
Abstract
Background
The crater lakes of Barombi Mbo and Barombi Kotto are well-known transmission foci of schistosomiasis and soil-transmitted helminthiasis having had several important control initiatives previously. To collect contemporary epidemiological information, a cross-sectional survey was undertaken inclusive of: signs and symptoms of disease, individual treatment histories, local water, sanitation and hygiene (WASH)-related factors and malacological surveillance, with molecular characterisation of specimens.
Methods
At each lake, a community cross-sectional survey was undertaken using a combination of stool and urine parasitological sampling, and interview with pro-forma questionnaires. A total of 338 children and adults participated. Material from snail and parasite species were characterised by DNA methods.
Results
Egg-patent prevalence of urogenital schistosomiasis was 8.7% at Barombi Mbo (all light-intensity infections) and 40.1% at Barombi Kotto (21.2% heavy-intensity infections). Intestinal schistosomiasis was absent. At Barombi Kotto, significantly more women reported signs and symptoms associated with female genital schistosomiasis. While there had been extensive recent improvement in WASH-related infrastructure at Barombi Mbo, water contact risk scores were higher among schistosomiasis-infected participants (P < 0.001) and at Barombi Kotto in general (P < 0.001). Across both lakes, mean prevalence of STH was very low (6.3%) evidencing an impressive decrease of 79.0% over the last decade; neither Strongyloides stercoralis nor Ascaris lumbricoides were found. A total of 29 freshwater sampling sites were inspected for snails, 13 in Barombi Mbo and 16 in Barombi Kotto; water chemistry differed significantly (P < 0.0001) between lakes for both mean pH (7.9 v. 9.6) and mean conductivity (64.3 μS v. 202.1 μS) respectively. Only two Bulinus camerunensis found on the central island of Barombi Kotto were observed to shed schistosome cercariae, but schistosome DNA was later detected in Bulinus sampled from both lakes as well as in Indoplanorbis exustus, an invasive species from Asia.
Conclusions
STH is currently at very low levels while urogenital schistosomiasis is of greatest concern at Barombi Kotto. This assessment highlights a unique opportunity for further study of the epidemiological dynamics at these crater lakes, to evaluate future intensified interventions both in terms of gaining and sustaining control at Barombi Kotto or in moving towards local interruption of transmission of both diseases at Barombi Mbo.
Similar content being viewed by others

Multilingual abstracts
Please see Additional file 1 for translations of the abstract into five official working languages of the United Nations.
Background
There are several neglected tropical diseases (NTDs) endemic throughout Cameroon that pose a significant threat to the well-being of the populace, estimated to be just over 20 million people [1]. Coordinated at the national level by the Ministry of Public Health, there are ongoing interventions against NTDs, especially those amenable to preventive chemotherapy, such as trachoma [2], lymphatic filariasis [3] and onchocerciasis [4]. With regard to schistosomiasis and soil-transmitted helminthiasis (STH), previous mapping initiatives have described the distributions of diseases [5–12]. It has been identified that more than two million people have schistosomiasis infection, and a further five million live in high transmission areas within the country [13]. The focus of efforts today is upon integrated mass drug administration (MDA) with praziquantel and mebendazole, primarily targeted to children of school-age along with education and social mobilisation [13]; where resources have permitted, inter-sectoral actions have improved water, sanitation and hygiene (WASH) factors at a variety of locations [14–17].
Three species of human schistosome exist in Cameroon, with some unique features that include cross-specific interactions between Schistosoma mansoni and Schistosoma haematobium [18], variable performance of praziquantel treatment at mixed transmission foci [19] and hybridization between Sc. haematobium and Schistosoma guineensis [20]. The competitive exclusion of the latter species [21] has been the subject of long-term studies in the field [22–24] and in the laboratory [20, 25, 26]. Furthermore, multidisciplinary studies on the transmission of urogenital schistosomiasis have also included medical malacology [27–30] as well as implementation of local snail control with focal molluscicides [31]. This was pioneered by Brian Duke and Peter Moore some 40 years ago [32–34] in the crater lakes Barombi Mbo and Barombi Kotto, located near Kumba in South-West, Cameroon (see Fig. 1) in seminal attempts to control urogenital schistosomiasis [35]. The prevalence of egg-patent infection with Sc. haematobium at these lakes was originally reported by Zahra in 1953 to be 91.0% Barombi Mbo and 76.0% Barombi Kotto [36].

Sketch map of South West Cameroon with the crater lakes of Barombi Mbo and Barombi Kotto depicted
Soil-transmitted helminths are also endemic in Cameroon; a study from 2010 revealed an overall STH prevalence of 46.2% in the South-West Region, with trichuriasis having highest prevalence (32.9%), followed by ascariasis (24.3%) and hookworm (15.0%) [37, 38]. The distribution of other STHs such as threadworm (Strongyloides spp.) remain poorly described. However, Strongyloides stercoralis has been noted within a HIV-cohort [39] and in children within peri-urban areas of Kumba [40]; an area also noted for autochthonous cases of paragonimiasis. A related zoonotic threadworm, Strongyloides fulleborni has been found in helminthological surveys of forest monkeys of the genus Cercopithecus, animals either eaten as bush meat or raised as semi-domestic pets [41].
In November 2015, a multidisciplinary implementation research network entitled COUNTDOWN was formed to investigate and support the scale-up of interventions against NTDs [42]. On 9th October 2015, The COUNTDOWN programme was officially launched in Yaoundé by the Minister of Public Health, His Excellency André Mama Fouda [43]. Where appropriate, the programme is developing national strategies to expand preventive chemotherapy against schistosomiasis and STH, alongside assessing future opportunities to interrupt transmission locally. Given the historical significance of the crater lakes Barombi Mbo and Barombi Kotto [27, 32–34, 44], a contemporary situational comparison was undertaken at each lake, referencing previous parasitological data from in 2004, specifically with the aim of providing an epidemiological update at each lake. The three complementary objectives were to: (i) describe the prevalence and intensity of schistosomiasis (Sc. mansoni and Sc. haematobium infections) and STH (inclusive of St. stercoralis) in each community, (ii) assess disease associations with demography, reported morbidity and water, sanitation and hygiene (WASH) and (iii) document the distribution, abundance and infection status of encountered snails, alongside molecular characterisation of snails and schistosomes. Taken as a whole, this analysis will enable assessment of prospects for more intensified disease-control interventions and prioritisation of resources for further study.
Study design and methods
This cross-sectional study was conducted during June 2016 at Barombi Mbo (4°40′N 9°24′E) and Barombi Kotto (4°28′N 9°16′E), South-West Cameroon. As population census data were not available by village, a preliminary sample size (n = 270 across both sites) was based on an estimated prevalence of 50% from a survey near Kumba [15]; the sample sizes were then recalculated based on assessed population sizes in the field and local knowledge of differences in STH prevalence at each site (expected to be 50% versus 5% at either crater lake). A target sample size of 169 participants from Barombi Kotto and 87 from Barombi Mbo was set, powered to 95% with 5% precision.
Ethical approval and individual consent
Study protocols were approved by the Liverpool School of Tropical Medicine Research Ethics Committee (M1516-18 and M1516-06) and the Cameroon National Ethical Committee of Research for Human Health. Participation involved obtaining informed consent initiated at a variety of levels following a process of sequential community meetings explaining the purpose of the study and its methods, thereafter obtaining written consent from adults and guardians of children. All participants found infected with schistosomiasis or STH were offered praziquantel (40 mg/kg) and (or) mebendazole (500 mg) treatment.
Assessment of schistosomiasis and soil-transmitted helminth infection
A single stool and mid-morning urine sample was each collected from all participants. Urine was first inspected visually for macrohaematuria according to a colour reference and turbidity chart [45] before being tested with reagent strips, Siemens Multistix® 10 SG and Siemens CLINITEK® Microalbumin 9 reagent dipstick, using a CLINITEK Status® + autoanalyser (Siemens Healthcare Ltd, Camberley, Surrey, UK) which have been used previously for detailed urological assessments [46] and a urine-CCA dipstick (Rapid Medical Diagnostics®, Pretoria, South Africa) for detection of intestinal schistosomiasis. For each urine sample, up to 60 ml but at least 10 ml, was filtered by plastic syringe across a 25 μm nylon pore filter within a 2.5 cm diameter swinnex filter holder. To visualise eggs, nylon filters were stained with Lugol’s iodine then counted under the microscopy at x100 magnification, with egg tallies expressed per 10 ml urine filtered [47]. Stool samples underwent four separate stool tests undertaken in parallel; I) a faecal occult blood test was performed [48], II) a double thick Kato-Katz smear was prepared for each sample and viewed at x100 magnification [48], III) approximately 5 g of stool was inspected by the Baermann concentration method, incubated for 2 h, following centrifugation and inspection of faecal pellet [47] and IV) a charcoal stool culture was prepared with approximately 3 g of stool and later incubated at ambient temperature inside a cooler box for 72 h before inspection under the dissecting microscope for parasite larvae [47].
Participant questionnaire
A pro forma questionnaire was implemented (available upon request from JRS), used in a face-to-face interview setting to record each participant’s demographics, general signs and symptoms, anthelminthic treatment history as well as access and utilization of local WASH-related infrastructure. Urological symptoms included self-reported dysuria, macrohaematuria, frequency of urination, lower abdominal pain and lower back pain. Frequency of each symptom was recorded as never occurring, or occurring daily, weekly or monthly. An additional set of questions was directed to females ≥16 years of age to investigate female genital schistosomiasis (FGS). FGS symptomatology included questions pertaining to intermenstrual bleeding, genital itching, vaginal discharge, dyspareunia and post coital bleeding.
Local water and sanitation facilities were inspected by the field team and classified into improved and unimproved facilities, according to definitions from the WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation (JMP) (WHO & UNICEF, 2015). A water contact risk score was calculated, based on that of Rudge et al. [49] by pooling affirmative responses to questions such as swimming, fishing, bathing etc., whereby water exposure activities were categorised by frequency of occurrence (never, daily, weekly or monthly), being assigned a categorical weighting [49].
Malacological surveys
Shoreline sites to be surveyed were based upon convenience sampling through observation of human water contact sites and by having adequate accessibility by foot or by canoe for the field team. At each site, four collectors searched by hand and with metal collection sieves for 20 min, recording all aquatic snails encountered. Global positioning system (GPS) coordinates, altitude and location photographs were taken with an Oregon 650 receiver (Garmin, Olathe, Kansas, USA). Water temperature (°C), pH and conductivity (μS) were recorded with a HI-98129 Pocket EC/TDS and pH Tester (Hanna Instruments Ltd, Leighton Buzzard, Bedfordshire, UK). All collected snails of medical importance were initially identified according to morphological keys of David S. Brown [50]. Snails were counted, graded by placement against ruler into small, medium and large size categories for each species, then transferred into plastic cups containing mineral water. Snails were subsequently exposed to natural or artificial light for two hours, the water was decanted and viewed under a dissecting microscope for cercariae and identified following Frandsen and Christensen [51].
Molecular characterisation of snails and schistosomes
After inspection for cercariae, snails were then placed into absolute ethanol before transfer to the UK where genomic DNA was obtained according to standard extraction protocols [52]. Genetic variation within a partial region of the mitochondrial cytochrome oxidase sub-unit 1 (cox1) gene [53], following modified protocols described by Kane et al. [54], was obtained. Snails were also assayed for presence of schistosome DNA by real-time PCR with Taqman® probes using schistosome–specific primers described by Verweij [55]. In total, 18 schistosome miracidia hatched from infected urine were placed on Whatman® FTA® indicator cards (Sigma-Aldrich, Gillingham, Dorset, UK), then inspected for sequence variation within the ribosomal internal transcribed spacer (ITS) and mitochondrial cox1 using standard methods and bioinformatics protocols [56, 57].
Data analysis
All numerical data were double-entered using Microsoft Excel 2013 and checked, with tabulations, graphs and statistical analyses conducted using IBM Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Egg counts and intensity of infection are well known to follow non-parametric distributions. Other variables were investigated as to whether they were distributed normally; parametric and non-parametric tests were then used accordingly. Helminth prevalence was calculated with 95% binomial confidence intervals. Chi-square and Fisher’s exact tests were used to check for associations between helminth infection, site, risk factors and morbidity. Mann–Whitney U-tests were used to check for differences in intensity of infection and water contact risk score by site. Univariable analysis and multivariable logistic regression analysis was conducted for Sc. haematobium associations with independent variables. Age group (preschool-aged children (PSAC); school-aged children (SAC); adults), gender and village site were included as core variables in all regression models, and a stepwise regression approach was used to arrive at the most parsimonious adjusted model, applying a 5% level of statistical significance.
Results
In total, 338 participants were recruited to the study across both villages, 126 at Barombi Mbo and 212 at Barombi Kotto; post-hoc calculations using observed prevalence indicated that sample sizes were exceeded for both communities for all diseases. The mean age across the study population was 22.5 years (from 1.0 to 83.5 years; Table 1). Of the adult cohort, 84 (55.6%) participants were male and 67 (44.4%) were female. Three women (2.1%) were pregnant and five (5.2%) reported to be menstruating and not formally included in analysis of haematuria.
Prevalence and intensity of schistosomiasis
Prevalence of schistosomiasis is shown in Table 1 across the different demographic groups. All Sc. haematobium infections at Barombi Mbo were classified as light (arithmetic mean egg count of all infected cases 2.2 eggs per 10 ml). At Barombi Kotto however, of 85 people infected (40.1% of total population), 18 infections (21.2% of those with egg-patent infection) were classified as heavy (greater than 50 eggs per 10 ml) with arithmetic mean egg count of all infected cases being 50.5 eggs per 10 ml. This difference between sites was significant (P < 0.001). At Barombi Mbo intensity of infection was highest among adults while at Barombi Kotto it was highest within children of school age. Mean water contact risk scores were higher among infected participants (P < 0.001) and also higher among participants in Barombi Kotto compared to Barombi Mbo (P < 0.001), Table 2. Use of lake water for domestic purposes was associated with infection (χ2(1) 6.84, P = 0.009). Risk factors associated with egg-patent infection are shown in Table 3, the strongest associations being lake location and sourcing water from it.
Urinary symptomatologies were more frequently reported at Barombi Kotto, with school children reporting the highest frequencies of dysuria (χ2(2) 11.076, P = 0.004) and macrohaematuria (χ2(2) 11.076, P = 0.004, Fig. 2a). Proteinuria, abnormal urology and albuminuria were all associated with infection and showed positive correlations with egg counts (data not shown). In the subgroup of females ≥16 years (n = 67), 54 (81%) completed the FGS questionnaire, with 27 women (50%) reporting ≥1 symptom. Presence of any four FGS symptoms was correlated with infection (P = 0.023). FGS symptoms were more commonly reported in Barombi Kotto (Fig. 2b).

Bar charts of prevalence of sign and symptoms reported by participant or by diagnostic testing. a Several urological parameters differ between Barombi Mbo and Barombi Kotto. b Key symptoms of female genital schistosomiasis differ between crater lake populations
Prevalence and intensity of STH
According to faecal sampling, overall prevalence of STH in 2016 was 6.3% (n infected = 15; 95% CI 3.6–10.0, including 2 cases of T. trichiura-hookworm co-infection). From Baermann and charcoal culture methods, no larva of St. stercoralis was encountered, although hookworm larvae were recovered from two charcoal cultures, and no egg of A. lumbricoides was observed. Eggs of T. trichiura were observed in Kato-Katz smears prepared at Barombi Mbo with a general prevalence of 8.0%, Table 4. Hookworm prevalence as measured by Kato-Katz sampling varied between 2.0–4.0% between the crater lakes. In comparison to 2004 data, there have been substantial reductions in STH prevalence at both Barombi Mbo and Barombi Kotto, with a relative decrease of more than 79.0%, Table 4.
WASH-related findings
WASH-related infrastructure and associated hygiene behaviours differed between lakes. In 2008, a fully functioning gravity flow, closed piped water system with sand box filter, had been installed at Barombi Mbo by a USA-based non-government development organisation which had also provided individual households with sand-filter boxes within households, and many of these were in use, see Fig. 3. Eighty-three per cent of participants at Barombi Mbo reported use of improved drinking water whereas all Barombi Kotto participants reported using unimproved drinking water which was taken from a nearby waterfall (use of lake water χ2(1) 10.891, P = 0.001). However, use of improved sanitation facilities was similar for each village; being 35% of participants at Barombi Mbo and 39% of participants at Barombi Kotto (P = 0.622). In terms of behaviour there was no significant difference between villages for reported shoe wearing (55% of Barombi Mbo residents, and 50% of Barombi Kotto residents, always wearing shoes; P = 0.540), and mild differences for reported soap use when handwashing (28% for Barombi Mbo and 38% for Barombi Kotto always using soap; P = 0.030).

Photographs of pertinent WASH intrastructures found at Barombi Mbo. a Gravity flow reservoir located 2 km away from the village. b Typical housing of Barombi Mbo with piped water stand nearby houshold grave [inset. Sandbox water filter for household drinking water]. c Village stand pipe for water; note open field drainage of water [inset. Several open drains from piped water coalesce in the center of the village and form an open drain, as yet not colonised by snails which are found downstream: B. forskalii are found at site A5 (see Fig. 4c)]. d Lakeshore canoe landing site where many B. truncatus were found often in discarded cut bamboo and plastic containers amongst the water lilies and aquatic vegetation
Treatment history with anthelminthics
Significantly more residents of Barombi Kotto (73.2%) reported having received anthelminthic treatment previously, compared to residents of Barombi Mbo (47.9%, P = <0.001). Participants who reported a history of previous infection were associated with having current schistosome egg-positive urine (χ2(1) 13.25, P < 0.001), as were those who reported never having received treatment (χ2(1) 4.04, P = 0.045), with positive associated risk factors, Table 3. Reported treatment coverage was lowest in the PSAC group.
Malacology surveys
Thirteen collecting sites around Barombi Mbo (A2 - A14), 7 around the central island of Barombi Kotto (A15 - A21) and 9 sites around Barombi Kotto lake perimeter (A22 – A30; note A30 was an outflow stream) were surveyed, see Fig. 4. Water chemistry readings were collected at each site and for Barombi Mbo the average temperature was 30.2 °C, mean pH of 7.9 and mean conductivity was 64.3 μS, for Barombi Kotto, the average temperature was 31.2 °C, mean pH of 9.6 and mean conductivity was 202.1 μS. The waters of Barombi Mbo have significantly lower pH and conductivity than Barombi Kotto (all P < 0.0001). Fig. 4 depicts the survey locations at Barombi Mbo; a total of 166 Bulinus were found (B. truncatus (n = 89) and B. forskalii/camerunensis (n = 77)) occurring at three sites (A2, A5 and A7). Since B. forskalii and B. camerunensis are only distinguishable upon molecular analysis, those snails that were collected but were not subjected to DNA analysis were referred to as B. forskalii/camerunensis. No snail from Barombi Mbo was observed to shed schistosome cercariae.

Schematic plot of snail collecting sites at Barombi Mbo and Barombi Kotto. a Barombi Mbo is aprroximately 2.5 km in diameter with human water contact sites at either side of the lake, b southern lake shore, c northern lake shore, all sample sites (green pins); sites where snails were found are indicated by red pins. d Barombi Kotto is approximately 1.2 km in diameter with water contact sites largely spread around the whole shoreline. Location of all sampling sites (green pins); sites where snails were found are indicated by red pins. e Location of sampling site on the central inhabited island of Barombi Kotto
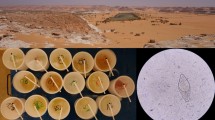
At Barombi Kotto apart from at three sites, snails were present in all sampling locations where twice as many snails per site were found along the island shoreline versus the lake perimeter. In total, 285 Bulinus forskalii/camerunensis were found and were of mixed sizes indicating all levels of snail maturity. An unexpected discoidal planorbid, tentatively identified upon shell morphology as either (?)Helisoma or (?)Indoplanorbis, was very common, with a total of 220 snails found. Following an anatomical dissection and inspection of the male genitalia together with an analysis of the coxI (see Fig. 5), this species was identified as Indoplanorbis exustus and is a first report of this Asian invasive species in Cameroon. Two B. camerunensis snails were observed to be shedding schistosome cercariae (site A20), and strigeid and gymnocephalous cercariae were encountered at sites A2 and A26.

Indoplanorbis exustus from Barombi Kotto. a Shell photographs (scale bar 0.5 cm). b Variant nucleotides within the cox1 upon comparison with reference DNA sequence. c Typical male genitalia from dissected snails having a characteristic short preputium (without the accessory gland characteristic of Helisoma spp.) and long penis sheath which clearly resembles the anatomy of Bulinus
Molecular characterisation of snails and schistosomes
Real-time PCR assays detected Schistosoma DNA in three B. truncatus, all from site A2, at Barombi Mbo. Partial coxI sequences were obtained for three B. truncatus and three B. forskalii/camerunensis, and were used in a BLAST search of GenBank. Exact matches were found with B. truncatus (GenBank: KJ157409.1) [58] and B. camerunensis (GenBank: AM286309.2) [54]. At Barombi Kotto, real-time PCR analyses detected the presence of Schistosoma DNA in seven B. forksalii/camerunensis and in two Indoplanorbis exustus (all from site A20). Partial coxI sequences were obtained from six B. forskalii/camerunensis and three Indoplanorbis exustus finding exact matches upon BLAST searches with B. camerunensis (GenBank: AM286309.2) [54] and very high similarity (98.8%) with I. exustus (GenBank: AY577511.1) [59].
The partial cox1 and ribosomal ITS sequences were successfully generated from 11 schistosome miracidia from Whatman® FTA® cards. A BLAST search of GenBank revealed exact matches with cox1 haplotype S. haematobium H1 found previously from material collected from Barombi Mbo (GenBank: JQ397366) and Barombi Kotto (GenBank:JQ397367) and ITS S. haematobium sequence (GenBank:JQ595394).
Discussion
The fauna of these crater lakes of Cameroon [27, 28, 60–63] have been the subject of much study as well as their surrounding geomorphology [64] and sedimentology [65], which provides strong evidence of human settlement some 2 800 years ago [66]. Today, each lake has several unique features, either natural or of manmade-origin. Barombi Mbo is much larger (2 500 m v. 1 200 m in diameter), substantially deeper (111 m v. 6 m), does not have a central inhabited island and is more oligotrophic (i.e. poor in nutrients) than Barombi Kotto. The majority of the shoreline of Barombi Mbo is very steeply shelved and largely not accessible by foot. In terms of limnology, while surface water temperatures are very similar, the pH and water conductivity are clearly different. Barombi Kotto is more alkaline with higher conductivity with more turbid, typically green water supporting copious phytoplankton [62].
Several of these differences were noted over 40 years ago reporting pH (6.3-7.0 v. >9.0) and conductivity (39.0 μS v. 150 μS) [35, 61, 62]. It is interesting that current water conductivity readings seem to have increased in both lakes. This could be due to anthropogenic influences such as pollution or by progressive eutrophication from surrounding cocoa plantations, the main cash crop. In comparison to other water bodies, the freshwater snail fauna here is meagre, with prosobranch species absent [50] and little planorbid biodiversity [67], for only 3 species of Bulinus, and an invasive Asian species Indoplanorbis exustus [68], were present. This latter species is an important intermediate host of Asiatic schistosomes and several food borne trematodes [69]. It has dispersed across continents, likely spread by man through the aquatic plant trade or by pisciculture through restocking [70]. Experimental infections of I. exustus with African schistosomes have not been able to demonstrate compatibility as yet [68], so this species may be playing a beneficial role as a biological control agent by drawing away schistosome miracidia that might otherwise develop in local Bulinus. This is supported by the detection of Schistosoma DNA in snails at site A20 but further study of the experimental compatibility of this species with local schistosomes would be advisable, as well as, increasing vigilance for other trematode diseases it may be able to transmit.
In terms of schistosomiasis and STH, the importance of the former was first described in these crater lakes in 1953 [36], with serious attempts to control its impact some twenty years later. These involved a combination of focal mollusciciding with frescon and mass treatment of patients with either ambilhar or niridazole [32–35]. While there was much promise in these efforts, they were not sustained, for each control tool became obsolete, and similar integrated approaches were largely abandoned [7, 71]. There were, however, attempts to use alternative molluscicides (i.e. bayluscide) in other parts of Cameroon [6, 31, 72], but only after the anthelminthic praziquantel became available and more affordable [73] could large-scale interventions against schistosomiasis become scalable [74]. This was further enhanced by the donation by Merck-KGaA (http://unitingtocombatntds.org/endorsement/merck-kgaa), so delivery of praziquantel could be integrated with either mebendazole or albendazole, expanding the remit of preventive chemotherapy campaigns to tackle several diseases simultaneously and, more importantly, at increasing scales of operation given the endemic zone of schistosomiasis and STH in Cameroon [9–11, 13, 19, 38, 75–77].
Nonetheless schistosomiasis and STH within these crater lakes have continued to cause morbidity for decades [15, 44], although the reported declines in prevalence of STH from 2004 are particularly impressive, and the absence of Strongyloides spp. has been confirmed. Even today, however, the disease burden of urogenital schistosomiasis is not fully appreciated, particularly in reference to FGS [78] or in its burden in preschool-aged children [79]. This was each clearly demonstrated in Barombi Kotto by raised signs and symptoms of FGS, for example dyspareunia, in women and that a quarter of PSAC had egg-patent infections. It is therefore appropriate to consider better targeting of preventive chemotherapy to these vulnerable populations if ensuing morbidity is to be better averted. This should become a subject of further investigation as interventions are targeted towards addressing these obvious gaps.
In the context of reported anthelminthic treatment coverage of 73.2% and 47.9%, ascertained in SAC and adults, at Barombi Kotto and Barombi Mbo respectively, there is still some room for improvement. Options for more intensified control interventions could include increasing frequency of treatment by offering selective treatment to those who request it throughout the year, alongside current MDA interventions which could operate at treatment cycles shorter than the current annual provision. In terms of gaining and sustaining control at Barombi Kotto, biannual MDA treatment could accelerate better towards expected declines in parasitaemia by mitigating reinfection more strongly. Previously the reinfection dynamics of schistosomiasis have been shown to be variable at mixed infection foci [19], but given that autochthonous transmission of intestinal schistosomiasis is not possible here as Biomphalaria is absent, future studies could shed more light on re-infection patterns. This should specifically address each of the currently infected demographic groups to help tailor future retreatment cycles.
An important additional point to consider when planning intensified control interventions is deciding when and how MDA campaigns should transition to test and treat strategies and in which demographic groups. The need to do so is exemplified by Fig. 6, where two SAC and one PSAC (see Fig. 6, numbered 1–3 inside the green box) from Barombi Kotto reported to wash regularly in the lake and complained of dysuria; furthermore four adults at Barombi Kotto (two males and two females) were identified as having egg counts far above the mean (see Fig. 6, numbered 4–7). Three reported to have had urogenital previously and had received treatment previously although all swam and washed in the lake, and both males fished. These findings support typical profiles of infected individuals, for example, high risk water contact, evidence of urological morbidity and sporadic treatment history. Some future targeting is needed to better identify these individuals such that all are treated more regularly to ensure that their inputs to environmental contamination are mitigated as best possible.

Scattergram of intensity of egg-patent infection with participant age reveals that there are individuals within each demographic group that have much higher than average egg counts (individuals 1–3 being school-aged children and individuals 4–7 being adults). It is likely that these individuals are most responsible for transmission of the disease, therefore future targetting of treatment to these individuals specifically would be worthwhile
As preventive chemotherapy does not guard against reinfection, broadening the scope of intensified interventions against schistosomiasis and STH to go beyond that of current anthelminthic treatment regimens alone, is crucial; hence WASH-related interventions that reduce environmental transmission and exposure are important [14, 17]. Most significantly, since 2008 the inhabitants of Barombi Mbo have benefited from the provision of an extensive improved water supply, bringing piped water close to all households, Fig. 3. It would seem likely that in addition to preventive chemotherapy this WASH intervention has clearly helped reduce those diseases where faecal-oral transmission occurs, given that household sanitation was relatively similar between locations. Whilst the transmission of schistosomiasis shares several features with STH, urogenital schistosomiasis sets itself apart by being transmitted within urine and not within stool.
It is open to conjecture what impact an improved water supply might have at Barombi Kotto in terms of transmission of urogenital schistosomiasis, if similarly installed and used since risk factors at each lake are clearly different, Table 2. While there are direct and indirect impacts of improving WASH for those who would no longer depend on drawing domestic water from the lake but, however, for those that fish, cross by canoe or play in the lake their cumulative water contact levels, and risk of infection, might not significantly reduce. All of the latter are significant local risk factors, see Table 3. Future recourse to snail control with focal molluscicides could be beneficial, and particularly insightful when set against previous attempts locally [32–34]. Historically, however, the prevalence of STH was much less than that at Barombi Mbo and in explanation, the volcanic soil type at Barombi Kotto might not be favourable for STH. Nevertheless, a safer water supply for the inhabitants on the Barombi Kotto island would be beneficial as a significant complementary factor for intensified treatment interventions and for several other reasons outside that of current STH and schistosomiasis control perspectives.
Conclusions
Our findings have implications in better tailoring and evaluating future interventions against schistosomiasis and STH, as several important lake-specific heterogeneities have been revealed. STH is currently at very low levels while urogenital schistosomiasis is of greatest concern at Barombi Kotto. The study of the epidemiological dynamics of each disease in these crater lakes provides a context for future assessment of intensified control, for example, it is most insightful for urogenital schistosomiasis in terms of gaining and sustaining control at Barombi Kotto or in moving towards local interruption of transmission at Barombi Mbo.
Abbreviations
- CCA:
-
Circulating cathodic antigen
- DNA:
-
Deoxyribonucleic acid
- FGS:
-
Female genital schistosomiasis
- GPS:
-
Global positioning system
- ITS:
-
Internal transcribed spacer
- JMP:
-
WHO/UNICEF joint monitoring programme for water supply and sanitation
- MDA:
-
Mass drug adminsitration
- NTDs:
-
Neglected tropical diseases
- PCR:
-
Polymerase chain reaction
- PSAC:
-
Pre-school-aged children
- SAC:
-
School-aged children
- STH:
-
Soil transmitted helminthiasis
- WASH:
-
Water, sanitation and hygiene
References
WHO-AFRO. Briefs of country master plans for neglected tropical disease programmes in the WHO African Region. Brassavile: WHO-AFRO; 2013.
Noatina BN, Kagmeni G, Souleymanou Y, Moungui HC, Hien AT, Akame J, Zhang YB, Bella ALF: Prevalence of trachoma in the North Region of Cameroon: results of a survey in 15 health districts. PLoS NTDs 2014, 8(6).
Nana-Djeunga HC, Tchatchueng-Mbougua JB, Bopda J, Mbickmen-Tchana S, Elong-Kana N, Nnomzo'o E, Akame J, Tarini A, Zhang Y, Njiokou F, et al. Mapping of Bancroftian filariasis in Cameroon: prospects for elimination. PLoS NTDs. 2015;9(9).
Wanji S, Kengne-Ouafo JA, Esum ME, Chounna PWN, Adzemye BF, Eyong JEE, Jato I, Datchoua-Poutcheu FR, Abong RA, Enyong P et al.: Relationship between oral declaration on adherence to ivermectin treatment and parasitological indicators of onchocerciasis in an area of persistent transmission despite a decade of mass drug administration in Cameroon. Parasites & Vectors 2015, 8.
Brooker S, Hay SI, Tchuente LAT, Ratard R. Using NOAA-AVHRR data to model human helminth distributions in planning disease control in Cameroon, West Africa. Photogramm Eng Remote Sens. 2002;68(2):175–9.
Greer GJ, Mimpfoundi R, Malek EA, Joky A, Ngonseu E, Ratard RC. Human schistosomiasis in Cameroon.2. Distribution of the snail hosts. Am J Trop Med Hyg. 1990;42(6):573–80.
Ratard R, Ekani MM, Greer GJ, Kouemeni L, Mimpfoundi R, Ngonseu E. Schistosomiasis in Cameroon. Parasitol Today. 1988;4(7):199.
Ratard RC, Kouemeni LE, Bessala MKE, Ndamkou CN. Distribution of hookworm infection in Cameroon. Ann Trop Med Parasitol. 1992;86(4):413–8.
Ratard RC, Kouemeni LE, Bessala MME, Ndamkou CN. Estimation of the number of cases of schistosomiasis in a country – the example of Cameroon. Trans R Soc Trop Med Hyg. 1992;86(3):274–6.
Ratard RC, Kouemeni LE, Bessala MME, Ndamkou CN, Greer GJ, Spilsbury J, Cline BL. Human schistosomiasis in Cameroon.1. Distribution of schistosomiasis. Am J Trop Med Hyg. 1990;42(6):561–72.
Ratard RC, Kouemeni LE, Bessala MME, Ndamkou CN, Sama MT, Cline BL. Ascariasis and trichuriasis in Cameroon. Trans R Soc Trop Med Hyg. 1991;85(1):84–8.
Vercruysse J, Behnke JM, Albonico M, Ame SM, Angebault C, Bethony JM, Engels D, Guillard B, Hoa NTV, Kang G, et al. Assessment of the anthelmintic efficacy of albendazole in school children in seven countries where soil-transmitted helminths are endemic. PLoS NTDs. 2011;5(3).
Tchuente LAT, N’Goran EK. Schistosomiasis and soil-transmitted helminthiasis control in Cameroon and Cote d’Ivoire: implementing control on a limited budget. Parasitology. 2009;136(13):1739–45.
Ndamkou NC, Ratard RC. Are sanitation, water-supply and a health-center sufficient to control schistosomiasis – the case of Douloumi, North Cameroon. Trop Dr. 1990;20(4):176–7.
Sama MT, Ratard RC. Water contact and schistosomiasis infection in Kumba, South-Western Cameroon. Ann Trop Med Parasitol. 1994;88(6):629–34.
Tchuente LAT, Southgate VR, Webster BL, De Bont J, Vercruysse J. Impact of installation of a water pump on schistosomiasis transmission in a focus in Cameroon. Trans R Soc Trop Med Hyg. 2001;95(3):255–6.
Cline BL, Hewlett BS. Community-based approach to schistosomiasis control. Acta Trop. 1996;61(2):107–19.
Cunin P, Tchuente LAT, Poste B, Djibrilla K, Martin PMV. Interactions between Schistosoma haematobium and Schistosoma mansoni in humans in north Cameroon. Tropical Med Int Health. 2003;8(12):1110–7.
Tchuente LAT, Momo SC, Stothard JR, Rollinson D. Efficacy of praziquantel and reinfection patterns in single and mixed infection foci for intestinal and urogenital schistosomiasis in Cameroon. Acta Trop. 2013;128(2):275–83.
Webster BL, Tchuente LAT, Jourdane J, Southgate VR. The interaction of Schistosoma haematobium and S-guineensis in Cameroon. J Helminthol. 2005;79(3):193–7.
Tchuente LAT, Southgate VR, Jourdane J, Webster BL, Vercruysse J. Schistosoma intercalatum: an endangered species in Cameroon? Trends Parasitol. 2003;19(9):389–93.
Southgate VR, Vanwijk HB, Wright CA. Schistosomiasis at Loum, Cameroun, Schistosoma haematobium, S. intercalatum and their natural hybrid. Zeitschrift Fur Parasitenkunde-Parasitology Res. 1976;49(2):145–59.
Tchuente LAT, Morand S, ImbertEstablet D, Delay B, Jourdane J. Competitive exclusion in human schistosomes: The restricted distribution of Schistosoma intercalatum. Parasitology. 1996;113:129–36.
Wright CA, Southgate VR, Vanwijk HB, Moore PJ. Hybrids between Schistosoma haematobium between Schistosoma intercalatum in Cameroon. Trans R Soc Trop Med Hyg. 1974;68(5):413–4.
Webster BL, Southgate VR, Tchuente LAT. Isoenzyme analysis of Schistosoma haematobium, S. intercalatum and their hybrids and occurrences of natural hybridization in Cameroon. J Helminthol. 2003;77(3):269–74.
Webster BL, Tchuente LAT, Southgate VR. A single-strand conformation polymorphism (SSCP) approach for investigating genetic interactions of Schistosoma haematobium and Schistosoma guineensis in Loum, Cameroon. Parasitol Res. 2007;100(4):739–45.
Gow JL, Noble LR, Rollinson D, Mimpfoundi R, Jones CS. Breeding system and demography shape population genetic structure across ecological and climatic zones in the African freshwater snail, Bulinus forskalii (Gastropoda, Pulmonata), intermediate host for schistosomes. Mol Ecol. 2004;13(11):3561–73.
Jones CS, Rollinson D, Mimpfoundi R, Ouma J, Kariuki HC, Noble LR. Molecular evolution of freshwater snail intermediate hosts within the Bulinus forskalii group. Parasitology. 2001;123:S277–92.
Mimpfoundi R, Greer GJ. Allozyme comparisons among species of the Bulinus-forskalii group (Gastropoda, Planorbidae) in Cameroon. J Molluscan Stud. 1989;55:405–10.
Mimpfoundi R, Ndassa A. Morphological studies on Bulinus sp (Gastropoda : Planorbidae) from Nchout Monoun, Cameroon. Afr Zool. 2006;41(2):210–4.
Greer GJ, Tchounwou PB, Takougang I, Monkiedje A. Field tests of a village-based mollusciciding programme for the control of snail hosts of human schistosomes in Cameroon. Tropical Med Int Health. 1996;1(3):320–7.
Duke BOL, Moore PJ. Use of a molluscicide, in conjunction with chemotherapy, to control Schistosoma haematobium at Barombi lake foci in Cameroon.1. Attack on snail hosts, using N-tritylmorpholine, and effect on transmission from snail to man. Tropenmed Und Parasitol. 1976;27(3):297–313.
Duke BOL, Moore PJ. Use of a molluscicide in conjunction with chemotherapy to control Schistosoma haematobium atBarombi lake foci in Cameroon.2. Urinary examination methods, use of niridazole to attack parasite in man, and effect on transmission from man to snail. Tropenmed Und Parasitol. 1976;27(4):489–504.
Duke BOL, Moore PJ. Use of a molluscicide in conjunction with chemotherapy to control Schistosoma haematobium at Barombi lake foci in Cameroon.3. Conclusions and costs. Tropenmed Und Parasitol. 1976;27(4):505–8.
Duke BOL, Moore PJ. Control of Schistosoma haematobium in West-Cameroon. Trans R Soc Trop Med Hyg. 1971;65(6):841.
Zhara A. Some notes on the incidence of schistosomiasis in the southern Cameroons. West Afr Med J. 1953;2(1):26–9.
Tchuente LAT, Ngassam RIK, Sumo L, Ngassam P, Noumedem CD, Nzu DDL, Dankoni E, Kenfack CM, Gipwe NF, Akame J, et al. Mapping of schistosomiasis and soil-transmitted helminthiasis in the regions of Centre, East and West Cameroon. PLoS NTDs. 2012;6(3).
Tchuente LAT, Noumedem CD, Ngassam P, Kenfack CM, Gipwe NF, Dankoni E, Tarini A, Zhang YB. Mapping of schistosomiasis and soil-transmitted helminthiasis in the regions of Littoral, North-West, South and South-West Cameroon and recommendations for treatment. BMC Infect Dis. 2013;13.
Nkenfou CN, Nana CT, Payne VK. Intestinal parasitic infections in HIV infected and non-infected patients in a low HIV prevalence region, West-Cameroon. PLoS One. 2013;8(2).
Moyou-Somo R, Kefie-Arrey C, Dreyfuss G, Dumas M. An epidemiological study of pleuropulmonary paragonimiasis among pupils in the peri-urban zone of Kumba town, Meme Division, Cameroon. BMC Public Health. 2003;3.
Pourrut X, Diffo JLD, Somo RM, Bilong CFB, Delaportee E, LeBreton M, Gonzalez JP. Prevalence of gastrointestinal parasites in primate bushmeat and pets in Cameroon. Vet Parasitol. 2011;175(1–2):187–91.
Stothard JR, Kabatereine NB, Archer J, Al-Shehri H, Tchuem-Tchuenté LA, Gyapong M, Bustinduy AL. A centenary of Robert T. Leiper’s lasting legacy on schistosomiasis and a COUNTDOWN on control of neglected tropical diseases. Parasitology. 2016;1:1–11.
Anon: http://www.lstmed.ac.uk/news-events/news/countdown-consortium-launches-in-cameroon. 2016. Accessed 20 Feb 2017.
Somo RM, Zukam DT, Kouamouo J, Enyong P, Ripert C. An epidemiological and radiological study of the vesical schistosomiasis foci of the Barombi lakes, Meme Division, Cameroon. Bull Soc Pathol Exot. 1987;80(5):813–22.
Rollinson D, Klinger EV, Mgeni AE, Khamis IS, Stothard JR. Urinary schistosomiasis on Zanzibar: application of two novel assays for the detection of excreted albumin and haemoglobin in urine. J Helminthol. 2005;79(3):199–206.
Stothard JR, Sousa-Figueiredo JC, Khamis IS, Garba A, Rollinson D. Urinary schistosomiasis-associated morbidity in schoolchildren detected with urine albumin-to-creatinine ratio (UACR) reagent strips. J Paediatr Urol. 2009;5:287–91.
Cheesbrough M. Medical laboratory manual for tropical countries. 1981.
Bustinduy AL, Sousa-Figueiredo JC, Adriko M, Betson M, Fenwick A, Kabatereine N, Stothard JR. Fecal occult blood and fecal calprotectin as point-of-care markers of intestinal morbidity in Ugandan children with Schistosoma mansoni infection. PLoS NTDs. 2013;7(11).
Rudge JW, Stothard JR, Basanez MG, Mgeni AF, Khamis IS, Khamis AN, Rollinson D. Micro-epidemiology of urinary schistosomiasis in Zanzibar: Local risk factors associated with distribution of infections among schoolchildren and relevance for control. Acta Trop. 2008;105(1):45–54.
Brown DS. Freshwater snails of Africa and their medical importance, 2nd edn. London: Taylor & Francis Ltd; 1994.
Frandsen F, Christensen NO. An introductory guide to the identification of cercariae from African fresh-water snails with special reference to cercariae of trematode species of medical and veterinary importance. Acta Trop. 1984;41(2):181–202.
Stothard JR, Rollinson D. An evaluation of random amplified polymorphic DNA (RAPD) for the identification and phylogeny of freshwater snails of the genus Bulinus (Gastropoda: Planorbidae). J Molluscan Stud. 1996;62:165–76.
Stothard JR, Rollinson D. Partial DNA sequences from the mitochondrial cytochrome oxidase subunit I (COI) gene can differentiate the intermediate snail hosts Bulinus globosus and B-nasutus (Gastropoda: Planorbidae). J Nat Hist. 1997;31(5):727–37.
Kane RA, Stothard JR, Emery AM, Rollinson D: Molecular characterization of freshwater snails in the genus Bulinus: a role for barcodes? Parasites & Vectors 2008, 1.
Verweij JJ. Application of PCR-based methods for diagnosis of intestinal parasitic infections in the clinical laboratory. Parasitology. 2014;141(14):1863–72.
Boissier J, Grech-Angelini S, Webster BL, Allienne JF, Huyse T, Mas-Coma S, Toulza E, Barre-Cardi H, Rollinson D, Kincaid-Smith J, et al. Outbreak of urogenital schistosomiasis in Corsica (France): an epidemiological case study. Lancet Infect Dis. 2016;16(8):971–9.
Huyse T, Webster BL, Geldof S, Stothard JR, Diaw OT, Polman K, Rollinson D: Bidirectional introgressive hybridization between a cattle and human schistosome species. Plos Pathogens 2009, 5(9).
Zein-Eddine R, Djuikwo-Teukeng FF, Al-Jawhari M, Senghor B, Huyse T, Dreyfuss G: Phylogeny of seven Bulinus species originating from endemic areas in three African countries, in relation to the human blood fluke Schistosoma haematobium. Bmc Evolutionary Biology 2014, 14.
Jorgensen A, Kristensen TK, Stothard JR. An investigation of the “Ancyloplanorbidae” (Gastropoda, Pulmonata, Hygrophila): preliminary evidence from DNA sequence data. Mol Phylogenet Evol. 2004;32(3):778–87.
Martin CH, Cutler JS, Friel JP, Touokong CD, Coop G, Wainwright PC. Complex histories of repeated gene flow in Cameroon crater lake cichlids cast doubt on one of the clearest examples of sympatric speciation. Evolution. 2015;69(6):1406–22.
Corbet SA, Green J, Griffith J, Betney E. Ecological studies on crater lakes in West Cameroon lakes Kotto and Mboandong. J Zool. 1973;170:309–24.
Green J. Ecological studies on crater lakes in West Cameroon zooplankton of Barombi Mbo, Mboandong, Lake Kotto and Lake Soden. J Zool. 1972;166:283.
Trewavas E, Green J, Corbet SA. Ecological studies on crater lakes in West Cameroon fishes of Barombi Mbo. J Zool. 1972;167(1):41.
Cornen G, Bandet Y, Giresse P, Maley J. The nature and chronostratigraphy of quaternary pyroclastic accumulations from Lake Barombi Mbo (West-Cameroon). J Volcanol Geotherm Res. 1992;51(4):357–74.
Giresse P, Maley J, Brenac P. Late quaternary paleoenvironments in the lake Barombi Mbo (West Cameroon) deduced from pollen and carbon isotopes of organic-matter. Palaeogeogr Palaeoclimatol Palaeoecol. 1994;107(1–2):65–78.
Lebamba J, Vincens A, Maley J. Pollen, vegetation change and climate at Lake Barombi Mbo (Cameroon) during the last ca. 33 000 cal yr BP: a numerical approach. Clim Past. 2012;8(1):59–78.
Kristensen TK, Brown DS. Control of intermediate host snails for parasitic diseases - A threat to biodiversity in African freshwaters? Malacologia. 1999;41(2):379–91.
Kristensen TK, Ogunnowo O. Indoplanorbis-exustus (Deshayes, 1834), a fresh-water snail new for Africa, found in Nigeria (Pulmonata, Planorbidae). J Molluscan Stud. 1987;53:245–6.
Liu LA, Mondal MMH, Idris MA, Lokman HS, Rajapakse P, Satrija F, Diaz JL, Upatham ES, Attwood SW: The phylogeography of Indoplanorbis exustus (Gastropoda: Planorbidae) in Asia. Parasites & Vectors 2010, 3.
Pointier JP, David P, Jarne P. Biological invasions: the case of planorbid snails. J Helminthol. 2005;79(3):249–56.
King CH, Sutherland LJ, Bertsch D. Systematic review and meta-analysis of the impact of chemical-based mollusciciding for control of Schistosoma mansoni and S. haematobium transmission. PLoS NTDs. 2015;9(12).
Takougang I, Meli J, Pone JW, Angwafo F. Community acceptability of the use of low-dose niclosamide (Bayluscide (R)), as a molluscicide in the control of human schistosomiasis in Sahelian Cameroon. Ann Trop Med Parasitol. 2007;101(6):479–86.
Southgate VR, Rollinson D, Tchuente LAT, Hagan P. Towards control of schistosomiasis in sub-Saharan Africa. J Helminthol. 2005;79(3):181–5.
Fenwick A, Webster JP, Bosque-Oliva E, Blair L, Fleming FM, Zhang Y, Garba A, Stothard JR, Gabrielli AF, Clements ACA, et al. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002–2008. Parasitology. 2009;136(13):1719–30.
Brooker S, Donnelly CA, Guyatt HL. Estimating the number of helminthic infections in the Republic of Cameroon from data on infection prevalence in schoolchildren. Bull World Health Organ. 2000;78(12):1456–65.
Massenet D, Inrombe J, Portal JL. Empirical check of the quality of the plans of LQAS sampling in the surveillance of the endemic schistosomiasis in North-Cameroon. Revue D Epidemiol Et De Sante Publique. 2011;59(3):197–8.
Massenet D, Toukour A, Ngassam RIK, Djao R, Portal JL, Tchuente LAT. Changes in the distribution of human schistosomiasis in Far North province, Cameroon, since 1986. Ann Trop Med Parasitol. 2011;105(4):325–8.
Christinet V, Lazdins-Helds JK, Stothard JR, Reinhard-Rupp J. Female genital schistosomiasis (FGS): from case reports to a call for concerted action against this neglected gynaecological disease. Int J Parasitol. 2016;46(7):395–404.
Stothard JR, Sousa-Figueiredo JC, Betson M, Bustinduy A, Reinhard-Rupp J. Schistosomiasis in African infants and preschool children: let them now be treated! Trends Parasitol. 2013;29(4):197–205.
Acknowledgements
JRS, LATT, SJC and LC participate in the four-country research programme consortium COUNTDOWN. We are grateful to the help and support of the communities at Barombi Mbo and Barombi Kotto.
Funding
This study is funded as part of the COUNTDOWN research programme consortium, by the Research and Evidence Division of the Department for International Development, UK. The funders had no role in study design, decision to publish, or preparation of the manuscript.
Availability of data and materials
The data from these COUNTDOWN studies will be available via the Global Atlas for Helminth Infections.
Authors’ contributions
JRS, JLC and LATT designed the study. LATT, JRS, FO, DS, TD, SJC, JLC, DEO and GDC conducted field work. DS, FO and TD analysed data with statistical advice from SJC, JLC and JRS. LC, TD, JRS and BW undertook molecular analyses of specimens. SJC drafted the manuscript with help from JRS and LATT. All the authors contributed to iterations and approved the final version.
Competing interests
None declared.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Study protocols were approved by the Liverpool School of Tropical Medicine Research Ethics Committee and the Cameroon National Ethical Committee of Research for Human Health.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Multilingual abstracts in the five official working languages of the United Nations. (PDF 906 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Campbell, S.J., Stothard, J.R., O’Halloran, F. et al. Urogenital schistosomiasis and soil-transmitted helminthiasis (STH) in Cameroon: An epidemiological update at Barombi Mbo and Barombi Kotto crater lakes assessing prospects for intensified control interventions. Infect Dis Poverty 6, 49 (2017). https://doi.org/10.1186/s40249-017-0264-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40249-017-0264-8