
Abstract
Objective
To investigate whether T2-weighted imaging (T2WI)-based intratumoral and peritumoral radiomics can predict extranodal extension (ENE) and prognosis in patients with resectable rectal cancer.
Methods
One hundred sixty-seven patients with resectable rectal cancer including T3T4N + cases were prospectively included. Radiomics features were extracted from intratumoral, peritumoral 3 mm, and peritumoral-mesorectal fat on T2WI images. Least absolute shrinkage and selection operator regression were used for feature selection. A radiomics signature score (Radscore) was built with logistic regression analysis. The area under the receiver operating characteristic curve (AUC) was used to evaluate the performance of each Radscore. A clinical-radiomics nomogram was constructed by the most predictive radiomics signature and clinical risk factors. A prognostic model was constructed by Cox regression analysis to identify 3-year recurrence-free survival (RFS).
Results
Age, cT stage, and lymph node-irregular border and/or adjacent fat invasion were identified as independent clinical risk factors to construct a clinical model. The nomogram incorporating intratumoral and peritumoral 3 mm Radscore and independent clinical risk factors achieved a better AUC than the clinical model in the training (0.799 vs. 0.736) and validation cohorts (0.723 vs. 0.667). Nomogram-based ENE (hazard ratio [HR] = 2.625, 95% CI = 1.233–5.586, p = 0.012) and extramural vascular invasion (EMVI) (HR = 2.523, 95% CI = 1.247–5.106, p = 0.010) were independent risk factors for predicting 3-year RFS. The prognostic model constructed by these two indicators showed good performance for predicting 3-year RFS in the training (AUC = 0.761) and validation cohorts (AUC = 0.710).
Conclusion
The nomogram incorporating intratumoral and peritumoral 3 mm Radscore and clinical risk factors could predict preoperative ENE. Combining nomogram-based ENE and MRI-reported EMVI may be useful in predicting 3-year RFS.
Critical relevance statement
A clinical-radiomics nomogram could help preoperative predict ENE, and a prognostic model constructed by the nomogram-based ENE and MRI-reported EMVI could predict 3-year RFS in patients with resectable rectal cancer.
Key points
• Intratumoral and peritumoral 3 mm Radscore showed the most capability for predicting ENE.
• Clinical-radiomics nomogram achieved the best predictive performance for predicting ENE.
• Combining clinical-radiomics based-ENE and EMVI showed good performance for 3-year RFS.
Graphical Abstract

Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Colorectal cancer ranks as the second most common cause of cancer mortality in the world [1]. Although most patients with resectable rectal cancer undergo curative resection, distant recurrence is the main cause of rectal cancer death [2]. Therefore, it is important to accurately assess risk factors for recurrence to improve survival. Extranodal extension (ENE) is the breakthrough growth of tumor cells from within the lymph node (LN) capsule into the surrounding perinodal adipose tissues [3]. Given this, ENE is known to be of important prognostic value in a variety of malignant tumors [4,5,6,7]. ENE has been recently incorporated into LN staging in neck cancer [8]. In rectal cancer, several previous studies indicated that ENE was an adverse factor for recurrence-free survival (RFS) [9,10,11]. Moreover, the panel agrees that radiologists should no longer consider the mesorectal fascia as involved when potentially malignant smooth enlarged lymph nodes (i.e., with an apparently intact capsule) contact the mesorectal fascia [12]. Therefore, these studies suggest that the preoperative prediction of ENE is an important parameter in reflecting the risk of recurrence and determining adjuvant treatment strategies [9,10,11].
Traditional imaging methods that depend on qualitative evaluation alone cannot reliably identify ENE in neck cancer, with an area under the receiver operating characteristic (ROC) curve (AUC) of 0.621–0.700 [13, 14]. Moreover, the size of node metastasis in head and neck squamous cell carcinoma is usually larger than that in rectal cancer [15]. Therefore, we hypothesized that the preoperative evaluation of ENE in patients with rectal cancer using qualitative evaluation alone was also not reliable. At present, no study has been performed to assess ENE in patients with rectal cancer using a method based on radiomics. Previous studies showed that the MRI-based radiomics signature score (Radscore) of the primary tumor could be used to identify lymph node metastasis (LNM) and tumor deposits in rectal cancer [16, 17]. However, most of these studies only focused on intratumoral regions, while peritumoral regions, which may have important information about the tumor, were excluded [18,19,20]. Heterogeneity exists not only in cancer cells but also in nonmalignant cells and infiltrating cells around the tumor, usually referred to as the peritumoral microenvironment [21]. Tumor evolution and progression are influenced by the interaction between cancer cells and the peritumoral microenvironment [22]. To our knowledge, no study has been performed to investigate the relationships between preoperative MRI-Radscore-based ENE and 3-year RFS. The Radscore from T2-weighted imaging (T2WI) of the primary tumor alone has been reported to be useful for predicting the response to chemoradiotherapy in rectal cancer [23]. Therefore, the primary aim of this study was to develop and validate a radiomics approach for the preoperative prediction of ENE based on intratumoral and peritumoral tissue on T2WI images in patients with rectal cancer undergoing radical resection. The secondary aim was to evaluate whether this predictive model-based ENE was associated with 3-year RFS in patients with rectal cancer.
Materials and methods
Patients
This prospective study was approved by the institutional review board of our hospital, and written informed consent was obtained from all patients. The study complied with the Declaration of Helsinki.
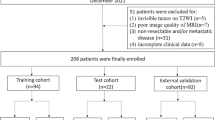
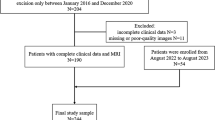
From January 2019 to January 2022, 202 patients with rectal cancer deemed resectable based on the results of preoperative MRI were enrolled. Total mesorectal excision was performed in all patients. The inclusion criteria were as follows: (1) patients who received radical surgery without preoperative adjuvant therapy, (2) rectal cancer and LN status confirmed by pathological results, and (3) complete high-resolution rectal MRI examination data recorded 2 weeks before surgery. The exclusion criteria were as follows: (1) tumor invisible on T2WI images (n = 4); (2) poor MRI image quality (n = 6); (3) nonresectable tumor and/or metastatic disease (cM1 or pM1) (n = 21); and (4) incomplete clinical data (n = 4). Ultimately, 167 patients were included in this study. Among the 167 patients, there were 60 patients without lymph node metastasis (LNM), 29 patients with 1 LNM, 47 patients with 2–3 LNMs, 22 patients with 4–6 LNMs, and 9 patients with 7 or more LNMs. According to the eighth edition American Joint Committee on Cancer (AJCC) rectal cancer staging system [8], there were 60 patients at stage pN0, 29 patients at stage pN1a, 47 patients at stage pN1b, 22 patients at stage pN2a, and 9 patients at stage pN2b. Baseline characteristics of the patients, including carbohydrate antigen 199 (CA199), carcinoembryonic antigen (CEA), sex, and tumor location, were also recorded. There were 117 patients in the training cohort and 50 patients in the validation cohort. A flowchart of the study participants is described in Fig. 1.

Flowchart of patient selection
Imaging protocol
MRI was performed on a 1.5-T MR scanner (MAGNETOM Aera, Siemens Healthineers). Scopolamine butylbromide (20 mg) (Buscopan, Boehringer Ingelheim) was intramuscularly injected to inhibit bowel motion 10 min before the MRI examination. Water or air was not given to dilate the rectum. Axial T2WI without fat saturation was performed, and the scanning direction was oriented perpendicular to the long axis of the rectum. The following parameters were used: TR, 4600; TE, 75; field of view (FOV), 220 mm2; matrix size, 256 × 512; and 3 mm thickness with no interslice gap. Diffusion-weighted imaging parameters were as follows: TR, 4600; TE, 59; number of signals acquired, eight; FOV, 360 mm2; 5 mm section thickness; and b = 0, 800 s/mm2.
Qualitative image evaluation
Two radiologists (with 5 and 12 years of experience in rectal cancer) who were blinded to the clinical information reviewed the MR images in 167 patients with rectal cancer. Radiologic ENE was considered positive when at least one of the following criteria was met: (1) irregular LN border and (2) invasion of the adjacent fat [13]. Additionally, we assessed whether the internal intensity of LN was heterogeneous and whether the chemical shift effect (CSE) along the margin of LN was absent [24]. Tumor cells inside the subcapsular sinus that break through the LN capsule may influence the uniform fat-water interface and thus destroy the normal CSE. If the LN capsule is broken by the tumor cell, the normal chemical shift effect in this region will disappear. The heterogeneous intensity of the LN indicates that the normal LN structure is replaced by tumor cells, and the low-intensity signal of the LN capsule on T2WI will disappear. Radiologic ENE status was compared with the nodal histopathology results (Fig. S1). For a node-to-node comparison, the following morphological features were recorded: LN size and the location related to the tumor, mesorectal fascia, and vessels. If the LNs on MRI did not match the histopathological results, these LNs were excluded. Finally, the pathological findings determine whether LNM and ENE are positive or negative. The LN yield at pathology per patient was more than 12. The extramural vascular invasion (EMVI) status of the primary tumor and T stage were also evaluated on MRI [25]. Moreover, the tumor length and maximal tumor thickness were obtained on the sagittal and oblique T2WI images, respectively.
Tumor segmentation
The tumor segmentation process on MRI is shown in Fig. 2. Tumor delineation was performed on the entire three-dimensional tumor volume on T2WI images by a radiologist (the first author) using AK software (Artificial Intelligence Kit, version 3.3.0, GE Healthcare). For the segmentation of peritumoral regions, a peritumoral 3 mm region was obtained with automated dilation of the tumor boundaries by 2 mm on the outside and shrinkage of the tumor boundaries by 1 mm on the inside, resulting in a ring with a thickness of 3 mm [26]. The peritumoral-mesorectal fat (MRF) region was obtained by drawing along the mesorectal fascia. Thirty patients’ data were randomly selected for assessing interobserver and intraobserver agreement of feature extraction by intraclass correlation coefficient (ICC) analysis. First, a radiologist delineated the tumor volume of interest on T2WI images and repeated this process after 3 weeks to calculate the intraobserver ICC. Two radiologists independently delineated the tumor volume of interest on T2WI images, and the interobserver ICC was calculated. Only radiomics features demonstrating an ICC greater than 0.75 were retained for further analysis.

Tumor segmentation process on MRI. First, we manually segmented the whole tumor on axial T2WI images and labeled it as the intratumoral area. Second, “shrink” was defined as the tumor border automatically shrinking by 1 mm on the inside. “Dilate” was defined as automated dilation of the tumor border by 2 mm on the outside. “Dilate-shrink” resulted in a ring with a thickness of 3 mm. Thus, the peritumoral 3 mm area was obtained, including the most peripheral portion of the tumor and the surrounding tissues. Moreover, the peritumoral-mesorectal fat (MRF) area was obtained by drawing along the mesorectal fascia
Feature extraction, selection, and model building
The radiomics module (backed by PyRadiomics) was used to extract radiomics features. Voxel size was resampled by 1 × 1 × 1 mm, and z score normalization of the signal intensities for T2WI images was performed using PyRadiomics [27]. In total, 1316 radiomics features, including 252 histogram features, 14 shape features, 336 Gy level co-occurrence matrix, 224 Gy level size zone matrix, 224 Gy level run length matrix, 196 Gy level dependence matrix, and 70 neighboring gray-tone difference matrix, were obtained from each patient. The statistical software R (version 3.5.1, 2019, The R Foundation for Statistical Computing, Vienna, Austria) was used to select radiomics features and build the model. The maximum relevance and minimum redundancy were first performed to select radiomics features [28]. The optimized subset of features was obtained using the least absolute shrinkage and selection operator in the training cohort [29]. Subsequently, a linear combination of the selected features weighted by their respective coefficients was used to calculate the Radscore for each patient. The diagnostic performance of the Radscore in the training cohort and validation cohort was evaluated using AUC. The most predictive Radscore was selected for the subsequent analysis.
The nomogram was constructed by univariate and multivariate logistic regression analyses. ROC curves were generated to assess the discriminatory ability in the training cohort and validation cohort. A calibration curve was generated to calibrate the nomogram. Decision curve analysis (DCA) was applied to investigate the clinical utility of the models.
Outcome
For patients with postoperative T1-2N0M0 rectal cancer, only the “follow-up watch” strategy was used. Patients with postoperative T3a/bN0M0, T4aN0M0, or T1-4aN1-2M0 rectal cancer received 5-fluorouracil-based adjuvant therapy after surgery. Locoregional recurrence or distant metastasis after surgery was evaluated every 3–6 months based on digital rectal examination and endoscopic examination plus CT, MRI, and/or PET/CT to determine relapse. The primary endpoint was a 3-year RFS.
Statistical analysis
Statistical analyses were performed using SPSS (version 23.0) and R software (version 3.5.1). An interreader agreement was conducted for the assessment results of ENE by the two radiologists using the kappa value. The relationship between clinical baseline characteristics and ENE status was evaluated by the chi-squared test, independent two-sample t test, and Fisher’s exact test (where appropriate). The “mRMR” algorithm in the “mRMRe” package was used to conduct the maximum relevant minimum redundancy to initially screen the radiomics features. The best feature cohort was selected by the “glmnet” algorithm in the “glmnet” package. ROC analysis was carried out based on the “pROC” package to evaluate the effectiveness. The “calibrate” function in the “rms” package was applied to calibration curve plots and builds nomograms, and decision curves were plotted based on the “rmda” package in both clinical and combined models. The differences in AUCs between the models were compared using Delong’s test. Kaplan–Meier analysis with the log-rank test was used for survival analysis. Univariate and multivariate Cox regression analyses were used to construct a prognostic model for assessing 3-year RFS. The diagnostic performance of this prognostic model was determined using time-dependent ROC curves.
Results
Patient characteristics
Among the 167 patients (mean age, 62 years; range 29–88 years), 117 patients were in the training cohort (43 ENE + and 74 ENE-), and 50 patients were in the validation cohort (8 ENE + and 42 ENE-). There was a significant difference in pathological ENE between the two cohorts (p = 0.008), but no significant differences were found in CA199, CEA, tumor length, wall thickness, age, sex, location, cT stage, pathological LN, MRI-reported EMVI, LN-irregular border and/or adjacent fat invasion, LN-CSE, and LN-heterogeneous intensity between the two cohorts (all p > 0.05) (Table 1).
MR-reported ENE correlation with pathologic results
The correlation of MR-reported ENE and pathologic results is shown in Table S1.
Pathologically confirmed ENE positivity was observed in 51 patients, with an MR-reported ENE positivity in 27 patients for reader 1 and 26 patients for reader 2. Pathologically confirmed ENE negativity was observed in 117 patients, with an MR-reported ENE negativity in 83 patients for reader 1 and 81 patients for reader 2. The interreader agreement between the two radiologists for assessing ENE was good, with a kappa value of 0.780 (95% CI = 0.671–0.874). The correlation of MR-reported ENE with pathologic findings was confirmed with kappa, sensitivity, and specificity values of 0.233, 52.9%, and 71.5%, respectively. Therefore, the association of MR-reported ENE with pathologic findings showed poor consistency.
Feature selection, development, and validation of prediction models
The final formula of the Radscore used to predict ENE is shown in Table S2. Combining intratumoral and peritumoral 3 mm Radscore resulted in the highest capability for predicting ENE, with AUCs of 0.707 and 0.667 in the training cohort and validation cohort, respectively (Fig. 3). A nomogram was constructed by adding the combined intratumoral and peritumoral 3 mm Radscore (odds ratio (OR) = 2.89) to the clinical model (age (OR = 0.95), cT stage (OR = 1.98), and LN-irregular border and/or adjacent fat invasion (OR = 3.36)) as summarized in Table 2. Compared with the clinical model, the nomogram (cutoff, -0.405) provided a slightly higher AUC in the training cohort (0.799 vs. 0.736, p = 0.072) and validation cohort (0.723 vs. 0.667, p = 0.4) (Tables 3 and 4; Fig. 4). For the nomogram, good agreement between the predicted probability and actual observed probability was demonstrated by the calibration curve. The result of the decision curve indicated that the nomogram had more benefits than the other models for predicting ENE when the threshold probability ranged from 0.18 to 0.73 in the training cohort and from 0.10 to 0.74 in the validation cohort (Fig. 5).

Receiver operating characteristic curves of intratumoral radiomics score (red line), intratumoral&peritumoral-MRF radiomics score (blue line), intratumoral and peritumoral-3-mm radiomics score (green line), peritumoral-3mm radiomics score (purple line), and peritumoral-MRF radiomics score (black line) for predicting extranodal extension in the training cohort (A) and validation cohort (B)

The performance and validation of the final selected model to predict extranodal extension (ENE). ROC of clinical model (red line), intratumoral and peritumoral-3-mm radiomics model (blue line), and nomogram (green line) for predicting ENE in the training cohort (A) and validation cohort (B). C The predictive nomogram of ENE

Fit and usefulness evaluation of the clinical-radiomics nomogram. Calibration curve of the clinical-radiomics nomogram for predicting extranodal extension (ENE) in the training cohort (red line) and validation cohort (blue line) (A); decision curve analysis (DCA) of the nomogram for assessing its clinical usefulness; this indicates that a nomogram to predict ENE gains more benefit than the “treat all,” “treat none,” radiomics model and the clinical model when the threshold probability ranges from 0.18 to 0.73 in the training cohort (B) and from 0.10 to 0.74 in the validation cohort (C)
Subgroup analyses
Subgroup analyses of the three models are shown in Fig. S2 and Table S3. There were 3 ENE + patients and 26 ENE- patients at the T1-T2 stage. For differentiating ENE + from ENE- patients at the T1-T2 stage, both the clinical model and the nomogram had similar AUCs, which were slightly higher than that of the radiomics model (0.705 vs. 0.660, p = 0.076, i.e., not statistically significant). There were 48 ENE + patients and 90 ENE-patients at the T3a/b-T4a stage. For differentiating ENE + from ENE- patients at the T3a/b-T4a stage, the nomogram showed better AUCs than the clinical model (0.725 vs. 0.656, p = 0.041) and slightly higher AUCs than the radiomics model (0.725 vs. 0.697, p = 0.085, i.e., not statistically significant).
Survival analysis
The median follow-up of the event-free patients was 24 months (range, 6–36 months) and 22 months (range, 7–36 months) in the training cohort and validation cohort, respectively. The 51 patients with ENE had a higher rate of recurrence than the 116 patients without ENE (43.1% vs. 18.9%). In the training cohort, there were 35 patients (35/117, 29.9%) with locoregional or distant relapse after a median duration of 10 months (3–36 months). In the validation cohort, there were 9 patients (9/50, 18%) with locoregional or distant relapse after a median duration of 8 months (4–29 months). As shown in Kaplan–Meier survival curves (Fig. 6), patients with low clinical-radiomics nomogram score-based ENE- (≤ -0.405) showed better 3-year RFS than those with high score-based ENE + (> -0.405).

Kaplan–Meier survival curves of the nomogram-based extranodal extension (ENE) for 3-year recurrence-free survival in patients with rectal cancer in the entire cohort (A), at T1-T2 stage (B), and T3a/b-T4a stage (C)
Univariate and multivariate Cox analyses showed that EMVI (hazard ratio [HR] = 2.523, 95% CI = 1.247–5.106, p = 0.010) and clinical-radiomics nomogram-based ENE (HR = 2.625, 95% CI = 1.233–5.586, p = 0.012) were independent risk factors for 3-year RFS (Table 5). EMVI and clinical-radiomics nomogram-based ENE assessments were performed to construct the prognostic model for 3-year RFS and indicated good performance, with AUCs of 0.761 in the training cohort and 0.710 in the validation cohort.
Discussion
From several studies, scholars have reported that intratumoral radiomics signatures could predict LNM and tumor deposits in rectal cancer [17, 30, 31]. In this study, we also assessed ENE with radiomic signatures from the primary tumor, instead of lymph nodes. The explanation could be that it was sometimes difficult to completely maintain the node-to-node correspondence between surgical histology and MR-identified nodes. Moreover, small LNs (e.g., < 5 mm) may have positive ENE, but were very difficult for the radiologist to draw ROI on given their small size. Even though small lymph nodes could be identified by the radiologist, drawing the entire lymph node on MR images with a slice thickness of 3 mm was also difficult. Since the risk of metastases is fundamentally driven by the primary tumor, we can hypothesize that radiomics analysis of the primary tumor may help identify the status of ENE. We found that T2WI-based radiomics from the intratumoral region could predict ENE with an AUC of 0.612. Jin et al. and Chen et al. reported that radiomics features obtained from intratumoral and peritumoral fat were used to construct a model for predicting tumor deposits [16, 32]. These studies found that the combined model incorporating intratumoral and peritumoral fat and clinical factors provided good performance for predicting tumor deposits. However, the radiomic features in these studies were extracted from ultrasound or CT images, which were not the best examination modality for rectal cancer. Jayaprakasam et al. reported that MRI radiomics features from MRF showed good performance for predicting tumor recurrence and response to neoadjuvant chemoradiation therapy in rectal cancer [33]. A recent study also showed that combining intratumoral and MRF radiomics models provided better performance than a single intratumoral radiomics model for predicting tumor deposits [34]. These studies defined the peritumoral region by drawing along the mesorectal fascia. However, some studies have defined the peritumoral region as the area immediately surrounding the tumor [20, 26, 35,36,37]. Therefore, it is uncertain whether we should combine intratumoral and MRF radiomics features or intratumoral and peritumoral regions immediately surrounding the tumor. In this study, we compared different regional Radscores and found that the combined intratumoral and peritumoral 3 mm Radscore achieved the highest capability for predicting ENE, with an AUC of 0.723. For radiomics features from the intratumoral region, the negative coefficient (-0.592) of Zone Percentage indicated a coarser texture, implying notable tumor heterogeneity. For peritumoral 3 mm radiomics features, the positive coefficient of gray-level variance indicating the variance in gray-level intensity for the runs implies tumor heterogeneity. For peritumoral-MRF radiomics features, the positive coefficient of short-run high gray-level emphasis and IDN imply homogeneous textures [38]. These findings may suggest that the peritumoral region far from the tumor contains less information than the region immediately surrounding the tumor. The probable interpretation could be related to the peritumoral immune microenvironment, which was mainly in the region immediately adjacent to the tumor [39]. Moreover, in a previous study, it was reported that tumor cells were separated from the infiltrating edge of the tumor and migrated to the surrounding stroma, indicating that tumor-budding cell clusters mainly existed at the edge of the tumor [40]. These findings may indicate that the region adjacent to the tumor plays an important role in metastatic LN.
To our knowledge, no studies have used clinical factors to select noninvasive independent predictors of ENE. We found that age, cT-stage, and LN-irregular border and/or invasion of the adjacent fat on MRI were independent predictors for ENE. Heterogeneous LN intensity and disappearance of the CSE were not independent risk factors for ENE. The most likely explanation is that heterogeneous intensity in LNs and the disappearance of LN-CSE are not unique to ENE, which can be seen in most metastatic LNs. Moreover, tumor cells inside the subcapsular sinus that do not break through the LN capsule may also influence the uniform fat-water interface and thus destroy the normal chemical shift effect [23]. In this study, LN-irregular border and/or adjacent fat invasion on MRI was considered a morphological feature for assessing ENE. We found that the correlations of LN-irregular border and/or adjacent fat invasion with pathologic findings were validated with kappa, sensitivity, and specificity values of 0.233, 52.9%, and 71.5%, respectively. The explanation could be that it was sometimes difficult to assess the border status of small nodes because of the restriction of spatial resolution. Moreover, there is a limitation for current imaging modalities to accurately identify microscopic ENE [41, 42]. Therefore, we may conclude that it was difficult to assess ENE using morphological features on MRI. Our findings indicated that adding the combined intratumoral and peritumoral 3 mm Radscore to the clinical model could improve the benefit compared with the clinical model alone for the assessment of ENE. However, there was no statistical significance for AUC between the clinical model and the nomogram. A possible explanation could be the small sample size of patients and lower incidence of ENE + in this study. Moreover, the proportions of patients with and without ENE greatly differed between the training cohort and the validation cohort. Therefore, further studies with larger sample sizes should be performed to confirm our findings.
For the subgroup analyses, our results showed that both the clinical model and clinical-radiomics nomogram had similar AUCs of 0.705 for differentiating ENE + from ENE- patients at the T1-T2 stage. The explanation could be that the incidence of ENE + is low (10.3%, 3/29) at the T1-T2 stage. For differentiating ENE + from ENE- patients at the T3a/b-T4a stage, the clinical-radiomics nomogram performed significantly better than the clinical model (AUC, 0.725 vs. 0.656). The explanation could be that the incidence of ENE + is high (34.8%, 48/138) at the T3a/b-T4a stage. Moreover, greater heterogeneity exists in T3a/b-T4a stage rectal cancers than in T1-T2 stage cancers, and these features cause substantial differences in radiomic features [43]. Therefore, combining these radiomics features with clinical risk factors may lead to a better prediction of ENE than the clinical model alone. These results may indicate that the clinical-radiomics nomogram can predict ENE stratified by tumor T staging. In addition, patients with ENE had a higher rate of recurrence than patients without ENE (51.9% vs. 8.3%). Our study showed that patients with low clinical-radiomics combined model score-based ENE had better 3-year RFS than patients with high scores. Multivariate Cox analysis showed that clinical-radiomics nomogram-based ENE in addition to MRI-reported EMVI were independent risk factors for predicting 3-year RFS. A previous study also confirmed that MRI-reported EMVI was strongly associated with distant recurrence [44]. Our findings may lead to the conclusion that T stage and N stage are not sufficient for classifying the patient, and it may be more sensible to include additional indicators, such as in the clinical-radiomics nomogram-based ENE and EMVI.
There are some limitations in this study. Firstly, due to the low incidence of ENE, the sample size of patients with ENE enrolled in this study was small. To prevent the model from being affected by data bias during the training process, relatively more positive samples were randomly allocated to the training set data to ensure that the ratio of ENE negative and positive in the training set data was within the range of 2:1. Although this allocation scheme would make the proportion of patients with ENE negative and positive very different in the validation cohort, the incidence rate of ENE was approximately 22% [45], which would not affect practical clinical applications. Secondly, this is a single-center study, and the model will need to be confirmed with external validation data. Thirdly, this study only included T2WI-based radiomics analysis. Other MRI sequences, such as DWI, were excluded. Fourthly, although we endeavored to keep the LNs on preoperative images matched with histopathologic results, it was sometimes difficult to completely maintain the node-to-node correspondence. However, clinicians generally focus only on the presence or absence of ENE in patients with rectal cancer. Therefore, in this study, the analysis was performed on a per-patient basis for ENE rather than on a per-node basis. Finally, patients with T3a/b-T4a or N + rectal cancer did not receive preoperative chemoradiotherapy. In this study, we found that the 3-year RFS rate was 73.5%, which did not differ when compared with standard therapy of preoperative chemoradiotherapy, surgery, and postoperative adjuvant chemotherapy with 3-year RFS rate of 75% [46]. This finding seems to indicate that preoperative chemoradiotherapy has not been shown to significantly increase the 3-year RFS rate compared with surgery alone [47].
In summary, our study provides a clinical-radiomics nomogram that combines intratumoral and peritumoral 3 mm Radscore, age, cT stage, and LN-irregular border and/or adjacent fat invasion for the preoperative prediction of ENE. Combining this nomogram-based ENE prediction with EMVI could help identify patients at high risk for recurrence and promote personalized treatment.
Availability of data and materials
The datasets generated during and analyzed during the current study are not publicly available due to PACS system regulated by Sichuan Provincial People’s Hospital but are available from the corresponding author upon reasonable request.
Abbreviations
- AJCC:
-
American Joint Committee on Cancer
- AUC:
-
Areas under the receiver operating characteristic curve
- CA199:
-
Carbohydrate antigen 199
- CEA:
-
Carcinoembryonic antigen
- CI:
-
Confidence interval
- CSE:
-
Chemical shift effect
- DCA:
-
Decision curve analysis
- EMVI:
-
Extramural vascular invasion
- ENE:
-
Extranodal extension
- FOV:
-
Field of view
- HR:
-
Hazard ratio
- ICC:
-
Intraclass correlation coefficient
- LN:
-
Lymph node
- LNM:
-
Lymph node metastasis
- MRF:
-
Mesorectal fat
- OR:
-
Odds ratio
- RFS:
-
Recurrence-free survival
- ROC:
-
Receiver operating characteristic
- T2WI:
-
T2-weighted images
References
Sung H, Ferlay J, Siegel RL et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 Cancers in 185 countries. CA Cancer J Clin 71:209–249
Siegel RL, Miller KD, Goding Sauer A et al (2020) Colorectal cancer statistics. CA Cancer J Clin 70:145–164
Bhattacharya P, Mukherjee R (2021) Lymph node extracapsular extension as a marker of aggressive phenotype: classification, prognosis and associated molecular biomarkers. Eur J Surg Oncol 47:721–731
Wind J, Lagarde SM, Ten Kate FJ et al (2007) A systematic review on the significance of extracapsular lymph node involvement in gastrointestinal malignancies. Eur J Surg Oncol 33:401–408
Alakus H, Hölscher AH, Grass G et al (2010) Extracapsular lymph node spread: a new prognostic factor in gastric cancer. Cancer 116:309–315
Lagarde SM, ten Kate FJ, de Boer DJ et al (2009) Extracapsular lymph node involvement differs between squamous cell and adenocarcinoma of the esophagus. Ann Surg Oncol 16:447–453
Ahn TS, Kim HS, Jeong CW et al (2015) Extracapsular extension of pelvic lymph node metastasis is an independent prognostic factor in bladder cancer: a systematic review and meta-analysis. Ann Surg Oncol 22:3745–3750
Amin MB, Edge SB, Greene FL et al (2017) AJCC Cancer staging manual, 8th edn. Springer, New York
Kim YL, Cho H, Kim CW et al (2021) Prognostic impact of extranodal extension in rectal cancer patients undergoing radical resection after preoperative chemoradiotherapy. Clin Colorectal Cancer 20:e35–e42
Veronese N, Nottegar A, Pea A et al (2016) Prognostic impact and implications of extracapsular lymph node involvement in colorectal cancer: a systematic review with meta-analysis. Ann Oncol 27:42–48
Yamano T, Semba S, Noda M et al (2015) Prognostic significance of classified extramural tumor deposits and extracapsular lymph node invasion in T3–4 colorectal cancer: a retrospective single-center study. BMC Cancer 15:859
Lambregts DMJ, Bogveradze N, Blomqvist LK et al (2022) Current controversies in TNM for the radiological staging of rectal cancer and how to deal with them: results of a global online survey and multidisciplinary expert consensus. Eur Radiol 32:4991–5003
Lee B, Choi YJ, Kim SO et al (2019) Prognostic value of radiologic extranodal extension in human papillomavirus-related oropharyngeal squamous cell carcinoma. Korean J Radiol 20:1266–1274
Chai RL, Rath TJ, Johnson JT et al (2013) Accuracy of computed tomography in the prediction of extracapsular spread of lymph node metastases in squamous cell carcinoma of the head and neck. JAMA Otolaryngol Head Neck Surg 139:1187–1194
Som PM (1992) Detection of metastasis in cervical lymph nodes: CT and MR criteria and differential diagnosis. AJR Am J Roentgenol 158:961–969
Chen LD, Li W, Xian MF et al (2020) Preoperative prediction of tumour deposits in rectal cancer by an artificial neural network-based US radiomics model. Eur Radiol 30:1969–1979
Yang YS, Feng F, Qiu YJ, Zheng GH, Ge YQ, Wang YT (2021) High-resolution MRI-based radiomics analysis to predict lymph node metastasis and tumor deposits respectively in rectal cancer. Abdom Radiol (NY) 46:873–884
Yuan Y, Chen XL, Li ZL et al (2022) The application of apparent diffusion coefficients derived from intratumoral and peritumoral zones for assessing pathologic prognostic factors in rectal cancer. Eur Radiol 32:5106–5118
Hu Y, Xie C, Yang H et al (2020) Assessment of intratumoral and peritumoral computed tomography radiomics for predicting pathological complete response to neoadjuvant chemoradiation in patients with esophageal squamous cell carcinoma. JAMA Netw Open 3:e2015927
Orel VE, Ashykhmin A, Golovko T, Rykhalskyi O, Orel VB (2021) Texture analysis of tumor and peritumoral tissues based on 18F-fluorodeoxyglucose positron emission tomography/computed tomography hybrid imaging in patients with rectal cancer. J Comput Assist Tomogr 45:820–828
Conti G, Calderan L, Sierra LAQ et al (2023) (2023) Tumor and peritumoral adipose tissue crosstalk: de-differentiated adipocytes influence spread of colon carcinoma cells. Tissue Cell 80:101990
Nelson DA, Tan TT, Rabson AB, Anderson D, Degenhardt K, White E (2004) Hypoxia and defective apoptosis drive genomic instability and tumorigenesis. Genes Dev 18:2095–2107
Shin J, Seo N, Baek SE et al (2022) MRI radiomics model predicts pathologic complete response of rectal cancer following chemoradiotherapy. Radiology 303:351–358
Zhang HM, Zhang CD, Zheng ZX et al (2017) Chemical shift effect predicting lymph node status in rectal cancer using high-resolution MR imaging with node-for-node matched histopathological validation. Eur Radiol 27:3845–3855
Smith NJ, Shihab O, Arnaout A, Swift RI, Brown G (2008) MRI for detection of extramural vascular invasion in rectal cancer. AJR Am J Roentgenol 191:1517–1522
Jiang Y, Wang H, Wu J et al (2020) Noninvasive imaging evaluation of tumor immune microenvironment to predict outcomes in gastric cancer. Ann Oncol 31:760–768
van Griethuysen JJM, Fedorov A, Parmar C et al (2017) Computational radiomics system to decode the radiographic phenotype. Cancer Res 77:e104–e107
Zhao Z, Anand R, Wang M (2019) IEEE International Conference on Data Science and Advanced Analytics (DSAA). IEEE, Washington, DC
Sauerbrei W, Royston P, Binder H (2007) Selection of important variables and determination of functional form for continuous predictors in multivariable model building. Stat Med 26:5512–5528
Li CL, Yin JD (2021) Radiomics based on T2-weighted imaging and apparent diffusion coefficient images for preoperative evaluation of lymph node metastasis in rectal cancer patients. Front Oncol 11:671354
Huang YQ, Liang CH, He L et al (2016) Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J Clin Oncol 34:2157–2164
Jin YM, Li M, Zhao YL et al (2021) Computed tomography-based radiomics for preoperative prediction of tumor deposits in rectal cancer. Front Oncol 11:710248
Jayaprakasam VS, Paroder V, Gibbs P et al (2022) MRI radiomics features of mesorectal fat can predict response to neoadjuvant chemoradiation therapy and tumor recurrence in patients with locally advanced rectal cancer. Eur Radiol 32:971–980
Feng FW, Liu YQ, Bao JY, Hong R, Hu S, Hu CH (2023) Multiregional-based magnetic resonance imaging radiomics model for predicting tumor deposits in resectable rectal cancer. Abdom Radiol (NY). https://doi.org/10.1007/s00261-023-04013-w
Pizzi AD, Chiarelli AM, Chiacchiaretta P et al (2021) MRI-based clinical-radiomics model predicts tumor response before treatment in locally advanced rectal cancer. Sci Rep 11:5379
Shi JX, Dong Y, Jiang WY et al (2022) MRI-based peritumoral radiomics analysis for preoperative prediction of lymph node metastasis in early-stage cervical cancer: a multi-center study. Magn Reson Imaging 88:1–8
Yu Y, Tan Y, Xie C et al (2020) Development and validation of a preoperative magnetic resonance imaging radiomics-based signature to predict axillary lymph node metastasis and disease-free survival in patients with early-stage breast cancer. JAMA Netw Open 3:e2028086
Zwanenburg A, Lege S, Vallières M, Löck S (2016) Image biomarker standardisation initiative - feature definitions. In eprint arXiv:1612.07003
Sun R, Limkin EJ, Vakalopoulou M et al (2018) A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: an imaging biomarker, retrospective multicohort study. Lancet Oncol 19:1180–1191
Dawson H, Galuppini F, Träger P et al (2019) Validation of the international tumor budding consensus conference 2016 recommendations on tumor budding in stage I-IV colorectal cancer. Hum Pathol 85:145–151
Prabhu RS, Magliocca KR, Hanasoge S et al (2014) Accuracy of computed tomography for predicting pathologic nodal extracapsular extension in patients with head-and-neck cancer undergoing initial surgical resection. Int J Radiat Oncol Biol Phys 88:122–129
Geltzeiler M, Clayburgh D, Gleysteen J et al (2017) Predictors of extracapsular extension in HPV-associated oropharyngeal cancer treated surgically. Oral Oncol 65:89–93
Sun Y, Hu P, Wang J et al (2018) Radiomic features of pretreatment MRI could identify T stage in patients with rectal cancer: preliminary findings. J Magn Reson Imaging. https://doi.org/10.1002/jmri.25969
Lord AC, D’Souza N, Shaw A et al (2022) MRI-diagnosed tumor deposits and EMVI status have superior prognostic accuracy to current clinical TNM staging in rectal cancer. Ann Surg 276:334–344
Heide J, Krüll A, Berger J (2004) Extracapsular spread of nodal metastasis as a prognostic factor in rectal cancer. Int J Radiat Oncol Biol Phys 58:773–778
Garcia-Aguilar J, Patil S, Gollub MJ et al (2022) Organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. J Clin Oncol 40:2546–2556
Akagi T, Inomata M, Fujishima H et al (2020) Preoperative chemoradiotherapy versus surgery alone for advanced low rectal cancer: a large multicenter cohort study in Japan. Surg Today 50:1507–1514
Funding
This study has received funding from the Key Research Project of Sichuan Province (grant number, 2022YFS0249).
Author information
Authors and Affiliations
Contributions
Conception and design were carried out by TL; administrative support was carried out by HL and LC; study materials were carried out by HL and HP; collection of data was carried out by ML, LY, and YL; statistics analysis was carried out by XZ and MP; manuscript writing was carried out by all authors; and the final manuscript has been approved by all authors. HL and LC contributed equally to this work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This prospective study was approved by the institutional review board of Sichuan Provincial People’s Hospital and written informed consent was obtained from all included.
Consent for publication
Not applicable.
Competing interests
XZ is an employee of GE Healthcare. The remaining authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Representative examples of evaluating extranodal extension (ENE) on T2WI and histopathology. Figure S2. Receiver operating characteristic curves of intratumoral & peritumoral-3 mm radiomics model, clinical model, and the clinical-radiomics nomogram for identifying extranodal extension at T1-T2 stage (A) and T3a/b-T4a stage (B) of rectal cancer. Table S1. The correlation between MR-reported extranodal extension (ENE) and pathological results. Table S2. Radiomics features score (radscore) formula of different models for predicting extranodal extension. Table S3. Subgroup analysis of the radiomics model, clinical model, and the clinical-radiomic nomogram.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, H., Chai, L., Pu, H. et al. T2WI-based MRI radiomics for the prediction of preoperative extranodal extension and prognosis in resectable rectal cancer. Insights Imaging 15, 57 (2024). https://doi.org/10.1186/s13244-024-01625-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-024-01625-8