
Abstract
Background
Mindfulness skills training is a core component of Dialectical Behavior Therapy and aims to improve emotion dysregulation (ED) in people with Borderline Personality Disorder (BPD). However, the underlying mechanisms of change are not fully understood.
Methods
A total of 75 BPD outpatients participated in a 10-week mindfulness skills training. Multilevel models with a time-lagged approach were conducted to examine the temporal dynamics between the proposed mechanisms and ED. Decentering, nonjudgment, body awareness and attention awareness as putative mechanisms and ED as outcome were assessed on a session-by-session basis.
Results
Greater nonjudgment and body awareness showed within-person effects; participants who reported higher nonjudgement of inner experience and body awareness than their own personal average at a given week showed improvement in ED at the following week. Notably, decentering moderated these associations, such that increased nonjudgment and body awareness predicted improvements in ED more strongly in those participants with high decentering ability. Lastly, a bidirectional relationship between the mechanisms and ED was found; when participants were more emotionally dysregulated than their usual state, they showed less gain in the mechanisms at the following week.
Conclusions
Knowing how mindfulness training works is relevant to optimize treatments. Clinicians may use strategies to increase these mechanisms when the goal is to improve emotion regulation difficulties in BPD.
Similar content being viewed by others


Introduction
Borderline personality disorder (BPD) is a severe mental illness with an estimated community prevalence of 2.7%. It is characterized by affective dysregulation, unstable identity and interpersonal relationships, and serious behaviors such as non-suicidal self-injury [1, 2]. The complexity and severity of BPD is characterized by high comorbidity with other psychiatric disorders, drug and/or alcohol abuse, and a high risk of suicide [3], which lead to an extensive use of healthcare resources, high costs of treatment, polymedication, as well as impaired psychosocial and occupational functioning [4,5,6].
One of the main features underlying cognitive, affective, and behavioral instability in BPD is a pervasive pattern of emotion dysregulation (ED) [7, 8]. ED involves the inability to regulate or change an emotional response or expression in a desired manner and involves a lack of (or maladaptive use of) emotion regulation strategies [9], which in turn facilitates the emergence of impulsive and risky behaviors (e.g., self-harm, substance use). These risk behaviors can be understood as a consequence of emotion regulation difficulties or as a strategy to regulate a distressing emotional state [10]. Therefore, prevention and treatment efforts are focused on addressing ED as a means of reducing distress, suffering, psychosocial impairment, and potentially life-threatening risk behaviors in individuals with a diagnosis of BPD [11].
Psychotherapy is the main recommended treatment for BPD [10, 12]. One of the empirically based therapies for the treatment of BPD is dialectical behavior therapy (DBT) [13]. DBT is a multifaceted intervention involving individual and group therapy. The group therapy addresses the skills training and comprises four different modules: mindfulness, emotion regulation, distress tolerance, and interpersonal effectiveness. Mindfulness is one of the main components of DBT, and usually mindfulness skills serve as a foundational basis for all other DBT skills [14]. Interestingly, mindfulness skills training as a stand-alone intervention improves ED in BPD [15, 16], but the underlying mechanisms of change are not yet fully understood.
An understanding of the mechanisms (i.e., mediators) through which psychological interventions produce changes in desired outcomes (understanding how and why it works) is essential to optimize treatments [17]. In addition, identifying moderators (i.e., the effects on direction or magnitude of the relation between the intervention and outcome) may guide therapeutic strategies that effectively impact the mechanisms or processes of an intervention in order to obtain therapeutic improvements [18]. Thus, clinical research based on mechanisms of change (and moderators) may inform which processes (e.g., cognitive, behavioral) of an intervention contribute to the expected outcomes and in what ways. One way to study the mechanisms is to demonstrate that changes in the putative mechanism are related to changes in the expected outcome through a temporal precedence with repeated session-by-session measures [17, 19] and also disaggregating within- and between-person effects of the mechanisms [20]. This method allows for a more precise examination of the process of change within an individual.
Research has focused on uncovering the mechanisms of change by which DBT skills training improves ED in BPD [21]. Studies suggest that a greater use of behavioral skills (learned during DBT skills training) mediates changes in emotion dysregulation [9, 22]. More specifically, studies exploring the within-person effects found that greater skills use predicted improvements in ED [23, 24] and fewer risk behaviors associated with high ED [25] after undergoing DBT skills training. However, there is a scarcity of studies focused on studying the mechanisms of change of mindfulness skills training as a stand-alone intervention. For example, a recent study reported that the amount of mindfulness practice at a given week (a required dose of at least 3 days and 30 min per week) predicted improvements in ED at the following week in BPD outpatients [26]. Importantly, previous studies have proposed four mechanisms by which mindfulness practice may work [27, 28], which are reviewed below.
Decentering consists of adopting a change in perspective of one's own experience through the disidentification of the mental contents that are usually experienced as defining the self [29, 30]. This metacognitive capacity involves a process of meta-awareness by observing thoughts and emotions in a non-attached manner, which results in a reduced reactivity to thought content [31]. Interestingly, decentering has been proposed as a mediating mechanism in both DBT mindfulness skills training to decrease borderline symptoms [16] and emotion regulation therapy to decrease anxious-depressive symptoms [32]. Furthermore, decentering has also been postulated as a moderator that attenuates the association between other mechanisms (e.g., rumination) and psychopathology [33]. Given the metacognitive quality of decentering [31], this capacity seems useful as a therapeutic strategy to decrease fusion with negative contents of the self.
The emotion regulation process related to a nonjudgmental stance towards internal experience (i.e., when individuals stop criticizing themselves) is associated with a lower level of psychopathology [34]. However, individuals with BPD are characterized by a high tendency to judge their internal experience [14, 35]. Therefore, strategies that help increase the capacity for nonjudgment are particularly relevant to foster emotional acceptance in BPD [14]. Interestingly, this capacity (i.e., nonjudgment) is an active component of mindfulness DBT skills training. Furthermore, nonjudgmental ability has been shown to act as a mediating mechanism between DBT skills training and clinical outcomes in BPD [36, 37]. For instance, increased levels of nonjudgment over time predict fewer borderline symptoms in women with BPD features [38].
Body awareness involves paying attention to body information by identifying internal body sensations (e.g., tension) and the associated emotional state (feeling relaxed or stressed) as opposed to avoiding the bodily experience [39]. Bodily sensations are a common object of attention during mindfulness meditations [40] and would be cultivated through the ability to observe the inner experience [41]. Body awareness levels are significantly decreased in individuals with BPD compared to healthy controls, and this deficit is associated with ED [42]. Therefore, increasing body awareness is a relevant aspect in the treatment of psychological disorders, including BPD [14, 27].
Attention awareness is another putative mechanism underlying mindfulness practice and involves cultivating a present-moment awareness. For instance, mindfulness meditation involves focusing attention on an object (e.g., breathing), noticing distraction, and returning to the object of attention [43]. Promoting attention regulation in individuals with BPD is relevant to ameliorate ED and impulse control by teaching participants to observe what they are experiencing in the present moment, without attachment or avoidance of the content of the experience [14]. To our knowledge, no study has evaluated these proposed mechanisms at the same time in a mindfulness training for individuals with BPD.
Understanding how these mechanisms work can be useful for clinicians. This knowledge may provide guidance on how to teach the skills more effectively, focus on the mechanisms with the greatest impact on ED, and target precise and direct strategies on the therapeutic needs of individuals. In summary, the main question guiding this study is how participants with BPD improve their level of ED through a mindfulness skills training. Therefore, this study explored the potential mechanisms of change within mindfulness training, focusing on decentering, nonjudgment, body awareness and attention awareness. Firstly, we evaluated whether these mechanisms and ED showed improvement over the course of mindfulness skills training. Secondly, we explored the temporal dynamics between mechanisms and ED throughout mindfulness skills training. Thirdly, based on previous findings [33], we explored decentering as a metacognitive ability that could moderate (i.e., increase the strength) the relationship between the other proposed mechanisms and ED. In summary, our hypotheses were: (1) Decentering, nonjudgment, body awareness and attention awareness would increase and ED would decrease during mindfulness skills training; (2) greater within- and between-person effects of mechanisms would predict improvements in ED in the following week; and this relationship would be bidirectional; and (3) the association between nonjudgment, body awareness, and attention awareness with ED would be greater among participants with higher decentering capacity.
Method
Participants
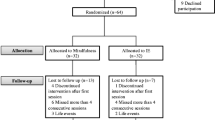
Participants were recruited from the Department of Psychiatry Unit of the Hospital de la Santa Creu i Sant Pau (Barcelona, Spain). This outpatient program is part of the Public National Mental Health Service of Spain and provides specialized care for people with BPD diagnosis. A total of 95 BPD outpatients were enrolled in a DBT skill training. Of these, 75 participants were included in the present study (13 discontinued the treatment before starting the first session; 7 had very low attendance and completed less than 3 weekly assessments). All participants were evaluated by a psychiatrist and a clinical psychologist from the psychiatry unit, both with a doctoral degree and experience in the treatment of people with BPD. The clinical diagnosis was based on two semi-structured interviews: Structured Clinical Interview for DSM IV axis II Disorders (SCID II) [44] and the Revised Diagnostic Interview for Borderlines (DIB-R) [45]. In addition, the baseline severity of borderline symptoms was assessed (Borderline Symptom List: BSL-23) [46]. The inclusion criteria were: (i) diagnostic confirmation of BPD; and (ii) age between 18–55 years. The exclusion criteria were: (i) presence of any of the following comorbid conditions: schizophrenia, drug-induced psychosis, organic brain syndrome, substance dependence, bipolar disorder, intellectual disability; and (ii) be receiving another type of psychotherapy at the time of study enrollment. Patients were allowed to continue with the drug regimen followed prior to study enrollment. However, they were not allowed to change the type or dose of drugs during the study period. Participants had not previously participated in DBT skills training.
Procedure
Participants were enrolled in a 10-week DBT mindfulness skills training. In total, 7 groups were conducted between February 2020 and October 2023 (12–15 participants/group). Each intervention group followed the same structure and weekly sessions were 2.5 h in length. All groups were led by the same team (2 clinical psychologists with training and experience in DBT, and expertise in mindfulness meditation). For each participant, written informed consent was obtained prior to inclusion in the study. The study was approved by the Clinical Research Ethics Committee of the Hospital de la Santa Creu i Sant Pau and was conducted in accordance with the criteria of the Declaration of Helsinki.
The intervention was based on the DBT skills training protocol (14). The 10-week mindfulness training program consisted of 1 week of orientation and goals, 6 weeks of mindfulness skills, and 3 weeks of acceptance skills (taken from the distress tolerance module). This mindfulness training for BPD is proposed by Linehan as an alternative to standard DBT skills training (14) and its efficacy has been shown in previous clinical trials [15, 47]. The mindfulness and acceptance skills taught were (i) Wise Mind; (ii) "What" Skills (i.e., observing, describing, participating); (iii) "How" Skills (i.e., nonjudgmentally, one-mindfully, and effectively); (iv) Radical Acceptance; (v) Mind Turning and Willingness; (vi) Half-smile and willing hands; and (vii) Mindfulness of current thoughts. Formal and informal mindfulness practice were taught during the sessions. In each session, a new skill was introduced and practiced through role-playing and discussion. Participants were then given meditation audios and worksheets related to the skills and instructed to practice at home. In the next session, the homework was reviewed and each participant commented on his or her experience with the practice, as well as any difficulties encountered. The therapist then reinforced the participants' progress and suggested effective ways to improve skill practice. The meditation audios were recorded by the lead therapist and lasted 10 min.
Measures
Several repeat measures were collected on a weekly basis during the mindfulness training. Only the first introduction/orientation session was not assessed because it did not include mindfulness skills practice. In order to assess the participants’ level of ED and specific mechanism of change, they were asked to complete the following scales before starting a new session (i.e., session 2 onwards).
Emotion dysregulation
The Brief Version of the Difficulties in Emotion Regulation Scale was used to capture how participants managed their weekly difficult emotional experiences (DERS-18) [48]. The 18-items Spanish translation of this self-report scale was administered and the total score was used in the analyses as an overall measure of emotion dysregulation. Items were rated on a scale from 1 (almost never) to 5 (almost always). This scale has high internal reliability (Cronbach's α = 0.91). In the current study, this scale obtained a good internal reliability at session 1 (Cronbach's α = 0.87).
For each mechanism of change proposed, the three most representative items from each original scale were used based on their highest factor loadings within the respective general construct. This approach aimed to simplify the weekly assessment process for participants and minimize the time required to complete the scales. The same Likert scale was used for all items, from 1 (almost never) to 5 (almost always).
Decentering
It was assessed with the Experiencing Questionnaire (EQ) [30]. The EQ is a 20-item self-report scale that assesses decentering and rumination. Decentering is the ability to observe thoughts and feelings in a detached manner [30]. In the present study, items from the Spanish validation EQ-Decentering was used [49]. These items were: (i) “I can separate myself from my thoughts and feelings” (factor loading: 0.74); (ii) “I can observe unpleasant feelings without being drawn into them” (factor loading: 0.72); (iii) “I view things from a wider perspective” (factor loading: 0.77). The Spanish EQ version has good internal reliability (Cronbach’s α = 0.89) [49] and in the present study the 3-items scale had an acceptable internal reliability at session 1 (Cronbach’s α = 0.73).
Nonjudgment
It was assessed with the Nonjudging of Inner Experience sub-scale of Five Facets Mindfulness Questionnaire (NJ-FFMQ) [40]. NJ-FFMQ refers to taking a non-evaluative stance toward thoughts and feelings and is closely associated with acceptance, a central component of mindfulness [41, 50]. In the present study, items of the Spanish validation of NJ-FFMQ subscale was used [50]. These items were: (i) “I make judgments about whether my thoughts are good or bad” (factor loading: 0.69); (ii) “I tell myself I shouldn’t be thinking the way I’m thinking” (factor loading: 0.67); (iii) “I think some of my emotions are bad or inappropriate and I shouldn’t feel them” (factor loading: 0.73). The Spanish NJ-FFMQ version has an excellent internal reliability (Cronbach's α = 0.91) [50] and the internal reliability of the 3-items in the current study at session 1 was good (Cronbach's α = 0.81).
Body awareness
It was assessed with the Body Awareness of Scale Body Connection (BA-SBC), which measures the conscious attention to sensory signals of the state of the body, such as the sensation of tension or relaxation [39]. Items of the Spanish BA-SBC version was used in the current study [51]. These items were: (i) “I take my body's signals to understand how I feel” (factor loading: 0.83); (ii) “I listen to my body's information about my emotional state” (factor loading: 0.85); (iii) “When I am tense, I pay attention to where the tension is concentrated in my body” (factor loading: 0.72). The Spanish BA-SBS has a good internal reliability (Cronbach's α = 0.86) [50]. The 3-items scale used in the current study also showed good internal reliability at session 1 (Cronbach's α = 0.84).
Attention awareness
It was assessed with the Mindfulness Attention Awareness Scale (MAAS) [52]. It is a 15-item self-reported questionnaire, which measures an individual’s awareness of their experience in the present moment, in contrast to having automated behaviors. Items of the Spanish MAAS version were used in the current study [53]. These items were: (i) "I drive places on ‘automatic pilot’ and then wonder why I went there" (factor loading: 0.77); (ii) "I find myself doing things without paying attention" (factor loading: 0.71); (iii) "I snack without being aware that I’m eating" (factor loading: 0.69). Both the original version [52] and the Spanish version [53] present high internal reliability (Cronbach’s α = 0.82 and 0.89, respectively). In the present study, the 3-items scale showed an acceptable internal reliability at session 1 (Cronbach's α = 0.71).
Data analysis
First, descriptive analyses of the participants were conducted. Second, pre- and post-intervention correlations were calculated to determine baseline and post-treatment relationships between mechanism of change and ED. Third, multilevel modeling (MLM) analyses with a restricted maximum likelihood (REML) estimation method and with a time-lagged approach were conducted to examine the temporal dynamics over time between the proposed mechanism of change (i.e., mediators) and ED. MLM allows modeling changes in the measures of interest over time and time-lagged predictions allows exploring the association of a previous time point measure (i.e., time x) with a later time point measure (i.e., time x + 1). For these analyses, the between- and within-person variability was disaggregated, that is recommended for multilevel models with repeated measures data [20]. To calculate the within-person effects (i.e., level 1), the person-mean-centered was calculated by subtracting the participant-level mean of all time points (i.e., each participant's mean from session 1 to 9) from each participant's score at each time point. Thus, scores at each time point become a deviation score, representing the person's deviation from her own average at that time point. To obtain the between-person effects (i.e., level 2), the grand-mean-centered was calculated by subtracting the sample average of all participant means from the participant-level mean. Thus, the participant-level mean represents the person's deviation from the total sample average [54]. This approach is recommended to interpret the parameters in MLM [55]. Then, it was estimated whether the within- and between-person effects of mechanisms (i.e., decentering, nonjudgment, body awareness and attention awareness) at session x predicted changes in ED at session x + 1, over mindfulness skills training. The reverse direction was also explored to assess the bidirectional relationship. That is, whether within- and between-person effects of ED level at session x predicted changes in the proposed mechanisms of change at session x + 1.
Fourth, cross-level interactions were conducted to assess the moderating role of decentering between the association of the other mechanisms and ED. A cross-level interaction occurs when a level 2 variable (i.e., between-person) moderates the magnitude of a level 1 association (i.e., within-person) [55]. Separate MLM analyses were performed to explore whether the between-person effect of decentering (level 2) moderates the within-person effects of nonjudgment, body awareness and attention awareness (level 1) on the prediction of ED. Significant interactions were probed by testing the simple slopes of each mechanism (e.g., nonjudgment) on ED at high and low levels of decentering capacity (i.e., ± 1 SD) [56].
In all MLM analyses the participants' intercept was defined as random effects. The partR2 package was used [57] to estimate the marginal and conditional R2 [58]. The coefficient of determination R2 was used to interpret the effect size of the models, which were classified as weak (0.02-0.13), medium (0.13-0.26) and large (> 0.26) [59]. All models were tested with the lme4 package [60] in RStudio and IBM SPSS statistics (version 24) was used for descriptive analyses.
Results
Characteristics of the sample
A total of 75 outpatients with a diagnosis of BPD attended a mindfulness skills training (Mage = 27.15 [range 18–53], 93.3% female). A total of 499 observations were obtained (Mean = 4.95, SD = 2.60). Most participants were working (33%) or studying (32%) at the time of the evaluation (see Table 1).
Regarding the weekly practice of the tasks assigned during training, the participants practiced mindfulness skills for a median of 3 days (M = 2.80, SD = 1.97, range = 0–7) and a mean of 27.90 min per week (SD = 27.81, range = 0–180). In addition, practice time increased over the course of the training, both in days (b = 0.16, SE = 0.02, p < 0.001) and minutes (b = 1.27, SE = 0.38, p < 0.01).
Table 2 shows the correlations between ED (DERS-18) and the mechanisms of change proposed in sessions 1 and 9 of the mindfulness training. Correlations were significant both at baseline (r range from -0.306 to -0.487) and at the end of the training (r range from -0.573 to -0.642). However, more robust correlations were observed in session 9 (moderate to high).
Changes in emotion dysregulation and mechanisms of change during mindfulness training
The effects of mindfulness training on ED levels and mechanisms of change were assessed. The mindfulness training (sessions from 1 to 9) prompted improvements in participants' ED over time (b = -0.82, p < 0.001) as well as an increase in each of the mechanisms assessed (decentering: b = 0.13, p < 0.001; nonjudgment: b = 0.20, p < 0.001; body awareness: b = 0.12, p < 0.01; attention awareness: b = 0.14, p < 0.01). See Fig. 1 to visualize the trajectory of the mechanisms of change session by session. Also, Table S1 (in additional file 1) presents the mean and standard deviation of all outcomes (i.e., mechanisms and ED) at each time point.

Session-by-session trajectory of mechanisms of change through mindfulness skills training. The gray area represents the confidence intervals (standard error). The horizontal line represents the mean of the measures of all time points (mean-centered)
Subsequently, it was explored whether improvements in ED and gains in mechanisms of change over mindfulness training were moderated by sociodemographic variables (e.g., age, sex) or baseline clinical variables (i.e., score in diagnostic interview for borderlines [DIB-R], borderline symptoms [BSL-23]; past suicide acts, past non-suicidal self-injury). Improvements in ED and gains in mechanisms were not moderated by sociodemographic variables (all p-values > 0.11) or by baseline clinical measures (all p-values > 0.18). Only a trend moderating effect of baseline borderline symptoms (i.e., BSL-23) on the session-by-session trajectory of ED was found (b = -0.01, SE = 0.009, p = 0.053).
Effects of mechanisms of change on emotion dysregulation over time
The time-lagged effects of decentering, nonjudgment, body awareness and attention awareness on ED was explored. In these analyses, the effect of both between and within person mechanisms on ED was tested (see Table 3). Consistent with our hypothesis, greater both within- and between-person effect of nonjudgment and body awareness at session x predicted improvements in ED at session x + 1. This means that when participants reported higher capacity of nonjudgment and body awareness than their personal average (i.e., higher-than-usual), and more than the total sample average, they also showed an improvement/reduction in their ED level at the following week. Similarly, greater between-person (but not within-person) effects of decentering and attention awareness at session x also predicted improvements in ED at session x + 1. Therefore, when participants reported higher capacity of decentering and attention awareness than the total sample average, they showed improvements in their ED in the following week (see also Table 3). Medium-to-large effects size were obtained in all models (R2: 0.20-0.31).
Subsequently, both the between- and within-person effect was assessed of all mechanisms on ED in the same model (see Table 4). Greater between-person effects of decentering, nonjudgment, and attention awareness, as well as greater within-person effects of body awareness in session x predicted improvements in ED at the following week (i.e., session x + 1). The variance of the time lagged fixed effects (i.e., the four mechanisms at session x) explained 52% of the total variance of DERS in the following week, yielding a large effect size.
In addition, since significant correlations were observed among the predictors, multicollinearity was assessed in all models by calculating the variance inflation factor (VIF). All VIF values were < 2, indicating that there were no multicollinearity problems [61].
Effects of emotion dysregulation on mechanism of change over time
We then explored the lagged effects of ED on each mechanism of change to determine the possibility of bidirectionality (see Table 3). Higher within- and between-person level of ED at session x predicted decreased capacity of decentering, nonjudgment and attention awareness at session x + 1. However, only higher between-person level of ED at session x predicted decreased body awareness at session x + 1. This means that when participants had a week with more emotion regulation difficulties than their personal average, they were less able to increase decentering, nonjudgment and attention awareness at the following week. In addition, when participants had more ED than the total sample average, they were also less able to increase body awareness in the following week. In all models, medium-to-large effects size were obtained (R2: 0.19-0.30). Thus, a bidirectional temporal dynamic between the proposed mechanisms and ED was found. Again, no multicollinearity problems were found (all VIF < 2).
Decentering moderates the association of body awareness, attention awareness, and nonjudgment with emotion dysregulation
Subsequently, the moderating role of decentering as a metacognitive process on the association between nonjudgment, body awareness, attention awareness, and ED was assessed. In these analyses, the between-person effects of decentering as moderator, the within-person effects of nonjudgment, body awareness and attention awareness as predictors, and ED as outcome were used [55]. First, an interaction effect was found between nonjudgment x decentering in predicting ED (b = -0.41, SE = 0.09, p < 0.001). Simple slope analysis showed that within-person increase in nonjudgment predicted improvements in ED more strongly among participants with high decentering (b = -2.37, SE = 0.31, p < 0.001) than among participants with low decentering (B = -0.71, SE = 0.22, p < 0.01; see Fig. 2).

Decentering moderating the association between Nonjudging of Inner Experience and Emotion Dysregulation
Second, an interaction effect was also found between body awareness x decentering in predicting ED (b = -0.25, SE = 0.08, p < 0.01). Simple slope analysis showed that a within-person increase in body awareness predicted improvements in ED more strongly among participants with high decentering (B = -1.88, SE = 0.30, p < 0.001) than among participants with low decentering (B = -0.84, SE = 0.21, p < 0.001; see Fig. 3).

Decentering moderating the association between Body Awareness and Emotion Dysregulation
There was no significant moderating effect of decentering on the association between attention awareness and ED (b = -0.09, SE = 0.09, p = 0.31). In addition, there was no evidence that a within-person effect of decentering was moderated by the between-person effects of nonjudgment, body awareness or attention awareness (all p-value > 0.69).
Discussion
This study aimed to explore how mindfulness DBT skills training improves emotion regulation in people with BPD. A main finding was that participants who at a given week increased their capacity for nonjudgment of inner experience and body awareness more than their own personal average (i.e., within-person effects), and those who increased their capacity for decentering and attention awareness more than the total sample average (i.e., between-person effects), showed improvements in ED at the following week. Moreover, as expected, a bidirectional relationship was found. That is, when participants were more emotionally dysregulated than their own usual state, they showed less gains in decentering, nonjudgment and attention awareness at the following week. Lastly, decentering moderated the relationship between nonjudgment and body awareness with ED, such that increased nonjudgment and body awareness predicted improvements in ED more strongly in those participants with high decentering capacity compared with those participants with low decentering. Therefore, the hypotheses of the present study were mostly confirmed, mainly in the effect of each of the proposed mechanisms on ED (hypothesis 1), specifically a within-person effects for nonjudgment of inner experience and body awareness on ED (hypothesis 2) and evidence for the moderating role of decentering (hypothesis 3).
The present study is an advance in identifying the possible mechanisms of change involved in a mindfulness DBT skills training as a stand-alone intervention to improve ED in BPD outpatients, using ad hoc methodology [19]. Previous studies reporting the mechanisms of change involved in a DBT skills training agree that greater use of behavioral skills mediates changes in ED [9]. Specifically, when participants use more DBT skills than their own personal average, their emotion regulation capacity improves [23, 24]. A recent study explored this question only in a DBT mindfulness skills training and also found that greater use of behavioral skills (i.e., mindfulness practice) predicted improvements in ED [26]. Current results extend previous findings and provide further evidence to report specifically what are the mechanisms of change involved in a mindfulness skill training.
Specifically, the within-person effects of nonjudgment and body awareness predicted subsequent improvements in ED. Previous empirical studies support these findings, showing that acceptance without judgment mediated changes in psychiatric symptoms and frequency of nonsuicidal self-injury –ED related outcomes– following DBT skills training [36, 37]. Similarly, Eisenlohr-Moul et al. [38] found that fluctuations in nonjudgment of internal experience over time (i.e., at within-person level) predicted lower borderline symptoms in women with BPD features. The tendency to judge internal experience is characteristic in individuals with BPD and contributes to emotional regulation problems [35, 62]. Therefore, strategies focused on improving this ability are key in the treatment of BPD [14]. The role of body awareness as a mechanism of change has been less studied in DBT interventions and the evidence obtained from other mindfulness-based interventions shows significant but small effects [63]. However, our results support the role of body awareness as a relevant mechanism to foster emotion regulation in BPD. For example, some of the items used to assess body awareness ("I take my body's signals to understand how I feel") highlight the importance of the body (e.g., attending to bodily sensations) to facilitate awareness of one's emotions and feelings, which is a pre-condition for regulating them [27].
An additional finding in the current study was that decentering ability modulated the strength of the association between nonjudgment, body awareness, and ED, such that high decentering capacity reinforced the effect of these mechanisms on reducing ED. This result is consistent with previous studies [44] and highlights the role of decentering as a metacognitive capacity that promotes emotion regulation [32]. Decentering is described as a metacognitive awareness that helps us disidentify from the contents of our experience so that instead of fusing with them (e.g., "I am not lovable"), we can perceive them as transient mental events (e.g., "I am having a thought of not being lovable") [31]. Given that decentering is diminished in individuals with BPD [49], a goal of mindfulness skills in DBT is to increase meta-awareness of mental contents by enhancing the ability to detach from thoughts and sensations, and decreasing reactivity to mental events (14). Furthermore, the findings support that decentering not only allows for greater meta-awareness of mental contents but also of bodily sensations, but not inversely (i.e., moderating role), suggesting that observing judgmental thought patterns and intense bodily sensations (e.g., associated with distress) from a decentered perspective may help reduce emotional reactivity [64].
As noted, a bidirectional temporal dynamic between the proposed mechanisms and ED was found. Interestingly, previous studies also found a bidirectional relationship between poorer psychosocial functioning and ED [54], and between mindfulness practice skills and ED [26] in people with BPD who attended DBT skill training. These antecedents suggest that when participants with BPD had a previous high level of ED, they tended to practice less and, therefore, improved less in the proposed mechanisms. One explanation for this effect is that mindfulness practice is mood-dependent [65] and therefore practicing skills is more difficult when one is emotionally dysregulated. This leads to a challenge for clinicians when intervening with individuals diagnosed with BPD who usually have pervasive patterns of ED. However, part of the effectiveness of DBT skill training is that participants are taught to express and manage difficult emotional states within a structured group setting in which the therapist models skills and provides positive feedback and reinforcement [21]. This encourages exposure to difficult experiences rather than avoidance or fusion with them [33]. In this way, patients undergoing DBT skills training may feel more capable to apply their newly learned skills to the real-world. In addition, the DBT skill set also includes distress tolerance skills when elevated emotional dysregulation hinders access to mindfulness skills [14].
The results of this study may have some clinical implications and allow for possible causal interpretations of the mechanisms that favor improvements in ED after mindfulness skill training. Nonjudgment and body awareness increases were related to within-person effects, whereas increases in decentering and attention awareness were only related to between-person effects. These differences suggest that certain facets of mindfulness are more attitudinal and may be more sensitive to within-person variability (i.e., capacity for nonjudging) while other aspects are more stable and may be related to between-person individual differences (e.g., capacity for paying attention or perspective taking) [37]. In light of the results, we hypothesize that mindfulness training in DBT is promoting both levels. However, changes at within-person level, such as learning to observe one's own experience without judgment, appear to be relevant psychological processes for fostering greater emotion regulation. Therefore, clinicians can optimize their interventions by emphasizing these processes of change in clients who exhibit high levels of self-judgment or self-criticism, as is often observed in individuals with BPD.
Importantly, when all four proposed mechanisms of change were included in the same model, they explained 52% of the variance of changes in ED in the following week. Thus, these mechanisms appear to complement each other and therapists could consider this information to improve the efficacy of BPD-oriented treatments. In addition, decentering capacity acted as a metacognitive process that enhances the effect of the other mechanisms on ED. This also suggests that therapists may use strategies that increase the decentering ability in BPD treatments.
The present study has some limitations that should be considered when interpreting the results. First, a single-arm non-randomized trial was implemented, that limits the generalizability of our conclusions. Second, to facilitate the weekly evaluation of the participants, the 3 most representative items of each measure (i.e., mechanisms of change) was used. However, these items may not be fully representative of the overall construct and may therefore increase risk of false negatives (i.e., type II error). Third, a measure of ED was used as the outcome. However, ED can also be considered as a process that contributes to the development or maintenance of psychopathology [66]. Therefore, a repeated measure of borderline symptoms would have enriched the results by exploring how mechanisms and ED session-by-session predict the trajectory of borderline symptoms after mindfulness skills training. Fourth, only the moderating role of decentering was tested and whether decentering was not moderated by the other mechanisms. However, we did not explore the possible moderating role of the other mechanisms among themselves and future studies could explore this issue. Fifth, the MLM analyses used did not take into account autoregressive effects (e.g., whether the change in ED at a specific time point could be influenced by an earlier time point of the same measure), potentially introducing bias into the findings [67]. Future studies should address the autoregressive effect when analyzing repeated measures data. Lastly, the sample was mostly composed of women. It is desirable that future studies consider more representative samples of men with BPD.
Conclusions
Knowing how a psychological intervention works (i.e., the mechanisms) is key to understanding the processes involved in therapeutic change. A recommended methodology for exploring this issue in a framework of multilevel modeling with repeated measures is to disaggregate the total effect of predictors into the between- and within-person effects [20]. This approach not only allows to obtain information about the between-person differences (e.g., those who frequently practice nonjudgment of their internal experience improve in ED compared to those who practice less) but also provides information into within-person processes (e.g., individuals who practice nonjudgment of their experience beyond their habitual tendency, demonstrate improvements in ED). The present study provides preliminary evidence of the mechanisms of change underlying mindfulness skills training. When treating emotional dysregulation in BPD patients, therapists could benefit from this information by promoting within-person processes such as nonjudgment and body awareness, as well as decentering strategies that strengthen the effects of these mechanisms. Finally, understanding how mindfulness DBT skills training works can help optimize treatment for BPD.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- BPD:
-
Borderline Personality Disorder
- ED:
-
Emotion Dysregulation
- DBT:
-
Dialectical Behavior Therapy
- SCID II:
-
Structured Clinical Interview for DSM IV axis II Disorders
- DIB-R:
-
Revised Diagnostic Interview for Borderlines
- DERS-18:
-
Brief Version of the Difficulties in Emotion Regulation Scale
- EQ:
-
Experiencing Questionnaire
- NJ-FFMQ:
-
Nonjudging of Inner Experience sub-scale of Five Facets Mindfulness Questionnaire
- BA-SBC:
-
Body Awareness of Scale Body Connection
- MAAS:
-
Mindfulness Attention Awareness Scale
- MLM:
-
Multilevel modeling
- REML:
-
Restricted maximum likelihood
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, Fifth Edition, Text Reviseds. Fifth Edition. American Psychiatric Association.; 2022. Available from: https://dsm.psychiatryonline.org/doi/book/10.1176/appi.books.9780890425787. Cited 2011 Nov 10.
Trull TJ, Jahng S, Tomko RL, Wood PK, Sher KJ. Revised NESARC personality disorder diagnoses: gender, prevalence, and comorbidity with substance dependence disorders. J Pers Disord. 2010;24(4):412–26. https://doi.org/10.1521/pedi.2010.24.4.412.
McGlashan TH, Grilo CM, Skodol AE, et al. The collaborative longitudinal personality disorders study: baseline Axis I/II and II/II diagnostic co-occurrence. Acta Psychiatr Scand. 2000;102(4):256–64. https://doi.org/10.1034/j.1600-0447.2000.102004256.x.
Alvarez-Tomás I, Soler J, Bados A, et al. Long-term course of borderline personality disorder: a prospective 10-year follow-up study. J Pers Disord. 2017;31(5):590–605. https://doi.org/10.1521/pedi_2016_30_269.
Leichsenring F, Fonagy P, Heim N, et al. Borderline personality disorder: a comprehensive review of diagnosis and clinical presentation, etiology, treatment, and current controversies. World Psychiatry. 2024;23(1):4–25. https://doi.org/10.1002/wps.21156.
Pascual JC, Martín-Blanco A, Soler J. Twenty-year trends in the psychopharmacological treatment of outpatients with borderline personality disorder: a cross-sectional naturalistic study in Spain. CNS Drugs. 2021;35(9):1023–32. https://doi.org/10.1007/s40263-021-00852-7.
Carpenter RW, Trull TJ. Components of emotion dysregulation in borderline personality disorder: a review. Curr Psychiatry Rep. 2013;15(1):335. https://doi.org/10.1007/s11920-012-0335-2.
Glenn CR, Klonsky ED. Emotion dysregulation as a core feature of borderline personality disorder. J Pers Disord. 2009;23(1):20–8. https://doi.org/10.1521/pedi.2009.23.1.20.
Neacsiu AD, Eberle JW, Kramer R, Wiesmann T, Linehan MM. Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: a pilot randomized controlled trial. Behav Res Ther. 2014;59:40–51. https://doi.org/10.1016/j.brat.2014.05.005.
Bohus M, Stoffers-Winterling J, Sharp C, Krause-Utz A, Schmahl C, Lieb K. Borderline personality disorder. Lancet. 2021;398(10310):1528–40. https://doi.org/10.1016/S0140-6736(21)00476-1.
Chapman AL. Borderline personality disorder and emotion dysregulation. Dev Psychopathol. 2019;31(3):1143–56. https://doi.org/10.1017/S0954579419000658.
2018 surveillance of personality disorders (NICE guidelines CG77 and CG78) [Internet]. London: National Institute for Health and Care Excellence (NICE); 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK550289/.
Storebø OJ, Stoffers-Winterling JM, Völlm BA, et al. Psychological therapies for people with borderline personality disorder. Cochrane Database Syst Rev. 2020;5(5):CD012955. https://doi.org/10.1002/14651858.CD012955.pub2. Published 2020 May 4.
Linehan MM. Skills training manual for treating borderline personality disorder. New York: Guilford Press; 1993.
Carmona i Farrés C, Elices M, Soler J, Domínguez-Clavé E, Pomarol-Clotet E, Salvador R, Pascual JC. Effects of mindfulness training on borderline personality disorder: impulsivity versus emotional dysregulation. Mindfulness. 2019;10(7):1243-1254. https://doi.org/10.1007/s12671-018-1071-4.
Schmidt C, Soler J, Carmona I Farrés C, et al. Mindfulness in borderline personality disorder: decentering mediates the effectiveness. Psicothema. 2021;33(3):407–14.
Kazdin AE. Mediators and mechanisms of change in psychotherapy research. Annu Rev Clin Psychol. 2007;3:1–27. https://doi.org/10.1146/annurev.clinpsy.3.022806.091432.
Kazdin AE. Evidence-based psychotherapies I: qualifiers and limitations in what we know. S Afr J Psychol. 2014;44(4):381–403. https://doi.org/10.1177/0081246314533750.
Holmes EA, Ghaderi A, Harmer CJ, et al. The lancet psychiatry commission on psychological treatments research in tomorrow’s science. Lancet Psychiatry. 2018;5(3):237–86. https://doi.org/10.1016/S2215-0366(17)30513-8.
Wang LP, Maxwell SE. On disaggregating between-person and within-person effects with longitudinal data using multilevel models. Psychol Methods. 2015;20(1):63–83. https://doi.org/10.1037/met0000030.
Chapman AL, Owens L. Mechanisms of change in dialectical behavior therapy. In: Bedics J, editor. The handbook of dialectical behavior therapy: theory, research, and evaluation. Elsevier Academic Press; 2020. p. 51–69. https://doi.org/10.1016/B978-0-12-816384-9.00003-8.
Asarnow JR, Berk MS, Bedics J, et al. Dialectical behavior therapy for suicidal self-harming youth: emotion regulation, mechanisms, and mediators. J Am Acad Child Adolesc Psychiatry. 2021;60(9):1105-1115.e4. https://doi.org/10.1016/j.jaac.2021.01.016.
Southward MW, Howard KP, Cheavens JS. Less is more: decreasing the frequency of maladaptive coping predicts improvements in DBT more consistently than increasing the frequency of adaptive coping. Behav Res Ther. 2023;163:104288. https://doi.org/10.1016/j.brat.2023.104288.
Wyatt KP, Eberle JW, Ruork AK, Neacsiu AD. Mechanisms of change in treatments for transdiagnostic emotion dysregulation: the roles of skills use, perceived control and mindfulness. Clin Psychol Psychother. 2023;30(6):1380–92. https://doi.org/10.1002/cpp.2879.
Barnicot K, Gonzalez R, McCabe R, Priebe S. Skills use and common treatment processes in dialectical behaviour therapy for borderline personality disorder. J Behav Ther Exp Psychiatry. 2016;52:147–56. https://doi.org/10.1016/j.jbtep.2016.04.006.
Schmidt C, Soler J, Vega D, Pascual JC. Practice matters: the role of mindfulness skills in emotion dysregulation in borderline personality disorder. J Context Behav Sci. 2024;32:100756. https://doi.org/10.1016/j.jcbs.2024.100756.
Hölzel BK, Lazar SW, Gard T, Schuman-Olivier Z, Vago DR, Ott U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect Psychol Sci. 2011;6(6):537–59. https://doi.org/10.1177/1745691611419671.
Tang YY, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015;16(4):213–25. https://doi.org/10.1038/nrn3916.
Carmody J, Baer RA, L B Lykins E, Olendzki N. An empirical study of the mechanisms of mindfulness in a mindfulness-based stress reduction program. J Clin Psychol. 2009;65(6):613-626. https://doi.org/10.1002/jclp.20579.
Fresco DM, Moore MT, van Dulmen MH, et al. Initial psychometric properties of the experiences questionnaire: validation of a self-report measure of decentering. Behav Ther. 2007;38(3):234–46. https://doi.org/10.1016/j.beth.2006.08.003.
Bernstein A, Hadash Y, Lichtash Y, Tanay G, Shepherd K, Fresco DM. Decentering and related constructs: a critical review and metacognitive processes model. Perspect Psychol Sci. 2015;10(5):599–617. https://doi.org/10.1177/1745691615594577.
O’Toole MS, Renna ME, Mennin DS, Fresco DM. Changes in decentering and reappraisal temporally precede symptom reduction during emotion regulation therapy for generalized anxiety disorder with and without co-occurring depression. Behav Ther. 2019;50(6):1042–52. https://doi.org/10.1016/j.beth.2018.12.005.
Wu JL, Hamilton JL, Fresco DM, Alloy LB, Stange JP. Decentering predicts attenuated perseverative thought and internalizing symptoms following stress exposure: a multi-level, multi-wave study. Behav Res Ther. 2022;152:104017. https://doi.org/10.1016/j.brat.2021.104017.
Carpenter JK, Conroy K, Gomez AF, Curren LC, Hofmann SG. The relationship between trait mindfulness and affective symptoms: a meta-analysis of the Five Facet Mindfulness Questionnaire (FFMQ). Clin Psychol Rev. 2019;74:101785. https://doi.org/10.1016/j.cpr.2019.101785.
Wupperman P, Neumann CS, Whitman JB, Axelrod SR. The role of mindfulness in borderline personality disorder features. J Nerv Ment Dis. 2009;197(10):766–71. https://doi.org/10.1097/NMD.0b013e3181b97343.
Krantz LH, McMain S, Kuo JR. The unique contribution of acceptance without judgment in predicting nonsuicidal self-injury after 20-weeks of dialectical behaviour therapy group skills training. Behav Res Ther. 2018;104:44–50. https://doi.org/10.1016/j.brat.2018.02.006.
Zeifman RJ, Boritz T, Barnhart R, Labrish C, McMain SF. The independent roles of mindfulness and distress tolerance in treatment outcomes in dialectical behavior therapy skills training. Personal Disord. 2020;11(3):181–90. https://doi.org/10.1037/per0000368.
Eisenlohr-Moul T, Peters JR, Chamberlain KD, Rodriguez M. Weekly fluctuations in nonjudging predict borderline personality disorder feature expression in women. J Psychopathol Behav Assess. 2016;38(1):149–57. https://doi.org/10.1007/s10862-015-9505-y.
Price CJ, Thompson EA. Measuring dimensions of body connection: body awareness and bodily dissociation. J Altern Complement Med. 2007;13(9):945–53. https://doi.org/10.1089/acm.2007.0537.
Carmody J, Baer RA. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J Behav Med. 2008;31(1):23–33. https://doi.org/10.1007/s10865-007-9130-7.
Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13(1):27–45. https://doi.org/10.1177/1073191105283504.
Schmitz M, Bertsch K, Löffler A, Steinmann S, Herpertz SC, Bekrater-Bodmann R. Body connection mediates the relationship between traumatic childhood experiences and impaired emotion regulation in borderline personality disorder. Borderline Personal Disord Emot Dysregul. 2021;8(1):17. https://doi.org/10.1186/s40479-021-00157-7. Published 2021 May 17.
Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008;12(4):163–9. https://doi.org/10.1016/j.tics.2008.01.005.
First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structured clinical interview for DSM-IV Axis II Personality Disorders (SCID-II). Washington: American Psychiatric Press, Inc; 2007.
Barrachina J, Soler J, Campins MJ, et al. Validación de la versión española de la Diagnostic Interview for Bordelines-Revised (DIB-R) [Validation of a Spanish version of the Diagnostic Interview for Bordelines-Revised (DIB-R)]. Actas Esp Psiquiatr. 2004;32(5):293–8.
Soler J, Vega D, Feliu-Soler A, et al. Validation of the Spanish version of the borderline symptom list, short form (BSL-23) [published correction appears in BMC Psychiatry. 2016 Dec 1;16(1):429]. BMC Psychiatry. 2013;13:139. https://doi.org/10.1186/1471-244X-13-139. Published 2013 May 14.
Elices M, Pascual JC, Portella MJ, et al. Impact of mindfulness training on borderline personality disorder: a randomized trial. Mindfulness. 2016;7(3):584–95. https://doi.org/10.1007/s12671-016-0492-1.
Victor SE, Klonsky ED. Validation of a brief version of the Difficulties in Emotion Regulation Scale (DERS-18) in five samples. J Psychopathol Behav Assess. 2016;38(4):582–9. https://doi.org/10.1007/s10862-016-9547-9.
Soler J, Franquesa A, Feliu-Soler A, et al. Assessing decentering: validation, psychometric properties, and clinical usefulness of the experiences questionnaire in a Spanish sample. Behav Ther. 2014;45(6):863–71. https://doi.org/10.1016/j.beth.2014.05.004.
Cebolla A, García-Palacios A, Soler J, Guillen V, Baños R, Botella C. Psychometric properties of the Spanish validation of the Five Facets of Mindfulness Questionnaire (FFMQ). Eur J Psychiatry. 2012;26(2):118–26. https://doi.org/10.4321/S0213-61632012000200005.
Quezada-Berumen LC, González-Ramírez MT, Cebolla A, Soler J, Garcia-Campayo J. Body awareness and mindfulness: validation of the Spanish version of the scale of body connection. Actas Esp Psiquiatr. 2014;42(2):57–67.
Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–48. https://doi.org/10.1037/0022-3514.84.4.822.
Soler J, Tejedor R, Feliu-Soler A, et al. Psychometric proprieties of Spanish version of Mindful Attention Awareness Scale (MAAS). Actas Esp Psiquiatr. 2012;40(1):19–26.
Wilks CR, Korslund KE, Harned MS, Linehan MM. Dialectical behavior therapy and domains of functioning over two years. Behav Res Ther. 2016;77:162–9. https://doi.org/10.1016/j.brat.2015.12.013.
Enders CK, Tofighi D. Centering predictor variables in cross-sectional multilevel models: a new look at an old issue. Psychol Methods. 2007;12(2):121–38. https://doi.org/10.1037/1082-989X.12.2.121.
Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park: Sage Publications; 1991.
Stoffel MA, Nakagawa S, Schielzeth H. rptR: Repeatability estimation and variance decomposition by generalized linear mixed-effects models. Methods Ecol Evol. 2017;8:1639–44. https://doi.org/10.1111/2041-210X.12797.
Nakagawa S, Schielzeth H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods Ecol Evol. 2013;4(2):133–42. https://doi.org/10.1111/j.2041-210x.2012.00261.x.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: Lawrence Erlbaum Associates, Publishers; 1988.
Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67(1):1–48. https://doi.org/10.18637/jss.v067.i01.
Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. 7th ed. New York: Pearson; 2010.
Elices M, Pascual JC, Carmona C, et al. Correction to: exploring the relation between childhood trauma, temperamental traits and mindfulness in borderline personality disorder. BMC Psychiatry. 2018;18(1):284. https://doi.org/10.1186/s12888-018-1834-4. Published 2018 Sep 4.
Treves IN, Tello LY, Davidson RJ, Goldberg SB. The relationship between mindfulness and objective measures of body awareness: a meta-analysis. Sci Rep. 2019;9(1):17386. https://doi.org/10.1038/s41598-019-53978-6. Published 2019 Nov 22.
Carpenter JK, Sanford J, Hofmann SG. The effect of a brief mindfulness training on distress tolerance and stress reactivity. Behav Ther. 2019;50(3):630–45. https://doi.org/10.1016/j.beth.2018.10.003.
Elices M, Tejedor R, Pascual JC, Carmona C, Soriano J, Soler J. Acceptance and present-moment awareness in psychiatric disorders: is mindfulness mood dependent? Psychiatry Res. 2019;273:363–8. https://doi.org/10.1016/j.psychres.2019.01.041.
Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. 2010;30(2):217–37. https://doi.org/10.1016/j.cpr.2009.11.004.
Falkenström F, Solomonov N, Rubel JA. How to model and interpret cross-lagged effects in psychotherapy mechanisms of change research: a comparison of multilevel and structural equation models. J Consult Clin Psychol. 2022;90(5):446–58. https://doi.org/10.1037/ccp0000727.
Acknowledgements
This study was supported by Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM).
Funding
This study was supported by the Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM) and by a grant from Instituto de Salud Carlos III [PI19/00087 and PI21/00505] and co-financed by the European Regional Development Fund (ERDF). CS was supported by the National Agency for Research and Development (ANID) / Scholarship Program / Doctorado Becas Chile [reference number 72190624]. SN was supported by a fellowship from “La Caixa” Foundation [ID 100010434; code: LCF/BQ/DR21/11880013].
Author information
Authors and Affiliations
Contributions
CS, JS, JCP, designed the study. JCP and LA recruited the participants. JS and DV performed the interventions. CS and SN collected and interpreted the data analyses. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Hospital de la Santa Creu i Sant Pau. Informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Schmidt, C., Soler, J., Vega, D. et al. How does mindfulness skills training work to improve emotion dysregulation in borderline personality disorder?. bord personal disord emot dysregul 11, 22 (2024). https://doi.org/10.1186/s40479-024-00265-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40479-024-00265-0