
Abstract
Background
Inguinal endometriosis is one of the most common forms of endometriosis. The present study introduces 8 cases of inguinal endometriosis and discusses probable theories of inguinal endometriosis by reviewing the literature.
Case presentation
8 Iranian cases of inguinal endometriosis with a mean age of 36 years were presented. Catamenial groin pain and swelling were the most common complications. Also, patients usually had accompanying symptoms such as pelvic pain and dysmenorrhea. One-half of patients had a history of previous abdominal surgery. Ultrasound was diagnostic in 4 patients (50%), and magnetic resonance imaging was used in two patients (25%). Among 6 patients who underwent hormonal therapy, 4 experienced an endometriosis size increase. Inguinal endometriosis was right-sided in 87.5% of patients, and among 4 patients who underwent surgery, 75% had proximal site involvement of the round ligament.
Conclusion
According to the rarity of inguinal endometriosis, it is more likely to be a misdiagnosis with other inguinal disorders such as inguinal hernia. Inguinal endometriosis should be considered in patients who undergo inguinal herniorrhaphy, with suspected findings such as thickening of the hernia sac wall, bloody fluid inside the sac, or thickening of the extraperitoneal round ligament during the surgery.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Endometriosis is a common gynecological disorder among women of reproductive age with about 10 to 15% prevalence [1, 2]. Ovaries are the most common site of endometriosis, although it can be identified in unconventional sites, such as the inguinal region, which accounts for 0.3–0.6% of all endometriosis [3,4,5]. 133 cases of inguinal endometriosis (IEM) have been reported until 2022 in the literature [6]. However, many inguinal IEM patients are not diagnosed because they undergo herniorrhaphy by general surgeons without any consideration for endometriosis [7]. IEM can co-exist with other groin disorders, such as inguinal hernia [8]. So, IEM is divided into three types: 1, IEM of inguinal hernia sac or hydrocele of canal of Nuck; 2, round ligament IEM; and 3, superficial IEM [9]. IEM’s diagnosis is challenging according to the wide range of differential diagnoses, such as inguinal hernia, inguinal lymphadenopathy, etc., so it can be misdiagnosed with other inguinal disorders commonly [10]. Female individuals with groin swelling or pain with menstruation-associated exacerbation (catamenial symptoms) should be assessed for IEM [6]. Although, a definitive diagnosis of IEM is usually made through histopathological examination [5]. Surgical resection is the standard treatment of IEM; nevertheless, the role of medical therapy is still controversial [10]. This study presents 8 cases of IEM who presented to the author’s office from 2017 to 2022. Also, it discusses probable theories of IEM by reviewing the literature.
Case presentation
Patient’s characteristics and symptoms
Eight Iranian cases of IEM, as well as one case of inguinal hernia with superficial implantations of the endometriosis surrounding the entrance of the hernia sac, were included1. The mean age was 36.3 years (standard deviation: 6.78, ranging between 30 and 51). Five patients were nulliparous, and the other 3 were multiparous. Visual analog scale (VAS) was used to assess the patient’s symptoms better. Patients with VAS ≥ 4 were considered to have the symptoms. Seven patients (87.5%) had complaints of inguinal swelling or pain, and six mentioned exacerbations in their menstrual period (catamenial symptoms). Also, seven patients (87.5%) had dysmenorrhea, 6 (75.0%) had dyspareunia, and 6 (75.0%) had pelvic pain.Footnote 1
History
Two patients had a history of primary infertility. Two had a history of inguinal herniorrhaphy, and four had a history of previous abdominal surgery. Also, six patients were diagnosed with pelvic endometriosis before presenting to the author’s office. The patient’s characteristics, symptoms, and history are summarized in Table 1.
Physical examination and laboratory tests
Right and left inguinal mass was detected by physical examination in 6 patients (75.0%) and 1 patient (12.5%), respectively. Six patients had tenderness in the right groin and one on the left side. The Valsalva maneuver did not lead to an increase in the inguinal masse’s size. As shown in Table 1, the CA-125 value was measured in 4 patients. It was higher than the normal range in only 2 patients.
Imaging assessment
Inguinal ultrasound revealed IEM in 6 patients. Trans-abdominal and transvaginal ultrasounds were performed on two patients because they have symptoms associated with pelvic endometriosis. Also, two patients (25.0%) were misdiagnosed previously by ultrasound, one with inguinal hernia and the other with inguinal lymphadenopathy. IEM size increase was assessed for 2 patients. In one patient, IEM size increased about 17 × 1 mm during 4 years with an average growth of (4 × 0.25 mm) per year despite medical treatment with progestin and GnRH agonists. In another patient, the IEM size was decreased, but notably, she underwent medical treatment with progestin during those 2 years. Also, two patients underwent magnetic resonance imaging (MRI). It revealed IEM in both patients. As shown in Fig. 1, MRI in patient 2 revealed 29 × 51 mm growths during 9 months despite taking an oral contraceptive. We used imaging #Enzian classification to describe imaging assessment results better. Imaging’s findings are summarized in Table 1.

Comparison of inguinal endometriosis size in magnetic resonance imaging. A first magnetic resonance imaging (35 × 9 mm); B second magnetic resonance imaging 9 months later (61 × 60 mm)
Treatment and surgical methods
As shown in Table 1, medical treatment by progestin, GnRH agonist, and Dydrogesterone was performed on 6 Patients, leading to IEM size decrease in 2 of them; however, IEM size increased in 4 patients, and their pain got worse.
Laparoscopic surgical intervention was performed on 5 patients. Four underwent IEM resection surgery. Under general anesthesia, they secured a Trendelenburg position. A central umbilical trocar (12 mm), 2 lateral trocars (5 mm), and a suprapubic trocar (5 mm) were inserted. Intraoperative CO2 pressure was established at 13 mm Hg. First, endometriosis abdominal and pelvic exploration was performed. Then, inguinal canal exploration was performed. Inguinal mass was resected with a safe margin in these patients. In addition, in patient 5, IEM was adherent to the femoral, external iliac, and inferior epigastric vessels. So, surgery was performed by a multidisciplinary team, including an expert vascular surgeon and a gynecologist. IEM was resected with a safe margin without any vascular injury. Then, a skin incision was conducted in the groin. In patients with involvements, IEM mass was resected from the external oblique, transversus abdominis, internal oblique muscles, and Scarpa facia. IEM lesion and resected part of the round ligament were pulled out via a skin incision. The abdominal wall defect was repaired by Prolene 3-0 suture in all patients. Also, to avoid an incisional hernia, a PROLENE Mesh was placed on the inguinal canal and fixed with Prolene 3-0 suture for patient 5. Also, a Hemovac drain was established to prevent post-surgical collection in this patient. After abdominal wall repair, the peritoneal defect was repaired via laparoscopy to avoid gas leakage, subcutaneous emphysema formation, and intestinal hernia. In cases with co-existing inguinal hernia, Inguinal hernia sacs and IEM were resected, and the abdominal wall defects were repaired. Then, abdominal-pelvic laparoscopic exploration was performed, and endometriosis lesions were removed in patients with other endometriotic lesions.
Patient 6 underwent pelvic endometriosis laparoscopic surgery due to pelvic endometriosis diagnosis. Nevertheless, mild-size endometrioid implantations were identified accidentally surrounding the entrance of the inguinal hernia sac during laparoscopy (Figs. 2 and 3). As mentioned, she had no IEM, so she was excluded from statistical analysis.

Pre-operative imaging assessment and intraoperative findings of case 5. A groin palpable mass; B inguinal endometriosis in ultrasound; C rectum endometriosis in transvaginal ultrasound; D inguinal endometriosis in magnetic resonance imaging; E inguinal bulging was seen during abdominal exploration; F uterosacral ligament endometriosis; G round ligament, external iliac artery, and vein after making incision; H pulling out inguinal mass via skin incision after resection with safe margin; I placing PROLENE Mesh on the external orifice of the inguinal canal; J peritoneal defect repairment; K inguinal endometriosis; L rectum endometriosis and inguinal mass; M Hemovac drain on inguinal site and corrugated drain on the anastomosis

Abdominal view of inguinal endometriosis and pulling out inguinal mass via skin incision. A inguinal canal and round ligament involvement by endometriosis (patient 1); B endometriosis implantations on the internal orifice of the inguinal canal (patient 3); C superficial endometriosis surrounding the entrance of inguinal hernia sac (patient 6); D inguinal endometriosis and round ligament remove via skin incision (patient 2)
Surgical findings
Among patients who underwent surgical interventions for IEM, three patients (75%) had proximal part of the inguinal canal and round ligament involvement by IEM. However, in one patient (25%), the proximal part was not involved, and IEM involved the distal portion of the round ligament near the labia majora and pubic symphysis. Also, two had co-existing inguinal hernia. The surgical #Enzian classification was used to better describe the patients’ surgery findings. Surgical interventions and findings are summarized in Table 1.
Histopathological examination and follow-up
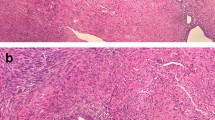
Histopathology examination revealed IEM in all four patients who had inguinal lesions. Also, it demonstrated abdominal wall endometriosis for patient 6 (Fig. 4).

Histopathological appearance of inguinal endometriosis. A glandular and stromal endometrial tissue surrounded by fibromuscular tissue × 40 LPF; B glandular and stromal endometrial tissue surrounded by fibromuscular tissue × 400 HPF
As shown in Table 1, during a long-time follow-up (> one year) for five patients who underwent surgery, patients had no complaints and suspected symptoms of IEM recurrence. The results of the statistical analysis are summarized in Table 2.
Discussion and conclusion
Clinical manifestations and differential diagnoses
This study discussed 8 cases of IEM with a mean age of 36. Five were nulliparous, so it seems there is no relationship between IEM and parity history. Catamenial groin pain or swelling was the most frequent symptom. Also, patients usually had accompanying symptoms such as pelvic pain and dysmenorrhea. One-half of patients had a history of previous abdominal surgery. Ultrasound was diagnostic in 4 patients (50%), and MRI was used in two patients (25%). Among 6 patients who underwent hormonal therapy, 4 (66.6%) experienced IEM size increase. IEM was right-sided in 87.5% of patients, and among 4 patients who underwent surgery, 75% had proximal site inguinal involvement.
About 133 cases of IEM were reported in the literature until 2022. The mean age is about 36 years old, and the largest number of the reported instances belongs to Japan [6]. Right-side IEM is more frequent than left-side; therefore, right inguinal swelling with pain exacerbation in the menstrual cycle is the typical clinical manifestation. Nevertheless, cases of bilateral or left-side IEM and cases without catamenial symptoms were reported [6]. Dysmenorrhea, dyspareunia, and pelvic pain are accompanying symptoms. However, in patients without these symptoms, IEM is not a diagnosis of exclusion [11]. Also, about 30% of IEM cases have a previous operation [6].
There are various causes for an inguinal mass, such as inguinal hernia, hydrocele of the canal of Nuck, inguinal lymphadenopathy, hemangioma, and malignancies [12,13,14]. Also, endometrial-like tissue can be identified in the sac of the inguinal hernia or the hydrocele of the canal of Nuck [13, 15]. So, about 20% of patients with IEM have Co-existing inguinal hernia or canal of Nuck hydrocele [6]. Several cases of IEM are misdiagnosed as an inguinal hernia due to the greater prevalence of inguinal hernia, less consideration of general surgeons for endometriosis, and insufficient post-operative histopathological assessments [10]. According to the wide range of differential diagnoses of inguinal swelling, diagnosis of the IEM is challenging and requires careful investigations. MRI is the most sensitive and specific imaging modality for IEM diagnosis. MRI identifies iron particles in the hemosiderin, in contrast with computed tomography. Therefore, MRI has more sensitivity and specificity than computed tomography. MRI shows IEMs as hyperechoic lesions on T1 images and hypoechoic on T2 images [11, 16,17,18]. However, ultrasound is valuable and diagnostic in most patients [6, 13, 19]. Abdominal ultrasound has been used to diagnose IEM in about 74% of patients [6]. Ultrasound is an appropriate modality for detecting cystic peritoneal implants in contrast to small peritoneal implantations. Still, the sensitivity and specificity of the ultrasound for the diagnosis of round ligament endometriosis have not been evaluated due to the limited number of studies [20].
A high CA-125 level is not identified in all cases of IEM, even though there are several cases of IEM with increased CA-125 [6]. Two patients (25%) among our study population had CA-125 levels higher than the normal range. In one of them, the CA-125 level was near the upper normal limit (36.96 U/Ml), and only one had a CA-125 high level (12.5%). In highly suspected cases of IEM, fine-needle aspiration cytology can confirm the IEM diagnosis before the operation, but it is not performed commonly [17].
Pathophysiology
Some theories describe the pathophysiology of endometriosis, including retrograde menstruation (Sampson theory), lymphatic or hematogenous benign metastasis, and Mullerianosis theory [21,22,23]. Dissemination of endometrial cells along the round ligament from the abdominal cavity is the more acceptable theory in cases with co-existing pelvic endometriosis. In these patients, endometriosis usually can be seen in the proximal part of the round ligament and inguinal canal [10]. Although, in isolated IEM without pelvic endometriosis, IEM nodules are usually seen on the distal part of the round ligament and not on the proximal portion. We hypothesize that Mullerianosis seems to be the most favorable theory in these patients. The round ligament involvement pattern can help to describe the appropriate theory in each patient better. Also, we hypothesize that the isolated distal part of the round ligament involvement by endometriosis is against retrograde menstruation theory and advocates for the Mularianosis theory in patients without co-existing pelvic endometriosis.
Peritoneal fluid circulates clockwise because of gravity and diaphragm respiratory movements [24]. Although, endometrial free cells in the peritoneal fluid spread in the abdominal cavity. The sigmoid colon prevents the entrance of the peritoneal fluid to the left inguinal canal [10]. The right-side canal does not have this support, so the round ligament plays a role as a transmitter of endometrial cells to the groin. It can be an appropriate explanation for IEM cases with co-existing pelvic endometriosis [10]. According to these two facts, the right-side dominancy of the IEM can be described [25].
Treatment
Surgical excision of the inguinal mass with inguinal canal exploration is the most common treatment [6]. The operation can be achieved by both open and laparoscopic approaches [26]. Due to the proximity of IEM lesions, external iliac and femoral vessels, complete resection of the inguinal mass with a safe margin without vessel wall damage is the most critical issue that should be considered during surgical excision. In case of co-existing inguinal hernia or canal of Nuck hydrocele, excision of the hernia sac and abdominal wall repairment by Mesh is required [10, 26]. Laparoscopic pelvic and abdominal cavity exploration is probably needed in case of co-existing pelvic or abdominal endometriosis. Patients who undergo inguinal herniorrhaphy with suspected findings (such as thickening of the hernia sac wall, bloody fluid inside the sac, or thickening of the extraperitoneal round ligament) during the surgery by general surgeons should refer to gynecologists for more assessments about other sites of endometriosis [10].
The sufficiency of hormonal therapy for IEM is not strongly acceptable and requires more investigation due to the limited number of patients undergoing medical treatment [6]. Post-operation hormonal therapy is often performed to prevent endometriosis recurrence [27]. Nevertheless, despite the slight recurrence rate of IEM, the benefits of hormonal treatment should be investigated [6]. However, for patients with IEM, enough time should be considered to choose the best surgical team and plan due to the low velocity of IEM growth.
Definitive diagnosis of IEM is based on post-operative histopathological examination [5]. Post-operative histopathological examination is crucial due to variations of histopathological findings, such as uterus-like tissue and malignant clear-cell carcinoma [6, 28].
In conclusion, IEM is a rare condition requiring precise diagnosis assessments. In case of an inguinal mass with aggravated swelling or pain in the menstrual period, IEM should always be considered. MRI is the most sensitive modality of IEM diagnosis. Also, ultrasound has been used for diagnosis. However, because ultrasound is an operator-dependent modality, suspected patients for IEM should be referred to an expert sonologist with enough experience in endometriosis diagnosis. Due to a wide range of differential diagnoses of groin masses, IEM can be misdiagnosed commonly. A more precise post-operative histopathological examination is required about inguinal masses. In cases that undergo inguinal herniorrhaphy and diagnosis with IEM during or after the operation, a gynecological consultant is necessary to investigate the other sites of endometriosis.
Availability of data and materials
Further information about this study is available by contacting the corresponding author.
Notes
Patient 6 has mild-size superficial endometriosis implantations surrounding the entrance of the inguinal hernia sac, which was identified accidentally during laparoscopic abdominal and pelvic exploration for endometriosis, but she had no IEM, so she was excluded, and then statistical analysis was performed on 8 patients with IEM.
Abbreviations
- IEM:
-
Inguinal endometriosis
- VAS:
-
Visual analog scale
- MRI:
-
Magnetic resonance imaging
References
de Graaff AA, D’Hooghe TM, Dunselman GAJ, Dirksen CD, Hummelshoj L, Simoens S, et al. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28:2677–85.
Mehedintu C, Plotogea MN, Ionescu S, Antonovici M. Endometriosis still a challenge. J Med Life. 2014;7:349–57.
Lee HJ, Park YM, Jee BC, Kim YB, Suh CS. Various anatomic locations of surgically proven endometriosis: a single-center experience. Obstet Gynecol Sci. 2015;58:53.
Blanco RG, Parithivel VS, Shah AK, Gumbs MA, Schein M, Gerst PH. Abdominal wall endometriomas. Am J Surg. 2003;185:596–8.
Jena SK, Begum J, Kumari S, Kar C. The groin endometriosis: a great mimicker of common groin conditions. J Gynecol Surg. 2020;36:30–3.
Dalkalitsis A, Salta S, Tsakiridis I, Dagklis T, Kalogiannidis I, Mamopoulos A, et al. Inguinal endometriosis: a systematic review. Taiwan J Obstet Gynecol. 2022;61:24–33.
Zihni İ, Karaköse O, Özçelik KÇ, Pülat H, Eroloğlu HE, Bozkurt KK. Endometriosis within the inguinal hernia sac. Turk J Surg. 2020;36:113–6.
Prodromidou A, Pandraklakis A, Rodolakis A, Thomakos N. Endometriosis of the canal of nuck: a systematic review of the literature. Diagnostics. 2020;11:3.
Niitsu H, Tsumura H, Kanehiro T, Yamaoka H, Taogoshi H, Murao N. Clinical characteristics and surgical treatment for inguinal endometriosis in young women of reproductive age. Dig Surg. 2019;36:166–72.
Li S-H, Sun H-Z, Li W-H, Wang S-Z. Inguinal endometriosis: ten case reports and review of literature. World J Clin Cases. 2021;9:11406–18.
Hagiwara Y, Hatori M, Moriya T, Terada Y, Yaegashi N, Ehara S, et al. Inguinal endometriosis attaching to the round ligament. Australas Radiol. 2007;51:91–4.
Yang DM, Kim HC, Ryu JK, Lim JW, Kim GY. Sonographic findings of inguinal endometriosis. J Ultrasound Med. 2010;29:105–10.
Cervini P, Mahoney J, Wu L. Endometriosis in the canal of nuck: atypical manifestations in an unusual location. Am J Roentgenol. 2005;185:284–5.
Fujikawa H, Uehara Y. Inguinal endometriosis: unusual cause of groin pain. Balkan Med J. 2020;
Albutt K, Glass C, Odom S, Gupta A. Endometriosis within a left-sided inguinal hernia sac. J Surg Case Rep. 2014;2014:rju046–rju046.
Licheri S, Pisano G, Erdas E, Ledda S, Casu B, Cherchi MV, et al. Endometriosis of the round ligament: description of a clinical case and review of the literature. Hernia. 2005;9:294–7.
AlSinan FM, Alsakran AS, Foula MS, al Omoush TM, Al-Bisher H. Inguinal endometriosis in a nulliparous woman mimicking an inguinal hernia: a case report with literature review. Am J Case Rep. 2021;22.
Gaeta M, Minutoli F, Mileto A, Racchiusa S, Donato R, Bottari A, et al. Nuck canal endometriosis: MR imaging findings and clinical features. Abdom Imaging. 2010;35:737–41.
Kamkarfar P, Shahriyaripoor R, Rokhgireh S, Mostafavi SRS, Chaichian S, Mehdizadeh KA. Comparison of diagnostic values of transvaginal sonography with laparoscopic and histological results in the evaluation of uterosacral ligaments’ involvement in endometriosis patients. Caspian J Intern Med. 2022;13:705–12.
Bazot M, Daraï E. Diagnosis of deep endometriosis: clinical examination, ultrasonography, magnetic resonance imaging, and other techniques. Fertil Steril. 2017;108:886–94.
Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol. 1927;14:422–69.
Pergialiotis V, Lagkadas A, Polychronis O, Natsis S, Karakalpakis D, Giannakopoulos K. Endometriosis-associated ovarian cancer. Presentation of a case report and review of the literature. Eur J Gynaecol Oncol. 2011;32:682–5.
Batt RE, Yeh J. Müllerianosis: four developmental (embryonic) mullerian diseases. Reprod Sci. 2013;20:1030–7.
Sun Z-J, Zhu L, Lang J-H. A rare extrapelvic endometriosis: inguinal endometriosis. J Reprod Med. 2010;55:62–6.
Burcharth J. The epidemiology and risk factors for recurrence after inguinal hernia surgery. Dan Med J. 2014;61:B4846.
Hwang B, Bultitude J, Diab J, Bean A. Cyst and endometriosis of the canal of Nuck: rare differentials for a female groin mass. J Surg Case Rep. 2022;2022.
Lee SE, Jo DH, Moon SH, Chong HI, Shin SI, Kim HG, et al. A case of inguinal endometriosis in the absence of previous gynecologic surgery. Korean J Obstet Gynecol. 2008;51:261–4.
Seki A, Maeshima A, Nakagawa H, Shiraishi J, Murata Y, Arai H, et al. A subserosal uterus-like mass presenting after a sliding hernia of the ovary and endometriosis: a rare entity with a discussion of the histogenesis. Fertil Steril. 2011;95:1788.e15-1788.e19.
Acknowledgements
Not applicable.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
AH contributed to the conception, design, and supervision of the study. AF, HZ, and SM performed material preparation, data collection, and analysis. AF wrote the first draft of the manuscript. MG performed the manuscript reviewing and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The written consent was obtained from each participant. Nikan Hospitals Ethics Committee (Tehran, Iran) approved this study protocol.
Consent for publication
Written informed consent was obtained from the patients for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Haghgoo, A., Faegh, A., Mostafavi, S.R.S. et al. Inguinal endometriosis: a case series and review of the literature. J Med Case Reports 18, 83 (2024). https://doi.org/10.1186/s13256-024-04400-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-024-04400-x