
Abstract
Background
The optimal timing of weaning from venovenous extracorporeal membrane oxygenation (VV ECMO) and its modalities have been rarely studied.
Methods
Retrospective, multicenter cohort study over 7 years in two tertiary ICUs, high-volume ECMO centers in France and Italy. Patients with ARDS on ECMO and successfully weaned from VV ECMO were classified based on their mechanical ventilation modality during the sweep gas-off trial (SGOT) with either controlled mechanical ventilation or spontaneous breathing (i.e. pressure support ventilation). The primary endpoint was the time to successful weaning from mechanical ventilation within 90 days post-ECMO weaning.
Results
292 adult patients with severe ARDS were weaned from controlled ventilation, and 101 were on spontaneous breathing during SGOT. The 90-day probability of successful weaning from mechanical ventilation was not significantly different between the two groups (sHR [95% CI], 1.23 [0.84–1.82]). ECMO-related complications were not statistically different between patients receiving these two mechanical ventilation strategies. After adjusting for covariates, older age, higher pre-ECMO sequential organ failure assessment score, pneumothorax, ventilator-associated pneumonia, and renal replacement therapy, but not mechanical ventilation modalities during SGOT, were independently associated with a lower probability of successful weaning from mechanical ventilation after ECMO weaning.
Conclusions
Time to successful weaning from mechanical ventilation within 90 days post-ECMO was not associated with the mechanical ventilation strategy used during SGOT. Further research is needed to assess the optimal ventilation strategy during weaning off VV ECMO and its impact on short- and long-term outcomes.
Similar content being viewed by others


Background
The rationale for venovenous extracorporeal membrane oxygenation (V-V ECMO) utilization is to ensure adequate gas exchange while allowing ventilator settings that enhance ventilator-induced lung injury (VILI) prevention, a key contributor to morbidity and mortality in acute respiratory distress syndrome (ARDS) [1]. The evidence supporting the use of ECMO is becoming more robust, as demonstrated in multicenter clinical trials [2, 3], bayesian analysis [4], and meta-analyses [5,6,7]. On these bases, the latest European guidelines on ARDS recommend V-V ECMO utilization in high-volume centers [8]. However, there are still pending research questions in that field, especially on the timing and the modalities of ECMO weaning. Once the lung function has sufficiently recovered [2, 9], the sweep gas flow is turned off, and the patient’s oxygenation and decarboxylation are both closely monitored for 6–24 h to assess the ability to be decannulated and liberated from V-V ECMO [9]. However, the optimal timing of this weaning trial and its modalities have not been well standardized and are mainly based on clinician preferences and expert opinion [10,11,12,13]. Indeed, two specific periods for ECMO weaning could be identified. Early weaning from V-V ECMO, when the patient is still on controlled ventilation with deep sedation, could reduce the risks of ECMO-related complications and costs. However, this approach may jeopardize the prevention of VILI and expose the patients to the need for a new ECMO run [13, 14]. On the other hand, waiting for an awake patient capable of breathing spontaneously on V-V ECMO may necessitate time [15]. This strategy could theoretically prolong the duration of ECMO, thereby increasing the patient's vulnerability to ECMO-related complications. On the other hand, it may also be associated with multiple physiological benefits, such as improved ventilation-perfusion matching, preserved respiratory muscle function, and decreased need for sedatives [16]. If this can be achieved while maintaining adequate control of the respiratory drive, it may favor lung healing and thereby facilitate liberation from ECMO. To date, the impact of different ventilation strategies during ECMO weaning on outcomes has been poorly investigated, although some authors have recently outlined ventilatory and clinical parameters that can predict unfavorable outcomes [14, 17]. Furthermore, the decision to discontinue ECMO or mechanical ventilation first is still a matter of debate [18, 19].
The objectives of this multicenter, retrospective study were (1) to describe the mechanical ventilation settings used at the time of V-V ECMO weaning in two experienced ECMO centers; (2) to compare two different approaches during the weaning process, namely controlled mechanical ventilation versus spontaneous assisted breathing, in terms of mechanical ventilation duration, ICU and hospital lengths of stay, and mortality after ECMO weaning.
Methods
Study design and patients
This study retrospectively included patients with severe ARDS (according to the Berlin Definition [20]) treated with ECMO in two university tertiary medical centers between January 2015 and December 2022. The medical ICUs from Pitié-Salpêtrière Hospital, Paris, and IRCCS San Gerardo dei Tintori Hospital, Monza, are among the largest and the most experienced ECMO centers in France and Italy, respectively. All consecutive patients with ARDS who received V-V ECMO or other ECMO settings (i.e., veno-arterial, V-A, or veno-arteriovenous, V-AV) during the study period were screened. Only patients weaned alive from V-V ECMO were included in this study. The exclusion criteria were no intubation on ECMO, bridge to lung transplant, or extubated before ECMO weaning.
Following ethical standards of local Institutional Review, no informed consent was required for this retrospective, observational study. The National Commission for Informatics and Liberties (no. 2217028v0) and the Comitato Etico Brianza (ref. NP3369) approved the data collection for this study.
Management of sedation and mechanical ventilation during ECMO
Deep intravenous (propofol or midazolam) or volatile (isoflurane [21]) sedation was maintained in the early phase of the disease (i.e. Richmond Agitation-Sedation Scale (RASS) [22] ≤ − 3), with the addition of neuromuscular blockade in case of patient-ventilator asynchronies. Light sedation (− 2 ≤ RASS ≤ − 1) with either a low dose of propofol or dexmedetomidine was used when the clinical condition was improving. The ventilation strategies used generally followed the EOLIA protocol [2]. Ultraprotective ventilation was provided either by volume or pressure-control modality, with a tidal volume of 6 ml/kg or below, adjusted to maintain a driving pressure below 15 cmH2O. Positive end-expiratory pressure was set at 10 cmH2O or more, and the respiratory rate was maintained between 10 and 20 cycles/min.
Sweep gas-off trial (SGOT)
The ventilatory and blood gas parameters at the end of the sweep gas-off trial (SGOT) that preceded the liberation from ECMO were recorded. The SGOT trial consisted of turning off the sweep gas flow while maintaining ECMO blood flow > 3 L/min, to avoid clotting [9]. The test duration ranges from 6 to 12 h (i.e. Monza, Italy) to 24 h (i.e. Paris, France) and aims to emulate gas exchanges with mechanical ventilation only. Based on lung function improvement, respiratory mechanics, and gas exchanges [9], the clinician in charge of the patient decided to perform an SGOT on controlled mechanical ventilation or spontaneous breathing with pressure support. Based on these mechanical ventilation modalities at the time of SGOT, patients were classified as Controlled Ventilation Group (i.e. patients who underwent the trial either on Volume-Control Ventilation, Pressure-Control Ventilation, Airway Pressure Release Ventilation, or Pressure-Control Bi-Level Positive Airway Pressure) or Spontaneous Breathing Group (i.e. patients on pressure support ventilation during the SGOT). Successful weaning criteria, including lung mechanics and gas exchanges, according to mechanical ventilation modalities during SGOT have been described elsewhere [2, 23] and are reported in Additional file 1.
Data collection
We collected data before ECMO implantation and at the time of ECMO weaning. Pre-ECMO ventilation settings and blood gas, Sepsis-related Organ Failure Assessment (SOFA) score, need for renal replacement therapy (RRT), cause of ARDS (i.e., viral pneumonia, bacterial pneumonia, autoimmune cause, or others), adjunct therapies before ECMO start, and ECMO management were also reported. The ventilation settings and the blood gas parameters were collected right before VV ECMO implantation. The SOFA score was intended as the one at the admission to the ECMO unit.
Outcome variables
The primary outcome was the time to successful weaning from mechanical ventilation within 90 days following ECMO discontinuation. Successful weaning from mechanical ventilation was defined as the removal of the endotracheal tube or tracheostomy cannula (for tracheostomized patients) without the need for reintubation in the following 72 h. Death or new ECMO run within 90 days after ECMO weaning were considered as competing events. Secondary outcomes were ventilator-associated pneumonia (VAP), ICU and hospital length of stay and mortality. VAP was diagnosed in patients who were on mechanical ventilation for at least 48 h and showed significant quantitative growth (≥ 104 colony-forming units (CFU)/mL) of at least one pathogen in the Broncho-Alveolar Lavage fluid sample [24, 25].
Statistical analyses
This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations for reporting cohort studies [26]. No power calculation or sample size computation was performed.
Baseline characteristics are reported as proportions (%) for categorical variables and as median [interquartile range, IQR] for continuous variables. The primary endpoint was the time to successful mechanical ventilation weaning within the 90 days following ECMO weaning, in the presence of the competing risks of death and second ECMO run according to the two mechanical ventilation groups. Day 0 of mechanical ventilation was considered as the date of ECMO weaning. The cumulative incidence curves for these competing events were drawn for each group. The cumulative incidence of successful mechanical ventilation weaning was compared between groups using a Gray test. The subdistribution hazard ratios (sHR) were estimated (with their 95% confidence interval, CI) for the competing events using a Fine and Gray competing risk regression. Baseline variables (i.e., obtained at the time of ECMO start) and ECMO weaning variables (i.e., obtained at the time of ECMO weaning) included in the multivariable model were defined a priori based on the available literature. Baseline variables included age, body mass index, COVID-19-related ARDS (yes/no), pre-ECMO PaO2/FiO2, and pre-ECMO SOFA. ECMO weaning variables were ventilation mode and compliance of the respiratory system at the time of the SGOT, ECMO duration, prone positioning on ECMO, VAP, pneumothorax, and renal replacement therapy before the SGOT. No imputation for missing data was performed. Log linearity was graphically assessed for the quantitative variable’s effects using restricted cubic splines. Additionally, a sensitivity analysis was performed for the subgroup of patients with COVID-19.
Categorical outcomes were compared with chi-square or Fisher’s exact tests, and continuous outcomes with Student’s t-test or Wilcoxon’s test, as appropriate. All analyses were conducted at the two-sided α risk of 5%. All analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria), version 4.1.3.
Results
Study population
The study flowchart is presented in Fig. 1. Of 603 patients receiving VV ECMO primarily for ARDS during the 7-year study period, 390 (median age 50 (IQR 41; 57) years) underwent a successful ECMO weaning and were included in our study. Two hundred and ninety-two (75%) patients had an SGOT on Controlled Ventilation whereas 98 (25%) were on Spontaneous Breathing. The baseline and pre-ECMO characteristics of these two study groups are reported in Table 1. Briefly, patients in the controlled ventilation group were significantly younger, had a higher body mass index, and were more frequently retrieved on ECMO to the two referral centers. The most frequent comorbidities were hypertension, diabetes, and chronic respiratory disease. Notably, 27 (7%) patients were immunocompromised at cannulation. The main cause of ARDS was COVID-19 in both groups, followed by bacterial pneumonia and viral non-COVID pneumonia. Patients in the controlled ventilation group had a significantly longer time between mechanical ventilation and ECMO than those in the spontaneous breathing group (3 [1–6] vs 1 [1–5] days, respectively, p = 0.004) and showed a lower Pre-ECMO PaO2/FiO2 ratio and a higher PaCO2. Pre-ECMO lung mechanics were more severe in the controlled ventilation group, with a significantly lower PEEP, a higher plateau pressure and respiratory rate, and a lower tidal volume. In this subgroup, before ECMO implementation, nitric oxide, and prone positioning were used more frequently. On the other hand, neuromuscular blockades were used similarly in both groups (Table 1).

Study flowchart. ARDS, acute respiratory distress syndrome; V-A, ECMO veno-arterial extracorporeal membrane oxygenation; V-V ECMO, venovenous extracorporeal membrane oxygenation
Characteristics during the SGOT
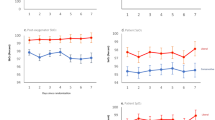
The characteristics and lung mechanics at the time of SGOT are presented in Table 2. At the time of SGOT, patients were on ECMO for 13 [7–29] and 12 [9–18] days (p = 0.398) in the controlled ventilation and the spontaneous breathing groups, respectively. When compared to patients in the spontaneous breathing group, patients in the controlled ventilation group had a significantly lower tidal volume, PEEP, and higher respiratory rate. Similarly, lower static respiratory system compliance and higher plateau pressure and driving pressure were reported in the controlled ventilation group.
Primary and secondary outcomes
The probability of successful weaning from mechanical ventilation within 90 days of ECMO discontinuation was not significantly different between the two groups (sHR, 1.23 [95% CI 0.84–1.82], p = 0.301) (Fig. 2). Death or a second ECMO run, the competing component of the primary outcome, was not significantly different between groups (sHR, 1.13 [95% CI [0.33–3.88]), p = 0.802) (Fig. 2). Patients in the spontaneous breathing group had a lower unadjusted length of stay in the ICU and the hospital and lower hospital mortality after ECMO weaning. ECMO-related complications, such as severe bleeding or ischemic stroke were not different between the two groups. Ventilator-associated pneumonia was more frequently recorded in the controlled ventilation group (Table 3).

Cumulative incidence function for the events of mechanical ventilation successful weaning and death or second run of ECMO, according to mechanical ventilation modalities during sweep gas-off trial. sHR, subdistribution hazard ratio; MV, mechanical ventilation
After adjustment to the patient’s characteristics and events occurring during the ECMO run, being on spontaneous ventilation during SGOT was not associated with a greater probability of successful mechanical ventilation weaning. Conversely, older age, ventilator-associated pneumonia on ECMO, pneumothorax, and RRT in ICU were significantly associated with a lower probability of successful weaning from mechanical ventilation at 90 days. A shorter ECMO duration and greater static compliance during SGOT were associated with a significant increase in the probability of weaning from mechanical ventilation (Fig. 3). Moreover, similar risk factors for successful weaning from mechanical ventilation at 90 days were found when the analysis was performed for the subgroup of patients with COVID-19 (see Additional file 2).

Association of covariates with the 90-day adjusted probability of successful weaning from mechanical ventilation after ECMO decannulation in the multivariable model, expressed using sHR (points) with their 95% CI (error bars). sHR, subdistribution hazard ratio. The model was performed on 355 patients due to missing data
Discussion
This study investigated ventilatory modalities and subsequent outcomes in 390 patients weaned from V-V ECMO. The analysis revealed no significant difference in the rate of successful mechanical ventilation weaning after SGOT, accounting for death and the need for a second ECMO run as competing events. Despite similar ECMO duration, patients on spontaneous breathing during SGOT had a shorter ICU and hospital length of stay, when compared to patients on controlled mechanical ventilation. However, after adjusting for covariates, spontaneous breathing during SGOT was not independently associated with a higher probability of being weaned from mechanical ventilation, as compared to controlled ventilation. Noticeably, spontaneous breathing during ECMO weaning was not associated with a higher incidence of ECMO-related complications.
Strong evidence to guide mechanical ventilation settings during V-V ECMO is still lacking. Current recommendations rely on experts’ opinions and ventilatory settings used in the ECMO groups in two recent RCTs [2, 3, 9]. Ultra-protective lung ventilation settings could enhance VILI prevention on ECMO [27], as suggested in the LIFEGARDS study [28] and several reviews [23, 29, 30]. Nonetheless, the association between ventilatory parameters while on ECMO and outcomes has not been well established, with studies showing conflicting results [28, 31]. Literature regarding mechanical ventilation settings during ECMO weaning is even more scarce since this topic has received very little attention. Limited data offer guidance about when and how to perform an SGOT [10,11,12, 23, 32]. Al-Fares et al. demonstrated that patients exhibiting higher tidal volumes, heart rate, ventilatory ratio, and esophageal pressure swings during SGOT have a decreased likelihood of achieving a safe liberation from VV ECMO [14]. Similarly, Gerhardinger et al. recently identified higher respiratory rate and PaCO2 before SGOT as independent risk factors for ECMO weaning failure while, during the trial, impaired oxygenation was the most relevant risk factor of ECMO weaning failure [33]. A higher PaCO2 and respiratory rate at the time of ECMO decannulation were also associated with prolonged mechanical ventilation and ICU length of stay following decannulation, whereas high PEEP seemed protective [17]. Our multivariate analysis showed that pneumothorax, ventilation-associated pneumonia, and renal replacement therapy during ECMO, all surrogates of patient severity, were independently associated with a lower likelihood of being successfully weaned from mechanical ventilation at day 90.
The ECMO duration until SGOT was unexpectedly found to be not different between the two groups in our study. One could argue that waiting for patients to be able to undergo spontaneous breathing ventilation could expose them to a longer ECMO run and therefore greater likelihood of ECMO-related complications. Interestingly, severe bleeding and pneumothorax incidence were similar between the two groups. These findings are reassuring, suggesting that maintaining V-V ECMO support until being on spontaneous ventilation is not associated with worse outcomes compared to controlled mechanical ventilation. A weaning ECMO strategy that encourages spontaneous breathing before or during an SGOT may facilitate liberation from ECMO by the inherent physiological benefits of spontaneous breathing efforts, such as the recruitment of the dorsal-dependent lung regions. Moreover, as compared to using ultra-low tidal volumes (1–2 mL/kg of predicted body weight) alongside prolonged infusion of neuromuscular blockers, this approach might be associated with more favorable outcomes [34]. Additionally, it may reduce costs and resource consumption following decannulation.
Initially, we hypothesized that patients weaned from ECMO on spontaneous breathing would require a longer ECMO duration. However, our findings contradicted this hypothesis, as the ECMO durations in both study groups were similar. Nonetheless, the lower pre-ECMO severity in the spontaneous breathing group, which facilitated faster lung function improvement, might partially account for these results. Further investigation is still necessary to determine the optimal timing for SGOT. Noticeably, some patients may be "forced" to undergo the SGOT despite not fulfilling the respiratory mechanic prerequisites for ECMO weaning criteria, due to severe ECMO complications or a lack of clinical improvement after a prolonged ECMO course [35].
Although it is to date the largest study on mechanical ventilation modalities during SGOT, we acknowledge that our study has several limitations. First, given its retrospective design, it is not possible to establish direct causal relationships, but only associations. Furthermore, for the same reason, some potentially important data might be missing. For instance, we did not have access to the data regarding the timing and number of previous failed SGOTs before the one preceding the liberation from ECMO. The ventilatory modes used at those times were not collected. Similarly, the surrogates of the respiratory drive (e.g., P0.1, delta Pocc, and Pressure-Muscle-Index) at the time of SGOT, which were recorded in the spontaneous breathing group, have not been collected as well. Second, we included patients from two distinct ECMO centers where ECMO practices may slightly differ (e.g., ECMO cannulation sites, and mode of ventilation during ECMO weaning…). Unfortunately, a Fine and Gray model with a random effect on the center does not exist to date. Notably, spontaneous breathing at the SGOT was the preferred modality at San Gerardo Hospital, while controlled mechanical ventilation was mainly used at La Pitié-Salpêtrière Hospital. Third, we did not collect data regarding the use of adjunct therapies for ARDS post-ECMO weaning in both groups, which may also have an important impact on economic and human resources. Fourth, we did not gather information on the level of sedation, neuromuscular blockade use, and fluid balance during the ECMO course, which may have significantly impacted the study outcomes. Lastly, our follow-up was limited to 90 days after ECMO weaning. Exploring the impact of these ventilation strategies on long-term lung function or psychological status could be valuable.
Conclusion
A strategy comprising spontaneous breathing during SGOT was not associated with a higher incidence of successful weaning from mechanical ventilation, compared to controlled mechanical ventilation. However, this approach appears to be safe and not associated with more ECMO-related complications. Further research is needed to assess the optimal ventilation strategy during weaning off V-V ECMO and its impact on short- and long-term outcomes.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- COVID-19:
-
Coronavirus disease 2019
- ECMO:
-
Extracorporeal membrane oxygenation
- FiO2:
-
Fraction of inspired oxygen
- IBW:
-
Ideal body weight
- ICU:
-
Intensive care unit
- MV:
-
Mechanical ventilation
- PaO2:
-
Partial pressure of alveolar oxygen
- PBW:
-
Predicted Body Weight
- PEEP:
-
Positive end-expiratory pressure
- SAPS II:
-
Simplified Acute Physiology Score II
- SARS-CoV-2:
-
Severe acute respiratory distress syndrome coronavirus 2
- SOFA:
-
Sequential Organ Failure Assessment
- SpO2:
-
Oxygen saturation measured by pulse oximetry
References
Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369:2126–36.
Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378:1965–75.
Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. The Lancet. 2009;374:1351–63.
Goligher EC, Tomlinson G, Hajage D, Wijeysundera DN, Fan E, Jüni P, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome and posterior probability of mortality benefit in a post hoc Bayesian analysis of a randomized clinical trial. JAMA. 2018;320:2251.
Munshi L, Walkey A, Goligher E, Pham T, Uleryk EM, Fan E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis. Lancet Respir Med. 2019;7:163–72.
Combes A, Peek GJ, Hajage D, Hardy P, Abrams D, Schmidt M, et al. ECMO for severe ARDS: systematic review and individual patient data meta-analysis. Intensive Care Med. 2020;46:2048–57.
Brodie D, Slutsky AS, Combes A. Extracorporeal life support for adults with respiratory failure and related indications: a review. JAMA. 2019;322:557.
Grasselli G, Calfee CS, Camporota L, Poole D, Amato MBP, Antonelli M, et al. ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med. 2023;49:727–59.
Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): Guideline from the extracorporeal life support organization (ELSO). ASAIO J. 2021;67:601–10.
Broman LM, Malfertheiner MV, Montisci A, Pappalardo F. Weaning from veno-venous extracorporeal membrane oxygenation: how I do it. J Thorac Dis. 2018;10:S692–7.
Vasques F, Romitti F, Gattinoni L, Camporota L. How I wean patients from veno-venous extra-corporeal membrane oxygenation. Crit Care. 2019;23:316.
Gattinoni L, Vassalli F, Romitti F, Vasques F, Pasticci I, Duscio E, et al. Extracorporeal gas exchange: when to start and how to end? Crit Care. 2019;23:203.
Teijeiro-Paradis R, Cherkos-Dawit T, Munshi L, Ferguson ND, Fan E. Liberation from venovenous extracorporeal membrane oxygenation for respiratory failure. CHEST. 2023.
Al-Fares AA, Ferguson ND, Ma J, Cypel M, Keshavjee S, Fan E, et al. Achieving safe liberation during weaning from VV-ECMO in patients with severe ARDS. Chest. 2021;160:1704–13.
Polo Friz M, Rezoagli E, Safaee Fakhr B, Florio G, Carlesso E, Giudici R, et al. Successful versus failed transition from controlled ventilation to pressure support ventilation in COVID-19 patients: a retrospective cohort study. Crit Care Explor. 2024;6: e1039.
Spinelli E, Mauri T, Lissoni A, Crotti S, Langer T, Albanese M, et al. Spontaneous breathing patterns during maximum extracorporeal CO2 removal in subjects with early severe ARDS. Respir Care. 2020;65:911–9.
Thiara S, Serpa Neto A, Burrell AJC, Fulcher BJ, Hodgson CL, for the EXCEL Study Investigators, the ANZICS-CTG and the International ECMO Network. Association of respiratory parameters at venovenous extracorporeal membrane oxygenation liberation with duration of mechanical ventilation and ICU length of stay: a prospective cohort study. Crit Care Explor. 2022;4:e0689.
Abrams D, Schmidt M, Pham T, Beitler JR, Fan E, Goligher EC, et al. Mechanical ventilation for acute respiratory distress syndrome during extracorporeal life support. research and practice. Am J Respir Crit Care Med. 2020;201:514–25.
Roncon-Albuquerque R, Gaião S, Vasques-Nóvoa F, Basílio C, Ferreira AR, Touceda-Bravo A, et al. Standardized approach for extubation during extracorporeal membrane oxygenation in severe acute respiratory distress syndrome: a prospective observational study. Ann Intensive Care. 2023;13:86.
Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA [Internet]. 2012 [cited 2023 Aug 31];307. Available from: https://doi.org/10.1001/jama.2012.5669
Grasselli G, Giani M, Scaravilli V, Fumagalli B, Mariani C, Redaelli S, et al. Volatile Sedation for acute respiratory distress syndrome patients on venovenous extracorporeal membrane oxygenation and ultraprotective ventilation. Crit Care Explor. 2021;3: e0310.
Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O’Neal PV, Keane KA, et al. The Richmond agitation-sedation scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338–44.
Combes A, Schmidt M, Hodgson CL, Fan E, Ferguson ND, Fraser JF, et al. Extracorporeal life support for adults with acute respiratory distress syndrome. Intensive Care Med. 2020;46:2464–76.
European Centre for Disease Prevention and Control. Surveillance of healthcare-associated infections in intensive care units: HAI Net ICU protocol, version 2.2. [Internet]. LU: Publications Office; 2017 [cited 2024 Jun 10]. Available from: https://doi.org/10.2900/833186
Chastre J, Luyt C-E. Does this patient have VAP? Intensive Care Med. 2016;42:1159–63.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet. 2007;370:1453–7.
Rozencwajg S, Guihot A, Franchineau G, Lescroat M, Bréchot N, Hékimian G, et al. Ultra-protective ventilation reduces biotrauma in patients on venovenous extracorporeal membrane oxygenation for severe acute respiratory distress syndrome*. Crit Care Med. 2019;47:1505–12.
Schmidt M, Pham T, Arcadipane A, Agerstrand C, Ohshimo S, Pellegrino V, et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome. an international multicenter prospective cohort. Am J Respir Crit Care Med. 2019;200:1002–12.
Schmidt M, Pellegrino V, Combes A, Scheinkestel C, Cooper D, Hodgson C. Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care. 2014;18:203.
Assouline B, Combes A, Schmidt M. Setting and monitoring of mechanical ventilation during venovenous ECMO. Crit Care. 2023;27:95.
The ReVA Research Network and the PROVE Network Investigators, Serpa Neto A, Schmidt M, Azevedo LCP, Bein T, Brochard L, et al. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: a pooled individual patient data analysis: mechanical ventilation during ECMO. Intensive Care Med. 2016;42:1672–84.
Gannon WD, Stokes JW, Bloom S, Sherrill W, Bacchetta M, Rice TW, et al. Safety and feasibility of a protocolized daily assessment of readiness for liberation from venovenous extracorporeal membrane oxygenation. Chest. 2021;160:1693–703.
Gerhardinger F, Fisser C, Malfertheiner MV, Philipp A, Foltan M, Zeman F, et al. Prevalence and risk factors for weaning failure from venovenous extracorporeal membrane oxygenation in patients with severe acute respiratory insufficiency. Crit Care Med [Internet]. 2023 [cited 2023 Oct 15]; Available from: https://doi.org/10.1097/CCM.0000000000006041
Guervilly C, Fournier T, Chommeloux J, Arnaud L, Pinglis C, Baumstarck K, et al. Ultra-lung-protective ventilation and biotrauma in severe ARDS patients on veno-venous extracorporeal membrane oxygenation: a randomized controlled study. Crit Care. 2022;26:383.
Masi P, Tuffet S, Boyer L, Folliguet T, Mekontso Dessap A, De Prost N. Short and long-term outcomes of patients with COVID-19-associated acute respiratory distress syndrome and difficult veno-venous-ECMO weaning. Crit Care. 2021;25:337.
Acknowledgements
None.
Funding
Support was provided solely from institutional and/or departmental sources.
Author information
Authors and Affiliations
Contributions
MTP, MP, MG, and MS designed and coordinated the study. MTP and RG collected the patient’s data. MTP, MP, MG, and MS analyzed the patient’s data and wrote the manuscript. MP and MS did the statistical analysis. All authors contributed to drafting the manuscript or critically revised it for important intellectual content and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Following ethical standards of local Institutional Review, no informed consent was required for this retrospective, observational study. The National Commission for Informatics and Liberties (no. 2217028v0) and the Comitato Etico Brianza (ref. NP3369) approved the data collection for this study.
Consent for publication
Not applicable.
Competing interests
Matthieu Schmidt reports lecture fees from Getinge, Dräger, Baxter, and Fresenius Medical Care outside the submitted work. Alain Combes reports grants from Getinge, and personal fees from Getinge, Baxter, and Xenios outside the submitted work. The other authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Marco Giani and Matthieu Schmidt are co-senior authors.
Supplementary Information
Additional file 1.
Prerequisites for weaning trial, weaning trial protocol, and criteria for successful trial according to the two groups.
Additional file 2.
Association of covariates with the 90-day adjusted probability of successful weaning from mechanical ventilation after ECMO decannulation in the multivariable model analyzing the subgroup of COVID-19 patients, expressed using sHR with their 95% CI.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Passarelli, M.T., Petit, M., Garberi, R. et al. Mechanical ventilation settings during weaning from venovenous extracorporeal membrane oxygenation. Ann. Intensive Care 14, 138 (2024). https://doi.org/10.1186/s13613-024-01359-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-024-01359-2