
Abstract
Chronic obstructive pulmonary disease(COPD) is an inflammatory disease characterized by the progressive and irreversible structural and functional damage of lung tissue. Although COPD is a significant global disease burden, the available treatments only ameliorate the symptoms, but cannot reverse lung damage. Researchers in regenerative medicine have examined the use of stem cell transplantation for treatment of COPD and other diseases because these cells have the potential for unlimited self-renewal and the ability to undergo directed differentiation. Stem cells are typically classified as embryonic stem cells, induced pluripotent stem cells, and adult stem cells (which includes mesenchymal stem cells [MSCs]), each with its own advantages and disadvantages regarding applications in regenerative medicine. Although the heterogeneity and susceptibility to senescence of MSCs make them require careful consideration for clinical applications. However, the low tumourigenicity and minimal ethical concerns of MSCs make them appear to be excellent candidates. This review summarizes the characteristics of various stem cell types and describes their therapeutic potential in the treatment of COPD, with a particular emphasis on MSCs. We aim to facilitate subsequent in-depth research and preclinical applications of MSCs by providing a comprehensive overview.
Similar content being viewed by others


Introduction
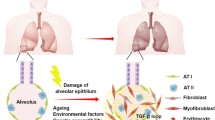
Chronic obstructive pulmonary diseases (COPD) is a heterogeneous lung disease that has high morbidity and mortality worldwide, and is an increasing economic and social burden [1, 2]. The recent burden of obstructive lung disease study and other large-scale epidemiological studies estimated that the global prevalence of COPD is 10.3% [3]. Another recent study estimated that the increasing prevalence of smoking in low- and middle-income countries and aging populations in high-income countries will lead to more than 5.4 million annual deaths from COPD and related conditions by 2060 [4]. Long-term exposure to cigarette smoke, harmful chemicals, smoke from burning fuels, and α1-antitrypsin deficiency are the main causes of COPD [5] (Fig. 1). As COPD progresses, patients experience irreversible obstruction of airflow, hypersecretion of mucus, destruction of alveolar wall, and proliferation of airway smooth muscle cells due to the chronic bronchitis and/or emphysema [6].

Risk factors and pathogenesis of COPD. By figdraw (www.figdraw.com)
Chronic bronchitis is characterized by non-specific inflammation of the mucosa and surrounding tissues of the trachea and bronchi, and is triggered by an infection or non-infectious factors (allergy, oxidative stress) in which the major pathological change is damage of epithelia in the central airway [7]. Prolonged inflammatory stimulation causes proliferation of bronchial mucosal cells and mucosal hypertrophy, resulting in obstruction of the airways and decreased ventilation. The excessive secretion of mucus and infiltration of inflammatory cells leads to the accumulation of mucus in the bronchial lumen, further aggravating the narrowing and obstruction of airways [8]. Emphysema is characterised by dilatation and destruction of lung tissue beyond the terminal fine bronchioles. Its manifestations are thinning of the alveolar walls; enlargement, rupture, or formation of large blisters in the alveolar cavities; reduced blood supply; and destruction of the elastic fibrous network [9].
COPD is, therefore, a multifactorial disease with a complex pathogenesis, and many studies have focused on the accumulation of inflammatory cells, the imbalance of protease/antiprotease activity, and oxidative stress [5, 10, 11] (Fig. 1). There is evidence that cigarette smoke and other inhaled particulates stimulate epithelial cells to produce reactive oxygen species, and that this induces inflammatory cells to infiltrate the periphery of the airways, leading to an imbalance of protease/antiprotease activity [12,13,14]. Elastin is a major protein in the connective tissue of the lung parenchyma, and an imbalance between proteases and antiproteases can decrease the level of elastin, leading to lung hyperinflation, lung dilatation, and loss of lung elasticity, culminating emphysema [15,16,17]. During disease progression, COPD patients experience a gradual decline in lung capacity which initially limits their ability to exercise, and eventually becomes disabling [18]. Although chronic bronchitis and emphysema are the predominant clinical phenotypes of COPD, these patients may also present with several other complications, such as airway hyperresponsiveness, hyperimmune response, asthma, and other lung diseases [19]. The many symptoms of COPD are responsible for its huge personal, social, and economic burden. COPD is incurable, but the clinical management of symptoms includes smoking cessation, vaccinations for respiratory pathogens, various medications (especially bronchodilators and steroids), oxygen therapy, and pulmonary rehabilitation [8]. These treatments aim to control the symptoms, decrease inflammation, and improve functional capacity. The use of anti-inflammatory drugs and bronchodilators reduces the severity of symptoms and improves patient quality-of-life, but these treatments only relieve symptoms and do not block or reverse lung damage [20]. Although smoking cessation and long-term oxygen therapy are relatively effective, they do not halt the underlying pathology of increased inflammation, apoptosis, and oxidative stress [21,22,23]. There are currently no treatments for the irreversible loss of lung function and incompletely reversible limitation of expiratory airflow, so there is an urgent need to develop new treatments that can repair the damaged lung tissues of patients with COPD.
Stem cells are undifferentiated cells with the capacity for self-renewal and multispectral differentiation, and cell-based tissue reconstruction using stem cells is an important part of regenerative medicine [24]. Cellular therapeutic approaches may provide new treatment options for COPD in the future. The unique properties of stem cells are that they can promote tissue repair and regeneration by replacing damaged cells, modulate immune responses, reduce inflammation, and promote tissue homeostasis [25]. Thus, a promising general approach for using stem cells to treat COPD is to harness their capacity for differentiation by stimulating them to regenerate lung parenchymal cells and airways, and/or to promote stem/progenitor cell differentiation of epithelial cells to restore the balance between proliferation and apoptosis.
Types of stem cells
The most important function of stem cells is their maintenance of cellular regeneration, in that they can differentiate into at least one type of highly mature cell. This means that stem cells have great potential for use in tissue repair if they can be promoted to replace diseased and damaged tissues [26]. There are three general types of stem cells: embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs) and adult stem cells (MSCs and several others) [27]. ESCs and iPSCs have the potential for unlimited proliferation and differentiation into all germ layers, and therefore have great potential for treatment of refractory diseases and injuries [28]. Adult stem cells are immature cells in adult tissues that are in a resting state, which function as a reservoir for self-renewal because of their ability to differentiate into highly specialised cells and repair tissue following injury [29]. There are two types of adult stem cells that affect airway function in COPD: mesenchymal stem cells (MSCs) and lung progenitor/stem cells.
Embryonic stem cells
ESCs are pluripotent stem cells isolated from blastomeres that can differentiate into all types of cells, making them highly valuable in regenerative medicine [30, 31]. Since 1998, when hESCs were first cultured and differentiated, many studies of drug-based therapies using ESCs have examined their use for treatment of spinal cord injury, macular degeneration, type 1 diabetes, heart failure, and other conditions [32]. ESCs also have potential for treatment of lung diseases, and studies have demonstrated that hESCs and mouse ESCs can differentiate into type II alveolar epithelial cells (ATIICs) using controlled culture conditions [33, 34]. Previous studies have used established transfection and culture procedures in a laboratory setting to develop genetically screened and highly purified hESC-ATIICs that have characteristics typical of ATIICs, including formation of lamellipodia, expression of surfactant protein, and the ability to proliferate and differentiate into type I alveolar epithelial cells (ATICs) [35]. Previous research demonstrated that ATIICs derived from hESCs can be engrafted into the lungs of mice with acute lung injury, and that this treatment inhibited or reversed fibrotic changes induced by bleomycin [36]. Although hESC-ATIICs have potential as a cellular source for treatments of distal lung diseases, there are many concerns regarding the safety of cell transplantation from differentiated ESCs. Methods such as the formation of embryoid bodies or coculture of these cells with lung mesenchyme have only produced small numbers of ATIICs [33, 34, 37, 38]. Another important concern is that the presence of pluripotent cells within a mixed population of ESC-derived cells may lead to formation of a teratoma, making this approach unsuitable for transplantation into the lungs. There are also serious ethical concerns, because the acquisition of hESCs necessitates the destruction of embryos.
A disadvantage of allogeneic transplantation of hESCs is that they can elicit a strong immune reaction; this necessitates intensive immunosuppressive treatment to prevent rejection, which increases the risk of an opportunistic infection and tumor development [39, 40].Many studies have therefore attempted to produce personalized hESCs to prevent immune rejection. For example, the implementation of alternative targeted methods, such as b2-microglobulin-deficient hESCs, greatly decreases the susceptibility of stem cells to recognition by CD8 + T cells. This approach can potentially provide a sustainable reservoir of cells for tissue regeneration without the need for matching of human leukocyte antigens (HLAs) [41]. A clinical case report showed that treatment with hESCs decreased symptoms in a patient with emphysema [42]. Although preclinical studies showed that ESCs can regenerate lung structures, the potential for teratoma formation, immune rejection, and ethical issues have prevented the development of clinical trials that use hESCs for treatment of COPD [43]. To address these ethical concerns and technical limitations, researchers have instead taken alternative approaches that use adult stem cells or iPSCs.
Induced pluripotent stem cells
iPSCs, which are generated by reprogramming adult somatic cells (e.g., skin cells) into a pluripotent state, have great potential for use in regenerative medicine. In 2006, the Yamanaka team reported the successful reprogramming of differentiated somatic cells into a cell type resembling embryonic stem cells by introduction of specific transcription factors. Since then, many researchers have utilized these cells as a source for regeneration in studies of disease-specific cells in different animal models, drug screening, and development of cell-based therapies [44]. hiPSCs are a promising source of therapeutic cells because they have totipotency similar to hESCs, they can differentiate into a variety of cell types, they do not induce strong immune responses, and there are no serious ethical concerns regarding their use [45, 46]. Extracting somatic cells from a patient and reprogramming them into iPSCs greatly reduces the risk of immune rejection after transplantation and improves the feasibility and safety of cell transplantation. Controlled differentiation programs allow iPSCs to develop into specific cell lineages, so they can replace the damaged cells that are in the tissues or organs affected by specific diseases [47]. There is also evidence that hiPSCs undergo targeted differentiation to produce alveolar epithelial cell type 2 (iAT2) cells, and that hiPSCs derived from distal lung cells can be implanted into the lungs, where they contribute to the formation of functional distal lung units and slow the progression of emphysema [48, 49].
Although iPSCs appear to have great potential, several limitations need to be addressed. One concern is “reprogramming efficiency”, because the process is slow and inefficient, even though it is reproducible [50]. Although recent advances showed that iPSCs can be amplified in scalable suspension cultures, and that large quantities of human iPSCs can be produced in a fully controlled bioreactor [51], further technological improvements are needed for producing “clinical-grade” iPSCs. Another important consideration is the risk of genetic and epigenetic abnormalities during reprogramming, because reprogrammed iPSCs may have different genomic instabilities that lead to development of a malignancy. In particular, the random integration of multiple copies of a transgene into the host genome during the overexpression of reprogramming factors can lead to significant phenotypic variability, and to potential disruptions in the function of critical genes in the generated iPSCs [44]. An even greater concern is that genomic alterations caused by the integration of transcription factor genes into the genome could lead to tumorigenicity [31]. There are also immunological concerns associated with cell therapies that utilize iPSCs [52]. Given the continuing improvements in the protocols used for differentiation and the availability of better techniques for enrichment, purification, and analysis, it may soon be possible to eliminate undifferentiated cells from the differentiated cell products. The risk of teratoma formation appears to be very low when using highly enriched cell products [53].
iPSCs have several potential uses in regenerative medicine studies: directly for cell transplantation, as a source of differentiated cells, and in model systems to explore the role of epigenetic reprogramming in abnormally functioning cells. Most research has focused on the last two methods [54]. Although clinical trials are increasingly using hESC or hiPSC derivatives to repair organs and treat diseases, our search of ClinicalTrials.gov identified 96 clinical trials using iPSCs, but only 5 that were related to lung and respiratory diseases, and none that examined iPSCs as a treatment for lung diseases in [53]. The challenges associated with vector integration, suboptimal efficiency in generation of hiPSCs, and the demand for different types of transplantable cells led to the development of a novel vector incorporating a Tet-On inducible gene expression system, an ATII C-specific NEOR transgene, and loxP target sequences. This innovative approach enabled the successful generation of hiPSC-ATIICs whose ultrastructural characteristics and functional properties were similar to those of ATIICs [55]. Similar hESCs-ATIICs and hiPSCs-ATIICs have significant promise for in vivo transplantation, differentiation into ATICs for alveolar regeneration following bleomycin-induced injury, and improving the function of damaged lungs [44]. However, the process of obtaining tissue-specific cells from iPSCs requires labor-intensive reprogramming and directed differentiation. It is imperative to develop expedited approaches, such as direct reprogramming of one somatic cell type into another cell type, as a more effective strategy for generation of iPSCs [56].
Lung progenitor/stem cells
The adult lung is a complex organ consisting of many types of cells that are distributed throughout the respiratory tract, and each region is characterized by its own distinct population of epithelial cells. Stem/progenitor cells from various epithelial lineages within the lung function in lung development, tissue maintenance, and repair following injury [57]. The maintenance of a precise equilibrium between each region-specific type of stem cell and its specific microenvironments is essential for the preservation of normal lung function and airway integrity during normal conditions and during the repair of lung damage. The region-specific epithelial stem/progenitor cells in the lungs of human adults and mice consist of basal cells, secretory cells, and mucous cells in the proximal airway submucosal glands; variant secretory cells in the small bronchi; bronchoalveolar duct junction stem cells; and a subset of ATIICs in the alveolar sac [58, 59]. Lung progenitor/stem cells have the capacity to undergo proliferation and differentiation following lung injury in order to restore damaged cell populations and uphold the typical physiological functioning of the lung [25]. Among these, basal cells are a key type of epithelial stem cell, because they play a crucial role in maintaining environmental homeostasis and promoting the repair of epithelial in the proximal airways. Bronchioalveolar stem cells are essential for repairing damage to the small bronchi and alveolar cells, and they play a crucial role in maintaining stability of the lung environment. Bronchoalveolar stem cells exhibit a diverse differentiation response to various forms of injury, giving rise to cell types including club cells and ciliated cells. Within the gas exchange region of the adult lung, a subset of ATIICs are stem/progenitor cells for ATICs, and ATIICs function as stem cells by maintaining epithelial homeostasis during normal conditions and in response to injury [57]. Through lineage tracing experiments, it has been demonstrated that AT2 cells, serving as stem/progenitor cells, possess the ability to self-renew and undergo transdifferentiation into AT1 cells [25]. The ability of the lung to self-repair following injury requires activation of stem cells and progenitor cells within each respiratory alveolus.
Individuals with COPD experience oxidative stress and disruption of the equilibrium between self-renewal and differentiation of stem/progenitor cells, and this prevents the regeneration of lung tissue [9]. Thus, there is an urgent need for more basic studies and clinical studies that examine the use of lung stem/progenitor cells for the management of COPD and other pulmonary ailments. We searched for clinical trials using bronchial basal cells for the treatment of COPD, of which only one had relevant results published. In this study, autologous P63 + lung progenitor cells were transplanted into COPD subjects, and the results suggest that transplantation of cultured P63 lung progenitor cells is safe and may represent a potential therapeutic strategy for COPD (NCT03188627) [60]. There has been great interest in the potential use of exogenous stem/progenitor cells to regenerate or enhance lung repair in patients with COPD, but significant hurdles must be overcome. Firstly, it is difficult to obtain sufficient quantities of autologous stem cells. Secondly, there is insufficient information regarding the identification and characterization of defined lung stem/progenitor cell subpopulations. Lastly, most current cell implantation techniques are inefficient and lack long-term efficacy [61]. Although several clinical studies have examined the use of endothelial progenitor cells and basal epithelial cells from the bronchus for investigational interventions, direct implantation of cells required for airway function is a potential approach for regenerating damaged lung tissue, and further studies using animal models are needed.
Mesenchymal stem cells
MSCs are a subset of stem cells that exhibit morphological similarities to fibroblasts and are found within the connective tissues of nearly all organs. In 2006, the International Society for Cellular Therapy (ISCT) delineated specific criteria for the identification of MSCs [62]: (1) adherence to plastic surfaces under standard culture conditions, (2) expression of a defined set of surface antigens, and (3) the capacity to differentiate into osteoblasts, chondrocytes, and adipocytes. MSCs exhibit low immunogenicity due to their lack of MHC-II antigen expression. Additionally, MSCs possess immunosuppressive capabilities, forming the foundation for their application in cell therapy. Extensive research utilizing animal models has been undertaken to evaluate the efficacy of MSCs and to progressively elucidate the mechanisms underlying MSC-based tissue repair therapies. Consequently, MSCs are emerging as a potent therapeutic tool for a wide range of diseases. Further investigation into their biological properties is essential to establish the theoretical groundwork necessary for clinical applications. MSCs will be elaborated in more detail below.
Strengths and weaknesses of different types of stem cells
Stem cells, with their unique characteristics of self-renewal and differentiation, are the focus of regenerative medicine. These different types of stem cells have distinct biological characteristics and differentiation potentials, and the best is still controversial. Advantages and disadvantages of different types of stem cells are briefly summarized in Fig. 2. Embryonic stem cells are highly undifferentiated cells that can be induced to differentiate into almost all cell types of the organism, but cannot develop into complete individuals. ESCs have long been expected to be the most promising cell source in the regenerative medicine. Ethical controversies, tumour formation and immune rejection make the use of embryonic stem cells a huge obstacle. As a replacement for ESCs, iPSCs are not beset with any serious ethical issues, but oncogenicity and cellular deterioration due to incomplete reprogramming remain challenges. Lung progenitor/stem cells are adult stem cells with the advantages of having low tumourigenicity, being suitable for autologous transplantation, and being less ethically problematic. However, lung progenitor/stem cells are rare and difficult to isolate and characterize. All of these cells seem to have insurmountable difficulties to be used in therapy, but the discovery of mesenchymal stem cells offers new hope for the development of regenerative medicine. MSCs are not only readily available from a wide range of sources, with low immunogenicity to avoid rejection, but also perfectly avoid the major drawbacks of other stem cells through immune modulation and suppression of inflammatory responses, making them an ideal cell choice for use in regenerative medicine and therapeutic areas. Conversely, most small-scale clinical trials in regenerative medicine that used MSCs, which are considered non-pluripotent, have not reported significant safety concerns [63]. Despite these advantages, the heterogeneity of MSCs poses problems such as unstable differentiation efficiency and susceptibility to senescence. Extensive and ongoing research is underway to ensure that MSCs are safe and effective in the long term. The future strategies may include: pre-treating stem cells prior to transplantation, or combining stem cell therapies with other therapeutic modalities (e.g., pharmacological interventions or gene therapy) to enhance their therapeutic effects; and developing biomaterials and scaffolds that are structurally similar to tissues and provide structural support that promotes stem cell survival, differentiation, and integration into damaged lung tissues [47]. A number of other cellular approaches may lead to better treatments for chronic respiratory diseases, such as the use of stem/progenitor cells for lung repair, implantation of cells in small animal models, derivation of clinically relevant cell types from human iPSCs, and ex vivo lung generation using decellularized lung scaffolds [64].

Advantages and disadvantages of different types of stem cells. By figdraw (www.figdraw.com)
Mesenchymal stem cells
MSCs are multipotent stem cells that are widely used in regenerative medicine because they are easy to isolate and culture, and because they have immunomodulatory effects and immune privilege. Many preclinical and clinical trials have reported that MSCs have a favorable safety profile, making them suitable for therapeutic interventions that target chronic lung diseases because they can rapidly localize to the lungs after infusion. Compared to other types of stem cells, MSCs are easier to isolate and widely available, and their use is not prevented by ethical concerns.
MSCs are believed to reside within the connective tissue of numerous organs, such as adipose tissue, the placenta, umbilical cord blood, the umbilical cord, and dental pulp, and the most widely used types are bone marrow MSCs (BM-MSCs), adipose MSCs (AD-MSCs), and umbilical cord MSCs (UC-MSCs) [65,66,67,68,69]. A patient who receives MSCs that are obtained by isolating and culturing the patient’s own bone marrow or adipose tissue (autologous transplantation) have a greatly reduced the risk of immune rejection [47]. MSCs can also be manipulated in vitro and in vivo to differentiate into various cell types, including endodermal cells (pneumocytes, myoblasts, and intestinal epithelial cells) and ectodermal cells (epithelial cells and neurons), making them especially promising for treatment of lung diseases [70,71,72]. Moreover, MSCs have immunomodulatory properties, in that they can dampen inflammatory and autoimmune reactions, and they release growth factors and extracellular vesicles that can facilitate tissue regeneration and repair.
Studies of animal models of emphysema demonstrated that intravenous or intratracheal administration of lung-MSCs or BM-MSCs led to repair of lung injury; improved lung function; increased the levels of EGF, HGF, and VEGF; decreased airway inflammation; inhibited the release of proteases from inflammatory cells due to down-regulation of cyclooxygenase-2; and increased the proliferation of AT1 and AT2 cells [73,74,75]. Moreover, preclinical studies demonstrated that MSCs have significant therapeutic potential due to their anti-inflammatory, microbicidal, angiogenic, and antifibrotic properties, properties that lead to improved lung function and increased survival rates in individuals with chronic inflammatory lung diseases [76].
Despite the significant therapeutic potential of MSCs, their limitations must also be considered before they are used in patients. Firstly, because MSCs are adult stem cells they have a limited potential for differentiation, and therefore a limited ability to generate the specific types of lung cells required for complete tissue regeneration [47]. Secondly, MSCs are a heterogeneous group of cells whose therapeutic efficacy is highly variable, and there are differences in disease phenotypes and patient phenotypes. Different cell sources, therapeutic dosages, and routes of administration may all affect the function of MSCs; culture conditions, number of passages, and other factors can also affect their function. More notably, a growing number of studies showed that MSCs undergo rapid apoptosis, autophagy, or have cytotoxic effects after systemic and potentially after intratracheal administration [64]. Although a wealth of data from preclinical studies suggest that MSCs can decrease chronic inflammation, whether this also occurs in clinical settings and produces clinical benefits remains to be determined. Finally, aging and a decreased proliferative capacity can adversely affect the function and regenerative potential of MSCs. More specifically, multiple passaging of MSC cultures induces cellular senescence and decreases their potential therapeutic efficacy. Sorting and exclusion of CD26-positive MSCs from heterologous cell populations leads to enhanced cell attachment in vitro and reduces the secretion of senescence-associated cytokines, and CD26-negative MSCs had excellent efficacy in a mouse model of emphysema [77]. Therefore, strategies that rejuvenate or selectively remove senescent MSCs may increase the clinical efficacy of this approach.
To date, a relatively large number of clinical trials have demonstrated that MSCs are safe. However, despite the initial hope that implantation of MSCs would be an efficacious treatment for lung diseases, the therapeutic efficacy of MSCs in clinical settings has not yet been demonstrated. In 2011, a clinical trial of infusion of autologous bone marrow mononuclear cell for the treatment of patients with advanced emphysema was carried out in Brazil, and the follow-up results confirmed that bone marrow mononuclear cell infusion is safe (NCT01110252) [78]. Treatment of COPD with MSCs (Prochymal™) showed a decrease in c-reactive protein levels, suggesting a possible improvement in the inflammatory process. However, no improvement in lung function or patient quality of life was found (NTC00683722) [79]. No adverse events were found in patients with severe emphysema who underwent lung volume reduction surgery followed by infusion of autologous MSC (NCT01306513) [80]. We found that individuals enrolled in clinical trials investigating MSC therapy for COPD primarily consisted of patients with moderate-to-severe COPD, potentially reflecting the progressive nature of the disease. While early-stage COPD symptoms can be managed with medication, individuals with end-stage respiratory failure from severe emphysema often require lung transplantation as the final treatment option. Numerous uncertainties and unresolved concerns persist regarding the effectiveness and safety of MSC therapies, underscoring the necessity for further clinical trials to address these gaps in knowledge.
Sources of mesenchymal stem cells
Bone marrow-derived mesenchymal stem cells
MSCs of various origins, including bone marrow, adipose tissue, and the umbilical cord, are frequently used in clinical trials. Bone marrow is the primary and paramount reservoir of MSCs, and BM-MSCs have been extensively studied in preclinical studies and clinical stem cell therapy trials. Friedenstein and colleagues initially discovered MSCs in bone marrow stromal cells in the 1970’s by using natural adhesion techniques. Since then, many preclinical studies have investigated the potential use of BM-MSCs for treating a range of diseases. Despite the perceived safety of bone marrow aspiration, the procedure is invasive, uncomfortable, and can lead to severe pain and infection [65]. Moreover, the restricted availability and high density of bone marrow lead to low yields of isolatable cells [81]. BM-MSCs from elderly patients have elevated expression of genes associated with aging, shorter telomeres, diminished proliferative capability, and decreased potential for differentiation [82].
Adipose tissue-derived mesenchymal stem cells
There has been significant interest in AD-MSCs in recent years due to their high versatility and capability for differentiation. These cells are a distinct population of progenitor cells within adipose tissue stromal compartments that can differentiate into various types of cells, including neurons, skeletal muscle cells, and osteoblasts [65]. The pioneering work of Zuk et al. in 2001 described the isolation of AD-MSCs that had the potential for multilineage differentiation from liposuction-derived adipose tissue, demonstrating that AD-MSCs were a promising alternative to BM-MSCs [65]. Notably, adipose tissue has more MSCs than bone marrow, and the surge in clinical trials examining AD-MSCs may be because adipose tissue is more plentiful and easily obtained than bone marrow. AD-MSCs will likely play a prominent role in future research until superior alternatives are developed.
AD-MSCs are morphologically similar to BM-MSCs, they can differentiate into diverse mesodermal tissues, and they express analogous cell surface proteins. Adipose tissue contains significant number of primitive stromal stem cells, with up to 5000 AD-MSCs per gram of fat, in contrast, bone marrow contains 100 to 1000 stem cells per milliliter [65]. Collection of AD-MSCs is also more convenient than collection of BM-MSCs, because it can achieved by the minimally invasive procedure of liposuction under local anesthesia. Liposuction is a common cosmetic procedure in which the fat tissue is frequently discarded, but these tissues could be used as a valuable source of stem cells [83]. There is evidence that the proliferation of AD-MSCs is approximately two-fold greater than that of other types of stem cells. Thus, extracting a small quantity of fat allows the rapid collection of a large number of AD-MSCs, thereby mitigating the risks associated with cell differentiation and mutation during in vitro culture [84]. Although AD-MSCs and BM-MSCs have many biological similarities, they also have some differences in terms of immunophenotype, differentiation potential, transcriptome, proteome, and immunomodulatory activity. Despite these differences, AD-MSCs appear to be as effective as BM-MSCs in certain clinical applications and may be more suitable in some cases [85].
Umbilical cord-derived mesenchymal stem cells
Perinatal mesenchymal stem cells can be obtained from various sources, such as the umbilical cord, umbilical cord blood, and Wharton’s jelly (muco-polysaccharides in the umbilical cord), and their collection is typically considered noninvasive and free from ethical concerns. Although UC-MSCs account for only 7–10% of all cells in the umbilical cord, their rapid proliferation allows for efficient expansion using in vitro culture [86].
Although MSCs from bone marrow, adipose tissue, and the umbilical cord have many characteristics in common, they differ in terms of immunophenotype, differentiation potential, and immunomodulatory properties. Clinical trials examining the efficacy of these different MSCs in treating neurodegenerative diseases, endocrine and reproductive disorders, skin regeneration, abnormalities in pulmonary development, and cardiovascular diseases have confirmed they have diverse functions and presumably different therapeutic potential. The process of selecting specific types of MSCs for treatment of different specific diseases is currently problematic. These cells may have similar effects on inhibiting disease progression in vitro, but the mechanisms differ, necessitating further preclinical research and clinical trials to indentify the mechanisms of MSCs that are from different sources [25].
Mechanisms by which mesenchymal stem cells repair lung injury
MSCs, which are considered to be multipotent stem cells, can be obtained from diverse tissues. Previous studies have administered MSCs from different sources utilizing a range of techniques, dosages, and timing of administration. The therapeutic effects of MSC treatment on lung function were demonstrated by reductions in the mean linear intercept, decreased pulmonary epithelial cell apoptosis, and improvements in the structural integrity of injured lung tissue [87,88,89,90]. The cell-based approach to regenerative medicine posits that MSC transplantation promotes the repair of lung injury because it introduces healthy cells that function in the structural and functional regeneration of damaged or diseased lung tissue (i.e., cell replacement or implantation), or because the paracrine effects of MSCs promote endogenous regeneration and repair [64]. Studies of different types of lung injuries showed that systemic or direct injection of airways with MSCs successfully introduced these cells into rodent lungs, but most of these studies found that the population of cells implanted in the lungs was too low to be physiologically or functionally significant. Instead, the therapeutic effects of these cells were attributed to paracrine signaling. In fact, many studies found that MSCs can decrease systemic inflammation and stimulate the production of diverse anti-inflammatory molecules [75]. Additionally, MSCs can stimulate the proliferation of different cell types within the lungs, thereby facilitating endogenous repair of lung tissue [91, 92]. Some research showed that MSCs can attract native stem cells to the injury site and promote their differentiation, thereby initiating the regeneration of epithelial tissue [93]. Despite the many research findings supporting the potential efficacy of MSCs in the treatment of respiratory and degenerative disorders, there is still an incomplete understanding of the precise mechanisms by which they decrease lung inflammation and facilitate organ recovery. It seems likely that the type of stem cell and the nature of the injury or disease determines the mechanism, which may include direct differentiation into different cell types, immunomodulation, activation of paracrine pathways, and increasing antiapoptotic activity [74, 94,95,96,97] (Fig. 3).

Mechanisms of MSCs-based therapies for COPD. VEGF: vascular endothelial growth factor; HGF: hepatocyte-derived growth factor; Bcl-2: B cell lymphoma-2; Bax: Bcl-2-associated X protein; ROS: reactive oxygen species; TGF-β: transforming growth factor-β; MMPs: matrix metalloproteinases; ECM: extracellular matrix; IL: interleukin. By figdraw (www.figdraw.com)
Cell replacement of damaged lung tissues
MSCs have unique properties that make them suitable candidates for treatment of COPD. MSCs can differentiate into lung-specific cells and replace damaged or dead cells, increase the activity and regenerative potential of endogenous tissue-resident stem cells, promote regeneration of lung structures, improve the structural integrity of airways, and decrease airflow limitation and restore lung function [47]. Some in vitro studies shown that ESCs and adult stem cells can induce the expression of phenotype markers for airway and/or alveolar epithelial cells [98]. When administered intravenously, MSCs primarily target the lungs [99, 100]. Some research suggests that transplanted MSCs have an initial preference for the lungs before migrating to other organs, such as the liver [101]. Multiple studies have demonstrated that MSCs can engraft into mature differentiated airway and alveolar epithelial cells. AD-MSCs can differentiate into alveolar epithelial cells, thereby ameliorating lung injury in a murine model of elastase-induced emphysema [102]. Additionally, the implantation of BM-MSCs into the lungs of an animal model led to their differentiation into ATIICs and the inhibition of alveolar cell apoptosis, thereby preventing lung emphysema induced by radiation and papain protease [103]. The mechanisms underlying the recruitment of circulating or systemically administered stem cells or progenitor cells into the lungs have not yet been fully elucidated, but are likely to be influenced the age of both the donor and recipient, cell type, and route of administration. However, the current understanding suggests that exogenous stem cells have limited potential for structural repair or replacement of damaged lung epithelial cells, indicating the need for additional research to verify the potential of functional epithelial transplantation [104]. Recently, the concept of cell replacement or implantation has been revived. Implantation of basal-like airway epithelial progenitor cells, iPSC-derived lung epithelial cells, or embryonic stem cell-derived AT2 cells using alternative cell sources appears to provide potential therapeutic effect in regenerating damaged lung tissues [64].
Paracrine effects
In recent years, there has been growing interest in the paracrine effects of MSCs, and the secretome of MSCs has emerged as a potential alternative to cell therapy for various lung diseases. Schweitzer et al. demonstrated that AD-MSCs had therapeutic effects on lung and systemic injuries induced by cigarette smoke, such as lung airway dilation, weight loss, and bone marrow suppression, and proposed that paracrine factors released by AD-MSCs were responsible for these effects [105]. Shigemura et al. validated that the reparative potential of AD-MSCs in treating emphysema was mediated by secretion of hepatocyte growth factor, and this intervention led to improved gas exchange and enhanced exercise tolerance [91]. Hence, there is great interest in the MSC-mediated mechanism of lung tissue repair and the role of paracrine activity in this process. The secretome of MSCs, which includes conditioned medium (CM) and extracellular vesicles (EVs), has immunomodulatory effects and decreases inflammation in pulmonary airways [106].
MSC-CM is readily accessible and regarded as minimally manipulated cell-free material derived from MSCs. There is evidence that administration of MSC-CM leads to a significant reduction in the severity of lung injury, and had efficacy comparable to MSCs in various in vitro and in vivo animal models. For example, Shologu et al. studied CM from BM-MSCs and AD-MSCs, and examined its effect on low-oxygen-induced lung epithelial injury in alveolar epithelial cells. Their findings indicated that MSC-CM improved alveolar epithelial cell viability, decreased the secretion of proinflammatory mediators, and increased the production of the anti-inflammatory cytokine IL-10 [107]. Other studies evaluated the therapeutic efficacy of MSC-CM in a rodent model of COPD induced by cigarette smoke exposure, and the results suggested that MSC and MSC-CM lead to a notable decrease in emphysema and an increase in the quantity of pulmonary capillaries [108]. In addition to emphysema, cigarette smoke can also trigger apoptosis in lung fibroblasts. Thus, Kim et al. reported that MSC-CM mitigated the apoptosis of lung fibroblasts and promoted their proliferation in vivo and in vitro [109]. The findings of these many studies of lung injury models indicate a significant potential for utilization of MSC-CM for decreasing cell death and inflammatory reactions and for increasing tissue repair and endogenous regeneration.
EVs, which include proteins, mRNAs, miRNAs, long noncoding RNAs, and lipids, can regulate gene expression and modulate diverse pathways [110]. EVs are categorized as exosomes, microvesicles, or apoptotic bodies based on their origin, mechanism of secretion, size, and surface markers. A study in mice demonstrated that MSC-EVs decreased pulmonary fibrosis, restored lung structure, improved alveolar formation, and enhanced lung function [111]. MSCs-EVs presumably had these effects by transferring bioactive mediators to injured cells, thereby regulating pathological and physiological responses and promoting cell survival, while decreasing immune and inflammatory responses [112]. Thus, these recent preclinical studies of lung injury indicate that the secretome of MSCs, including CM and EVs, has promising therapeutic effects.
Conclusion
COPD is a common chronic respiratory disease, but current treatments cannot halt disease progression or significantly decrease mortality. Researchers in regenerative medicine have examined the potential for treating lung diseases using a variety of stem cell types, such as ESCs, iPSCs, and multiple types of MSCs. Considering the unavoidable limitations, ESCs and iPSCs are difficult to achieve clinical applications. The differentiation potential, aging status, and immunophenotype of MSCs are closely related to the extraction, storage, and clinical efficacy. In recent years, with the increasing maturity of stem cell isolation, culture and differentiation technologies, the limitations of MSCs have been properly resolved, making it possible to use MSCs for various tissue and organ repair and regeneration in the clinic. More and more preclinical and clinical studies have confirmed that MSCs do not only rely on direct cell-to-cell contact, but also secrete extracellular vesicles to exert therapeutic functions, such as immunomodulation, anti-inflammation, angiogenesis, antioxidant and anti-apoptosis.
In conclusion, there appears to be a promising future for the use of MSCs therapies for treatment of COPD. Future basic research, clinical trials, and interdisciplinary collaborations are needed to develop safe and effective stem cell-based therapies for COPD that improve patient prognosis and enhance quality-of-life.
Data availability
Not applicable.
Abbreviations
- CODP:
-
Chronic obstructive pulmonary disease
- MSCs:
-
Mesenchymal stem cells
- ESCs:
-
Embryonic stem cells
- iPSCs:
-
Induced pluripotent stem cells
- ATIICs:
-
Type II alveolar epithelial cells
- ATICs:
-
Type I alveolar epithelial cells
- HLAs:
-
Human leukocyte antigens
- BM-MSCs:
-
Bone marrow mesenchymal stem cells
- AD-MSCs:
-
Adipose tissue mesenchymal stem cells
- UC-MSCs:
-
Umbilical cord mesenchymal stem cells
- CM:
-
Conditioned medium
- EVs:
-
Extracellular vesicles
References
Celli B, Fabbri L. Definition and Nomenclature of Chronic Obstructive Pulmonary Disease: Time for Its Revision. 2022. 206(11): pp. 1317–1325.
Agustí A, Celli BR. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. 2023. 61(4).
Adeloye D, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–58.
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report. 2023.
Barnes PJ, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. 2015;1:15076.
Vlahos R, Bozinovski S. Role of alveolar macrophages in chronic obstructive pulmonary disease. Front Immunol. 2014;5:435.
Deng Y, et al. Integrated Phytochemical Analysis Based on UPLC-Q-TOF-MS/MS, Network Pharmacology, and Experiment Verification to explore the potential mechanism of Platycodon grandiflorum for chronic bronchitis. Front Pharmacol. 2020;11:564131.
Kim V, Criner GJ. Chronic bronchitis and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(3):228–37.
Lan Y, et al. Predifferentiated amniotic fluid mesenchymal stem cells enhance lung alveolar epithelium regeneration and reverse elastase-induced pulmonary emphysema. Stem Cell Res Ther. 2019;10(1):163.
Churg A, Cosio M, Wright JL. Mechanisms of cigarette smoke-induced COPD: insights from animal models. Am J Physiol Lung Cell Mol Physiol. 2008;294(4):L612–31.
Sharafkhaneh A, Hanania NA, Kim V. Pathogenesis of emphysema: from the bench to the bedside. Proc Am Thorac Soc. 2008;5(4):475–7.
Jones B, et al. Animal models of COPD: what do they tell us? Respirol (Carlton Vic). 2017;22(1):21–32.
Hogg J, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–53.
McGuinness AJ, Sapey E. Oxidative stress in COPD: sources, markers, and potential mechanisms. J Clin Med, 2017. 6(2).
Mecham R. Elastin in lung development and disease pathogenesis. Matrix Biology: J Int Soc Matrix Biology. 2018;73:6–20.
Chillappagari S, et al. Altered protease and antiprotease balance during a COPD exacerbation contributes to mucus obstruction. Respir Res. 2015;16:85.
Pandey KC, De S, Mishra PK. Role of proteases in Chronic Obstructive Pulmonary Disease. Front Pharmacol. 2017;8:512.
Wise R. Changing smoking patterns and mortality from chronic obstructive pulmonary disease. Prev Med. 1997;26(4):418–21.
Mannino D. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest. 2002;121:S121–6.
Singh D, et al. Global strategy for the diagnosis, management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164.
Anthonisen NR, et al. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142(4):233–9.
Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–46.
Jin Z, et al. Biological effects and mechanisms of action of mesenchymal stem cell therapy in chronic obstructive pulmonary disease. J Int Med Res. 2015;43(3):303–10.
Moodley Y. Evidence for human lung stem cells. N Engl J Med. 2011;365(5):464. author reply 465-6.
Hoang DM, et al. Stem cell-based therapy for human diseases. Signal Transduct Target Ther. 2022;7(1):272.
Coppolino I, et al. Role of stem cells in the Pathogenesis of Chronic Obstructive Pulmonary Disease and Pulmonary Emphysema. COPD. 2018;15(5):536–56.
Shahbazi MN, Siggia ED. Self-organization of stem cells into embryos: a window on early mammalian development. 2019. 364(6444): pp. 948–51.
Yamanaka S. Pluripotent stem cell-based Cell Therapy-Promise and challenges. Cell Stem Cell. 2020;27(4):523–31.
Urbán N, Cheung TH. Stem cell Quiescence: Challenging path Activation 2021. 148(3).
Odorico JS, Kaufman DS, Thomson JA. Multilineage Differ Hum Embryonic stem cell Lines Stem Cells. 2001;19(3):193–204.
Damdimopoulou P, et al. Human embryonic stem cells. Best Pract Res Clin Obstet Gynaecol. 2016;31:2–12.
Ilic D, et al. Human embryonic and induced pluripotent stem cells in clinical trials. Br Med Bull. 2015;116:19–27.
Ali NN, et al. Derivation of type II alveolar epithelial cells from murine embryonic stem cells. Tissue Eng. 2002;8(4):541–50.
Rippon HJ, et al. Derivation of distal lung epithelial progenitors from murine embryonic stem cells using a novel three-step differentiation protocol. Stem Cells. 2006;24(5):1389–98.
Wang D, et al. A pure population of lung alveolar epithelial type II cells derived from human embryonic stem cells. Proc Natl Acad Sci U S A. 2007;104(11):4449–54.
Wang D, et al. Transplantation of human embryonic stem cell-derived alveolar epithelial type II cells abrogates acute lung injury in mice. Mol Ther. 2010;18(3):625–34.
Samadikuchaksaraei A, et al. Derivation of distal airway epithelium from human embryonic stem cells. Tissue Eng. 2006;12(4):867–75.
Van Vranken BE, et al. Coculture of embryonic stem cells with pulmonary mesenchyme: a microenvironment that promotes differentiation of pulmonary epithelium. Tissue Eng. 2005;11(7–8):1177–87.
Simon DM, Levin S. Infectious complications of solid organ transplantations. Infect Dis Clin North Am. 2001;15(2):521–49.
Penn I. Post-transplant malignancy: the role of immunosuppression. Drug Saf. 2000;23(2):101–13.
Wang D, et al. Targeted disruption of the β2-Microglobulin gene minimizes the immunogenicity of human embryonic stem cells. Stem Cells Transl Med. 2015;4(10):1234–45.
Shroff G. Human embryonic stem cells (hESCs) in the treatment of emphysematous COPD: a case report. Clin Case Rep. 2015;3(7):632–4.
Sun Z, et al. Stem cell therapies for chronic obstructive pulmonary disease: current status of pre-clinical studies and clinical trials. J Thorac Dis. 2018;10(2):1084–98.
Quan Y, Wang D. Clinical potentials of human pluripotent stem cells in lung diseases. Clin Transl Med. 2014;3:15.
Takahashi K, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell. 2007;131(5):861–72.
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663–76.
Singh PV, Singh PV, Anjankar A. Harnessing the therapeutic potential of stem cells in the management of Chronic Obstructive Pulmonary Disease: a Comprehensive Review. Cureus. 2023;15(8):e44498.
Altalhi W, et al. Intratracheally injected human-induced pluripotent stem cell-derived pneumocytes and endothelial cells engraft in the distal lung and ameliorate emphysema in a rat model. J Thorac Cardiovasc Surg. 2023;166(1):e23–37.
Jacob A, et al. Differentiation of human pluripotent stem cells into functional lung alveolar epithelial cells. Cell Stem Cell. 2017;21(4):472–e48810.
Romito A, Cobellis G. Pluripotent Stem Cells: Current Understanding and Future Directions. 2016. 2016: p. 9451492.
Manstein F, Ullmann K. High Density Bioprocess Hum Pluripotent stem Cells Metabolic Control silico Model. 2021;10(7):1063–80.
Moradi S, et al. Research and therapy with induced pluripotent stem cells (iPSCs): social, legal, and ethical considerations. Stem Cell Res Ther. 2019;10(1):341.
Goecke T et al. Unlocking Future: Pluripotent Stem Cell-Based Lung Repair 2024. 13(7).
Basma H, et al. Reprogramming of COPD lung fibroblasts through formation of induced pluripotent stem cells. Am J Physiol Lung Cell Mol Physiol. 2014;306(6):L552–65.
Yan Q, et al. A site-specific genetic modification for induction of pluripotency and subsequent isolation of derived lung alveolar epithelial type II cells. Stem Cells. 2014;32(2):402–13.
Sayed N, Wong WT, Cooke JP. Therapeutic transdifferentiation: can we generate cardiac tissue rather than scar after myocardial injury? Methodist Debakey Cardiovasc J. 2013;9(4):210–2.
Li F, et al. Diversity of epithelial stem cell types in adult lung. Stem Cells Int. 2015;2015:p728307.
Bertoncello I, McQualter JL. Lung stem cells: do they exist? Respirology. 2013;18(4):587–95.
Kotton DN, Morrisey EE. Lung regeneration: mechanisms, applications and emerging stem cell populations. Nat Med. 2014;20(8):822–32.
Wang Y, Meng Z. Autologous transplantation of P63(+) lung progenitor cells for chronic obstructive pulmonary disease therapy. 2024. 16(734): p. eadi3360.
Parekh KR, et al. Stem Cells lung Regeneration. 2020;319(4):C675–93.
Dominici M, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8(4):315–7.
Herberts CA, Kwa MS, Hermsen HP. Risk factors in the development of stem cell therapy. J Transl Med. 2011;9:29.
Stolk J, et al. Translating Basic Research into Safe and Effective Cell-based treatments for respiratory diseases. Am J Physiol Lung Cell Mol Physiol. 2019;16(6):657–68.
Zuk P, et al. Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng. 2001;7(2):211–28.
‘t Anker P, et al. editors. Isolation of mesenchymal stem cells of fetal or maternal origin from human placenta. Stem cells (Dayton, Ohio), 2004. 22(7): pp. 1338-45.
Erices A, Conget P, Minguell J. Mesenchymal progenitor cells in human umbilical cord blood. Br J Haematol. 2000;109(1):235–42.
Troyer D, Weiss M. Wharton’s jelly-derived cells are a primitive stromal cell population. Stem Cells. 2008;26(3):591–9.
Gronthos S, et al. Stem cell properties of human dental pulp stem cells. J Dent Res. 2002;81(8):531–5.
Kopen G, Prockop D, Phinney D. Marrow stromal cells migrate throughout forebrain and cerebellum, and they differentiate into astrocytes after injection into neonatal mouse brains. Proc Natl Acad Sci USA. 1999;96(19):10711–6.
Pittenger M, et al. Multilineage potential of adult human mesenchymal stem cells. Volume 284. New York, N.Y.): Science; 1999. pp. 143–7. 5411.
Wecht S, Rojas M. Mesenchymal stem cells in the treatment of chronic lung disease. Respirol (Carlton Vic). 2016;21(8):1366–75.
Cappetta D, De Angelis A. Lung Mesenchymal Stem Cells Ameliorate Elastase-Induced Damage in an Animal Model of Emphysema. 2018. 2018: p. 9492038.
Katsha A, et al. Paracrine factors of multipotent stromal cells ameliorate lung injury in an elastase-induced emphysema model. Mol Therapy: J Am Soc Gene Therapy. 2011;19(1):196–203.
Gu W, et al. Mesenchymal stem cells alleviate airway inflammation and emphysema in COPD through down-regulation of cyclooxygenase-2 via p38 and ERK MAPK pathways. Sci Rep. 2015;5:8733.
Cruz F, Rocco P. The potential of mesenchymal stem cell therapy for chronic lung disease. Expert Rev Respir Med. 2020;14(1):31–9.
Kim M, et al. CD26 inhibition potentiates the therapeutic effects of Human umbilical cord blood-derived mesenchymal stem cells by delaying Cellular Senescence. Cell Mol Life Sci. 2021;9:803645.
Ribeiro-Paes JT, et al. Unicentric study of cell therapy in chronic obstructive pulmonary disease/pulmonary emphysema. Int J Chron Obstruct Pulmon Dis. 2011;6:63–71.
Weiss DJ, et al. A placebo-controlled, randomized trial of mesenchymal stem cells in COPD. Chest. 2013;143(6):1590–8.
Stolk J, et al. A phase I study for intravenous autologous mesenchymal stromal cell administration to patients with severe emphysema. QJM. 2016;109(5):331–6.
Bateman M, et al. Concise Review: using Fat to Fight Disease: a systematic review of Nonhomologous adipose-derived Stromal/Stem cell therapies. Stem Cells. 2018;36(9):1311–28.
Cheng H, et al. Replicative senescence of human bone marrow and umbilical cord derived mesenchymal stem cells and their differentiation to adipocytes and osteoblasts. Mol Biol Rep. 2011;38(8):5161–8.
Gimble J, Katz A, Bunnell B. Adipose-derived stem cells for regenerative medicine. Circul Res. 2007;100(9):1249–60.
Kern S, et al. Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells. 2006;24(5):1294–301.
Strioga M, et al. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev. 2012;21(14):2724–52.
Hoang VT, et al. Standardized xeno- and serum-free culture platform enables large-scale expansion of high-quality mesenchymal stem/stromal cells from perinatal and adult tissue sources. Cytotherapy. 2021;23(1):88–99.
Guan X, et al. Mesenchymal stem cells protect cigarette smoke-damaged lung and pulmonary function partly via VEGF-VEGF receptors. J Cell Biochem. 2013;114(2):323–35.
Antunes MA, et al. Mesenchymal stem cell trials for pulmonary diseases. J Cell Biochem. 2014;115(6):1023–32.
Huh J, et al. Bone marrow cells repair cigarette smoke-induced emphysema in rats. Am J Physiol Lung Cell Mol Physiol. 2011;301(3):L255–66.
Chen Y, et al. Mesenchymal stem cell-based HSP70 promoter-driven VEGFA induction by resveratrol alleviates elastase-induced emphysema in a mouse model. Cell Stress Chaperones. 2015;20(6):979–89.
Shigemura N, et al. Autologous transplantation of adipose tissue-derived stromal cells ameliorates pulmonary emphysema. Am J Transplantation: Official J Am Soc Transplantation Am Soc Transpl Surg. 2006;6(11):2592–600.
Zhao Y, et al. Bone marrow mesenchymal stem cell transplantation for treatment of emphysemic rats. Int J Clin Exp Med. 2014;7(4):968–72.
Newman R, et al. Treatment of inflammatory diseases with mesenchymal stem cells. Inflamm Allergy Drug Targets. 2009;8(2):110–23.
Han I, et al. Differentiation potential of mesenchymal stem cells is related to their intrinsic Mechanical properties. Int Neurourol J. 2017;21:S24–31.
D’Agostino B, et al. Mesenchymal stem cell therapy for the treatment of chronic obstructive pulmonary disease. Expert Opin Biol Ther. 2010;10(5):681–7.
Cruz F, Rocco P. Stem-cell extracellular vesicles and lung repair. Stem cell Invest. 2017;4:78.
Antunes M, et al. Effects of different mesenchymal stromal cell sources and delivery routes in experimental emphysema. Respir Res. 2014;15:118.
Weiss DJ, et al. Stem cells and cell therapies in lung biology and lung diseases. Proc Am Thorac Soc. 2008;5(5):637–67.
Zhang J, et al. Evidence that bone marrow-derived mesenchymal stem cells reduce epithelial permeability following phosgene-induced acute lung injury via activation of wnt3a protein-induced canonical wnt/β-catenin signaling. Inhal Toxicol. 2016;28(12):572–9.
Li JW, et al. Mesenchymal stromal cells-derived exosomes alleviate ischemia/reperfusion injury in mouse lung by transporting anti-apoptotic miR-21-5p. Eur J Pharmacol. 2019;852:68–76.
Gao J, et al. The dynamic in vivo distribution of bone marrow-derived mesenchymal stem cells after infusion. Cells Tissues Organs. 2001;169(1):12–20.
Fukui E, et al. Adipose tissue-derived stem cells have the ability to differentiate into alveolar epithelial cells and ameliorate Lung Injury caused by Elastase-Induced Emphysema in mice. Stem Cells Int. 2019;2019:p5179172.
Zhen G, et al. Mesenchymal stem cells transplantation protects against rat pulmonary emphysema. Front Biosci. 2008;13:3415–22.
Sueblinvong V, Weiss DJ. Cell therapy approaches for lung diseases: current status. Curr Opin Pharmacol. 2009;9(3):268–73.
Schweitzer K, et al. Adipose stem cell treatment in mice attenuates lung and systemic injury induced by cigarette smoking. Am J Respir Crit Care Med. 2011;183(2):215–25.
Shologu N et al. Human mesenchymal stem cell secretome from bone marrow or adipose-derived tissue sources for treatment of Hypoxia-Induced Pulmonary Epithelial Injury. Int J Mol Sci, 2018. 19(10).
Wang G, et al. Adult stem cells from bone marrow stroma differentiate into airway epithelial cells: potential therapy for cystic fibrosis. Proc Natl Acad Sci U S A. 2005;102(1):186–91.
Huh JW, et al. Bone marrow cells repair cigarette smoke-induced emphysema in rats. Am J Physiol Lung Cell Mol Physiol. 2011;301(3):L255–66.
Kim SY, et al. Mesenchymal stem cell-conditioned media recovers lung fibroblasts from cigarette smoke-induced damage. Am J Physiol Lung Cell Mol Physiol. 2012;302(9):L891–908.
Cruz FF, Rocco PRM. Stem-cell extracellular vesicles and lung repair. Stem Cell Investig. 2017;4:78.
Kamada Y, et al. Transplantation of basic fibroblast growth factor-pretreated adipose tissue-derived stromal cells enhances regression of liver fibrosis in mice. Am J Physiol Gastrointest Liver Physiol. 2009;296(2):G157–67.
Mohammadipoor A, et al. Therapeutic potential of products derived from mesenchymal stem/stromal cells in pulmonary disease. Respir Res. 2018;19(1):218.
Acknowledgements
The authors declare that artificial intelligence is not used in this study.
Funding
This work was supported by the grants from Natural Science Foundation of Fujian Province, China (2022J01272), the Startup Fund for Scientific Research of Fujian Medical University (2021QH1115).
Author information
Authors and Affiliations
Contributions
SL wrote the manuscript; SL and ZG edited the manuscript and designed the figures. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lai, S., Guo, Z. Stem cell therapies for chronic obstructive pulmonary disease: mesenchymal stem cells as a promising treatment option. Stem Cell Res Ther 15, 312 (2024). https://doi.org/10.1186/s13287-024-03940-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13287-024-03940-9