances in RNA therapeutics for human diseases[J]. Int J Mol Sci. 2022;23(5):2736.
Barata P, Sood AK, Hong DS. RNA-targeted therapeutics in cancer clinical trials: current status and future directions[J]. Cancer Treat Rev. 2016;50:35–47.
Xu Y, Chen W, Liang J, et al. The miR-1185-2-3p-GOLPH3L pathway promotes glucose metabolism in breast cancer by stabilizing p53-induced SERPINE1[J]. J Exp Clin Cancer Res : CR. 2021;40(1):47.
Zamecnik PC, Stephenson ML. Inhibition of Rous sarcoma virus replication and cell transformation by a specific oligodeoxynucleotide[J]. Proc Natl Acad Sci USA. 1978;75(1):280–4.
Xiong H, Veedu RN, Diermeier SD. Recent advances in oligonucleotide therapeutics in oncology[J]. Int J Mol Sci. 2021;22(7):3295.
Taniguchi H, Suzuki Y, Imai K, et al. Antitumoral RNA-targeted oligonucleotide therapeutics: the third pillar after small molecule inhibitors and antibodies[J]. Cancer Sci. 2022;113(9):2952–61.
Hair P, Cameron F, Mckeage K. Mipomersen sodium: first global approval[J]. Drugs. 2013;73(5):487–93.
Quemener AM, Bachelot L, Forestier A, et al. The powerful world of antisense oligonucleotides: from bench to bedside[J]. Wiley Interdiscip Rev RNA. 2020;11(5):e1594.
Roberts TC, Langer R, Wood MJA. Advances in oligonucleotide drug delivery[J]. Nat Rev Drug Discovery. 2020;19(10):673–94.
Heo Y-A. Golodirsen: first approval[J]. Drugs. 2020;80(3):329–33.
Ackermann EJ, Guo S, Benson MD, et al. Suppressing transthyretin production in mice, monkeys and humans using 2nd-Generation antisense oligonucleotides[J]. Amyloid : Int J Exp Clin Invest : J Int Society Amyloidosis. 2016;23(3):148–57.
Gertz MA. Hereditary ATTR amyloidosis: burden of illness and diagnostic challenges[J]. Am J Manag Care. 2017;23(7 Suppl):S107–12.
Lebedeva I, Stein CA. Antisense oligonucleotides: promise and reality. Annu Rev Pharmacol Toxicol. 2001;41:403–19.
Liu G, Kolesar J, Mcneel DG, et al. A phase I pharmacokinetic and pharmacodynamic correlative study of the antisense Bcl-2 oligonucleotide g3139, in combination with carboplatin and paclitaxel, in patients with advanced solid tumors[J]. Clin Cancer Res : J Am Asso Cancer Res. 2008;14(9):2732–9.
Rudin CM, Salgia R, Wang X, et al. Randomized phase II Study of carboplatin and etoposide with or without the bcl-2 antisense oligonucleotide oblimersen for extensive-stage small-cell lung cancer: CALGB 30103[J]. J Clin Oncol : J Am Soc Clin Oncol. 2008;26(6):870–6.
Rudin CM, Otterson GA, Mauer AM, et al. A pilot trial of G3139, a bcl-2 antisense oligonucleotide, and paclitaxel in patients with chemorefractory small-cell lung cancer[J]. Ann Oncol : J Eur Soc Med Oncol. 2002;13(4):539–45.
Tolcher AW, Kuhn J, Schwartz G, et al. A Phase I pharmacokinetic and biological correlative study of oblimersen sodium (genasense, g3139), an antisense oligonucleotide to the bcl-2 mRNA, and of docetaxel in patients with hormone-refractory prostate cancer[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2004;10(15):5048–57.
Tolcher AW, Chi K, Kuhn J, et al. A phase II, pharmacokinetic, and biological correlative study of oblimersen sodium and docetaxel in patients with hormone-refractory prostate cancer[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2005;11(10):3854–61.
Sternberg CN, Dumez H, Van Poppel H, et al. Docetaxel plus oblimersen sodium (Bcl-2 antisense oligonucleotide): an EORTC multicenter, randomized phase II study in patients with castration-resistant prostate cancer[J]. Ann Oncol : J Eur Soc Med Oncol. 2009;20(7):1264–9.
Rom J, Von Minckwitz G, Eiermann W, et al. Oblimersen combined with docetaxel, adriamycin and cyclophosphamide as neo-adjuvant systemic treatment in primary breast cancer: final results of a multicentric phase I study[J]. Ann Oncol : J Eur Soc Med Oncol. 2008;19(10):1698–705.
Mita MM, Ochoa L, Rowinsky EK, et al. A phase I, pharmacokinetic and biologic correlative study of oblimersen sodium (Genasense, G3139) and irinotecan in patients with metastatic colorectal cancer[J]. Ann Oncol : J Eur Soc Med Oncol. 2006;17(2):313–21.
Gagliardi M, Ashizawa AT. The challenges and strategies of antisense oligonucleotide drug delivery[J]. Biomedicines. 2021;9(4):433.
Ohanian M, Tari Ashizawa A, Garcia-Manero G, et al. Liposomal Grb2 antisense oligodeoxynucleotide (BP1001) in patients with refractory or relapsed haematological malignancies: a single-centre, open-label, dose-escalation, phase 1/1b trial[J]. Lancet Haematol. 2018;5(4):e136–46.
Wilson MR, Zoubeidi A. Clusterin as a therapeutic target[J]. Expert Opin Ther Targets. 2017;21(2):201–13.
Chi KN, Hotte SJ, Yu EY, et al. Randomized phase II study of docetaxel and prednisone with or without OGX-011 in patients with metastatic castration-resistant prostate cancer[J]. J Clin Oncol : J Am Soc Clin Oncol. 2010;28(27):4247–54.
Sridhar SS, Freedland SJ, Gleave ME, et al. Castration-resistant prostate cancer: from new pathophysiology to new treatment[J]. Eur Urol. 2014;65(2):289–99.
Kumano M, Furukawa J, Shiota M, et al. Cotargeting stress-activated Hsp27 and autophagy as a combinatorial strategy to amplify endoplasmic reticular stress in prostate cancer[J]. Mol Cancer Ther. 2012;11(8):1661–71.
Chi KN, Yu EY, Jacobs C, et al. A phase I dose-escalation study of apatorsen (OGX-427), an antisense inhibitor targeting heat shock protein 27 (Hsp27), in patients with castration-resistant prostate cancer and other advanced cancers[J]. Ann Oncol : J Eur Soc Med Oncol. 2016;27(6):1116–22.
Prakash TP, Siwkowski A, Allerson CR, et al. Antisense oligonucleotides containing conformationally constrained 2’,4’-(N-methoxy)aminomethylene and 2’,4’-aminooxymethylene and 2’-O,4’-C-aminomethylene bridged nucleoside analogues show improved potency in animal models[J]. J Med Chem. 2010;53(4):1636–50.
Shastri A, Choudhary G, Teixeira M, et al. Antisense STAT3 inhibitor decreases viability of myelodysplastic and leukemic stem cells[J]. J Clin Investig. 2018;128(12):5479–88.
Hong D, Kurzrock R, Kim Y, et al. AZD9150, a next-generation antisense oligonucleotide inhibitor of STAT3 with early evidence of clinical activity in lymphoma and lung cancer[J]. Sci Transl Med. 2015;7(314):314ra185.
Odate S, Veschi V, Yan S, et al. Inhibition of with the generation 2.5 antisense oligonucleotide, AZD9150, decreases neuroblastoma tumorigenicity and increases chemosensitivity[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2017;23(7):1771–84.
Reilley MJ, Mccoon P, Cook C, et al. STAT3 antisense oligonucleotide AZD9150 in a subset of patients with heavily pretreated lymphoma: results of a phase 1b trial[J]. J Immunother Cancer. 2018;6(1):119.
Rudin CM, Marshall JL, Huang CH, et al. Delivery of a liposomal c-raf-1 antisense oligonucleotide by weekly bolus dosing in patients with advanced solid tumors: a phase I study[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2004;10(21):7244–51.
Gokhale PC, Zhang C, Newsome JT, et al. Pharmacokinetics, toxicity, and efficacy of ends-modified raf antisense oligodeoxyribonucleotide encapsulated in a novel cationic liposome[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2002;8(11):3611–21.
Dritschilo A, Huang CH, Rudin CM, et al. Phase I study of liposome-encapsulated c-raf antisense oligodeoxyribonucleotide infusion in combination with radiation therapy in patients with advanced malignancies[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2006;12(4):1251–9.
Greenberger LM, Horak ID, Filpula D, et al. A RNA antagonist of hypoxia-inducible factor-1alpha, EZN-2968, inhibits tumor cell growth[J]. Mol Cancer Ther. 2008;7(11):3598–608.
Jeong W, Rapisarda A, Park SR, et al. Pilot trial of EZN-2968, an antisense oligonucleotide inhibitor of hypoxia-inducible factor-1 alpha (HIF-1α), in patients with refractory solid tumors[J]. Cancer Chemother Pharmacol. 2014;73(2):343–8.
Downward J. RNA interference[J]. BMJ (Clin Res ed). 2004;328(7450):1245–8.
Zhu KY, Palli SR. Mechanisms, applications, and challenges of insect RNA interference[J]. Annu Rev Entomol. 2020;65:293–311.
Alshaer W, Zureigat H, Al Karaki A, et al. siRNA: Mechanism of action, challenges, and therapeutic approaches[J]. Eur J Pharmacol. 2021;905:174178.
Zhang MM, Bahal R, Rasmussen TP, et al. The growth of siRNA-based therapeutics: updated clinical studies[J]. Biochem Pharmacol. 2021;189:114432.
Iwakawa H-O, Tomari Y. Life of RISC: Formation, action, and degradation of RNA-induced silencing complex[J]. Mol Cell. 2022;82(1):30–43.
Wood H. FDA approves patisiran to treat hereditary transthyretin amyloidosis[J]. Nat Rev Neurol. 2018;14(10):570.
Weng Y, Xiao H, Zhang J, et al. RNAi therapeutic and its innovative biotechnological evolution[J]. Biotechnol Adv. 2019;37(5):801–25.
Sheridan C. PCSK9-gene-silencing, cholesterol-lowering drug impresses[J]. Nat Biotechnol. 2019;37(12):1385–7.
Davis ME, Zuckerman JE, Choi CHJ, et al. Evidence of RNAi in humans from systemically administered siRNA via targeted nanoparticles[J]. Nature. 2010;464(7291):1067–70.
Zuckerman JE, Gritli I, Tolcher A, et al. Correlating animal and human phase Ia/Ib clinical data with CALAA-01, a targeted, polymer-based nanoparticle containing siRNA[J]. Proc Natl Acad Sci USA. 2014;111(31):11449–54.
Strumberg D, Schultheis B, Traugott U, et al. Phase I clinical development of Atu027, a siRNA formulation targeting PKN3 in patients with advanced solid tumors[J]. Int J Clin Pharmacol Ther. 2012;50(1):76–8.
Schultheis B, Strumberg D, Santel A, et al. First-in-human phase I study of the liposomal RNA interference therapeutic Atu027 in patients with advanced solid tumors[J]. J Clin Oncol : J Am Soc Clin Oncol. 2014;32(36):4141–8.
Schultheis B, Strumberg D, Kuhlmann J, et al. Safety, efficacy and pharcacokinetics of targeted therapy with the liposomal RNA interference therapeutic Atu027 combined with gemcitabine in patients with pancreatic adenocarcinoma. A randomized phase Ib/IIa study[J]. Cancers. 2020;12(11):3130.
ZordeKhvalevsky E, Gabai R, Rachmut IH, et al. Mutant KRAS is a druggable target for pancreatic cancer[J]. Proc Natl Acad Sci USA. 2013;110(51):20723–8.
Golan T, Khvalevsky EZ, Hubert A, et al. RNAi therapy targeting KRAS in combination with chemotherapy for locally advanced pancreatic cancer patients[J]. Oncotarget. 2015;6(27):24560–70.
Xu X, Ho W, Zhang X, et al. Cancer nanomedicine: from targeted delivery to combination therapy[J]. Trends Mol Med. 2015;21(4):223–32.
El Dika I, Lim HY, Yong WP, et al. An open-label, multicenter, phase I, dose escalation study with phase II expansion cohort to determine the safety, pharmacokinetics, and preliminary antitumor activity of intravenous TKM-080301 in subjects with advanced hepatocellular carcinoma[J]. The Oncologist. 2019;24(6):747.
Xiao T, Xiao Y, Wang W, et al. Targeting EphA2 in cancer[J]. J Hematol Oncol. 2020;13(1):114.
Wagner MJ, Mitra R, Mcarthur MJ, et al. Preclinical mammalian safety studies of EPHARNA (DOPC Nanoliposomal EphA2-Targeted siRNA)[J]. Mol Cancer Ther. 2017;16(6):1114–23.
Chen H, Liu H, Qing G. Targeting oncogenic Myc as a strategy for cancer treatment[J]. Signal Transduct Target Ther. 2018;3:5.
Miller AJ, Chang A, Cunningham PN. Chronic microangiopathy due to DCR-MYC, a Myc-targeted short interfering RNA[J]. Am J Kidney Dis. 2020;75(4):513–6.
Kumthekar P, Ko CH, Paunesku T, et al. A first-in-human phase 0 clinical study of RNA interference-based spherical nucleic acids in patients with recurrent glioblastoma[J]. Sci Transl Med. 2021;13(584):3945.
Bartel DP. Metazoan MicroRNAs[J]. Cell. 2018;173(1):20–51.
Krol J, Loedige I, Filipowicz W. The widespread regulation of microRNA biogenesis, function and decay[J]. Nat Rev Genet. 2010;11(9):597–610.
Baek D, Villén J, Shin C, et al. The impact of microRNAs on protein output[J]. Nature. 2008;455(7209):64–71.
Calin GA, Dumitru CD, Shimizu M, et al. Frequent deletions and down-regulation of micro- RNA genes miR15 and miR16 at 13q14 in chronic lymphocytic leukemia[J]. Proc Natl Acad Sci USA. 2002;99(24):15524–9.
Ha M, Kim VN. Regulation of microRNA biogenesis[J]. Nat Rev Mol Cell Biol. 2014;15(8):509–24.
Setten RL, Rossi JJ, Han S-P. The current state and future directions of RNAi-based therapeutics[J]. Nat Rev Drug Discovery. 2019;18(6):421–46.
Iorio MV, Croce CM. MicroRNA dysregulation in cancer: diagnostics, monitoring and therapeutics. A comprehensive review[J]. EMBO Mol Med. 2012;4(3):143–59.
Li Z, Rana TM. Therapeutic targeting of microRNAs: current status and future challenges[J]. Nat Rev Drug Discovery. 2014;13(8):622–38.
Li WJ, Wang Y, Liu R, et al. MicroRNA-34a: potent tumor suppressor, cancer stem cell inhibitor, and potential anticancer therapeutic[J]. Front Cell Dev Biol. 2021;9:640587.
Cortez MA, Valdecanas D, Niknam S, et al. In vivo delivery of miR-34a sensitizes lung tumors to radiation through RAD51 regulation[J]. Mol Ther Nucleic Acids. 2015;4:e270.
Witten L, Slack FJ. miR-155 as a novel clinical target for hematological malignancies[J]. Carcinogenesis. 2020;41(1):2–7.
Seto AG, Beatty X, Lynch JM, et al. Cobomarsen, an oligonucleotide inhibitor of miR-155, co-ordinately regulates multiple survival pathways to reduce cellular proliferation and survival in cutaneous T-cell lymphoma[J]. Br J Haematol. 2018;183(3):428–44.
Huang D, Xue H, Shao W, et al. Inhibiting effect of miR-29 on proliferation and migration of uterine leiomyoma via the STAT3 signaling pathway[J]. Aging. 2022;14(3):1307–20.
Baldassari F, Zerbinati C, Galasso M, et al. Screen for microRNA and drug interactions in breast cancer cell lines points to miR-126 as a modulator of CDK4/6 and PIK3CA inhibitors[J]. Front Genet. 2018;9:174.
Zeng A, Wei Z, Yan W, et al. Exosomal transfer of miR-151a enhances chemosensitivity to temozolomide in drug-resistant glioblastoma[J]. Cancer Lett. 2018;436:10–21.
Guo J, Zhang C-D, An J-X, et al. Expression of miR-634 in gastric carcinoma and its effects on proliferation, migration, and invasion of gastric cancer cells[J]. Cancer Med. 2018;7(3):776–87.
Pardi N, Hogan MJ, Porter FW, et al. mRNA vaccines - a new era in vaccinology[J]. Nat Rev Drug Discovery. 2018;17(4):261–79.
Wolff JA, Malone RW, Williams P, et al. Direct gene transfer into mouse muscle in vivo[J]. Science (New York NY). 1990;247(4949 Pt 1):1465–8.
Fang E, Liu X, Li M, et al. Advances in COVID-19 mRNA vaccine development[J]. Signal Transduct Target Ther. 2022;7(1):94.
Woodworth KR, Moulia D, Collins JP, et al. The advisory committee on immunization practices’ interim recommendation for use of Pfizer-BioNTech COVID-19 vaccine in children aged 5–11 years - United States, November 2021[J]. MMWR Morb Mortal Wkly Rep. 2021;70(45):1579–83.
Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine[J]. N Engl J Med. 2020;383(27):2603–15.
Nanduri S, Pilishvili T, Derado G, et al. Effectiveness of Pfizer-BioNTech and Moderna vaccines in preventing SARS-CoV-2 infection among nursing home residents before and during widespread circulation of the SARS-CoV-2 B.1.617.2 (Delta) variant - national healthcare safety network, March 1-August 1, 2021[J]. MMWR Morbid Mortal Week Rep. 2021;70(34):1163–6.
Lorentzen CL, Haanen JB, Met Ö, et al. Clinical advances and ongoing trials on mRNA vaccines for cancer treatment[J]. Lancet Oncol. 2022;23(10):e450–8.
Linares-Fernández S, Lacroix C, Exposito J-Y, et al. Tailoring mRNA Vaccine to balance innate/adaptive immune response[J]. Trends Mol Med. 2020;26(3):311–23.
Beck JD, Reidenbach D, Salomon N, et al. mRNA therapeutics in cancer immunotherapy[J]. Mol Cancer. 2021;20(1):69.
Van Hoecke L, Verbeke R, Dewitte H, et al. mRNA in cancer immunotherapy: beyond a source of antigen[J]. Mol Cancer. 2021;20(1):48.
Ke Y. Perspectives on mRNA vaccine development for cancer[J]. J Interferon Cytokine Res : J Int Soc Interferon Cytokine Res. 2022;42:592.
Bonehill A, Tuyaerts S, Van Nuffel AMT, et al. Enhancing the T-cell stimulatory capacity of human dendritic cells by co-electroporation with CD40L, CD70 and constitutively active TLR4 encoding mRNA[J]. Mol Ther : J Am Soc Gene Ther. 2008;16(6):1170–80.
Wilgenhof S, Van Nuffel AMT, Benteyn D, et al. A phase IB study on intravenous synthetic mRNA electroporated dendritic cell immunotherapy in pretreated advanced melanoma patients[J]. Ann Oncol : J Eur Soc Med Oncol. 2013;24(10):2686–93.
De Keersmaecker B, Claerhout S, Carrasco J, et al. TriMix and tumor antigen mRNA electroporated dendritic cell vaccination plus ipilimumab: link between T-cell activation and clinical responses in advanced melanoma[J]. J Immunother Cancer. 2020;8(1):e000329.
Rausch S, Schwentner C, Stenzl A, et al. mRNA vaccine CV9103 and CV9104 for the treatment of prostate cancer[J]. Hum Vaccin Immunother. 2014;10(11):3146–52.
Kübler H, Scheel B, Gnad-Vogt U, et al. Self-adjuvanted mRNA vaccination in advanced prostate cancer patients: a first-in-man phase I/IIa study[J]. J Immunother Cancer. 2015;3:26.
Saad F, Shore N, Zhang T, et al. Emerging therapeutic targets for patients with advanced prostate cancer[J]. Cancer Treat Rev. 2019;76:1–9.
Sebastian M, Schröder A, Scheel B, et al. A phase I/IIa study of the mRNA-based cancer immunotherapy CV9201 in patients with stage IIIB/IV non-small cell lung cancer[J]. Cancer Immunol, Immunother : CII. 2019;68(5):799–812.
Sebastian M, Papachristofilou A, Weiss C, et al. Phase Ib study evaluating a self-adjuvanted mRNA cancer vaccine (RNActive®) combined with local radiation as consolidation and maintenance treatment for patients with stage IV non-small cell lung cancer[J]. BMC Cancer. 2014;14:748.
Papachristofilou A, Hipp MM, Klinkhardt U, et al. Phase Ib evaluation of a self-adjuvanted protamine formulated mRNA-based active cancer immunotherapy, BI1361849 (CV9202), combined with local radiation treatment in patients with stage IV non-small cell lung cancer[J]. J Immunother Cancer. 2019;7(1):38.
Ugur S, Petra O, Evelyna D, et al. An RNA vaccine drives immunity in checkpoint-inhibitor-treated melanoma[J]. Nature. 2020;585(7823):107.
Dowdy SF. Overcoming cellular barriers for RNA therapeutics[J]. Nat Biotechnol. 2017;35(3):222–9.
Wang C, Zhang J, Yin J, et al. Alternative approaches to target Myc for cancer treatment[J]. Signal Transduct Target Ther. 2021;6(1):117.
Nakajima EC, Drezner N, Li X, et al. FDA approval summary: sotorasib for KRAS G12C-mutated metastatic NSCLC[J]. Clin Cancer Res : J Am Assoc Cancer Res. 2022;28(8):1482–6.
Zhang Z, Zhou C, Tang L, et al. Identification of personalized alternative splicing based neoantigens with RNA-seq[J]. Aging. 2020;12(14):14633–48.
Cheng R, Xu Z, Luo M, et al. Identification of alternative splicing-derived cancer neoantigens for mRNA vaccine development[J]. Brief Bioinform. 2022;23(2):bbab553.
Kowalski PS, Rudra A, Miao L, et al. Delivering the messenger: advances in technologies for therapeutic mRNA delivery[J]. Mol Ther : J Am Soc Gene Ther. 2019;27(4):710–28.
Bulcha JT, Wang Y, Ma H, et al. Viral vector platforms within the gene therapy landscape[J]. Signal Transduct Target Ther. 2021;6(1):53.
Atchison RW, Casto BC, Hammon WM. Adenovirus-associated defective virus particles[J]. Science (New York, NY). 1965;149(3685):754–6.
Sha S, Maloney AJ, Katsikis G, et al. Cellular pathways of recombinant adeno-associated virus production for gene therapy[J]. Biotechnol Adv. 2021;49:107764.
Mingozzi F, High KA. Immune responses to AAV vectors: overcoming barriers to successful gene therapy[J]. Blood. 2013;122(1):23–36.
Pan X, Veroniaina H, Su N, et al. Applications and developments of gene therapy drug delivery systems for genetic diseases[J]. Asian J Pharm Sci. 2021;16(6):687–703.
Yin H, Kanasty RL, Eltoukhy AA, et al. Non-viral vectors for gene-based therapy[J]. Nat Rev Genet. 2014;15(8):541–55.
Rezaee M, Oskuee RK, Nassirli H, et al. Progress in the development of lipopolyplexes as efficient non-viral gene delivery systems[J]. J Contr Release : J Contr Release Soc. 2016;236:1.
Wang C, Zhang Y, Dong Y. Lipid Nanoparticle-mRNA formulations for therapeutic applications[J]. Acc Chem Res. 2021;54(23):4283–93.
Hou X, Zaks T, Langer R, et al. Lipid nanoparticles for mRNA delivery[J]. Nat Rev Mater. 2021;6(12):1078–94.
Cullis PR, Hope MJ. Lipid nanoparticle systems for enabling gene therapies[J]. Mol Ther : J Am Soc Gene Ther. 2017;25(7):1467–75.
Boussif O, Lezoualc’h F, Zanta MA, et al. A versatile vector for gene and oligonucleotide transfer into cells in culture and in vivo: polyethylenimine[J]. Proc Natl Acad Sci USA. 1995;92(16):7297–301.
Singha K, Namgung R, Kim WJ. Polymers in small-interfering RNA delivery[J]. Nucleic Acid Ther. 2011;21(3):133–47.
Ghosh R, Singh LC, Shohet JM, et al. A gold nanoparticle platform for the delivery of functional microRNAs into cancer cells[J]. Biomaterials. 2013;34(3):807–16.
Ghosh P, Han G, De M, et al. Gold nanoparticles in delivery applications[J]. Adv Drug Deliv Rev. 2008;60(11):1307–15.
Wu S-H, Mou C-Y, Lin H-P. Synthesis of mesoporous silica nanoparticles[J]. Chem Soc Rev. 2013;42(9):3862–75.
Caoduro C, Hervouet E, Girard-Thernier C, et al. Carbon nanotubes as gene carriers: Focus on internalization pathways related to functionalization and properties[J]. Acta Biomater. 2017;49:36–44.
Song W-J, Du J-Z, Sun T-M, et al. Gold nanoparticles capped with polyethyleneimine for enhanced siRNA delivery[J]. Small. 2010;6(2):239–46.
Tang F, Li L, Chen D. Mesoporous silica nanoparticles: synthesis, biocompatibility and drug delivery[J]. Adv Mater (Deerfield Beach, Fla). 2012;24(12):1504–34.
Ahir M, Upadhyay P, Ghosh A, et al. Delivery of dual miRNA through CD44-targeted mesoporous silica nanoparticles for enhanced and effective triple-negative breast cancer therapy[J]. Biomater Sci. 2020;8(10):2939–54.
Bertucci A, Prasetyanto EA, Septiadi D, et al. Combined delivery of temozolomide and anti-miR221 PNA using mesoporous silica nanoparticles induces apoptosis in resistant glioma cells[J]. Small. 2015;11(42):5687–95.
Author information
Authors and Affiliations
Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Y., Lu, L., Song, F. et al. Research progress on non-protein-targeted drugs for cancer therapy. J Exp Clin Cancer Res 42, 62 (2023). https://doi.org/10.1186/s13046-023-02635-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13046-023-02635-y