
Abstract
Purpose
Patients undergoing knee surgery are at high risk for deep vein thrombosis (DVT), which is infrequent but potentially life-threatening. It has not been identified how to efficiently detect high-risk DVT while minimizing bleeding complications from anticoagulation. We hypothesized that the degree of activation of thrombotic markers may correlate with the size of the thrombus. Therefore, we investigated the correlation between thrombotic markers and DVT thrombus volume in patients after knee surgery.
Methods
This retrospective study involved 29 patients who underwent around knee osteotomy or total / unicompartmental knee arthroplasty from 2018 to 2020. Fibrin monomer complex (FMC) at 1, and 7 days after surgery, and D-dimer at 4, and 7 days after surgery were investigated. In addition, the volume of DVT was estimated with ultrasonography at the 7 days after surgery. Body mass index, surgical time, and total volume of blood loss were also evaluated. Factors related to thrombus volume were examined statistically.
Results
Nine patients (31.0%) exhibited asymptomatic distal DVT, whereas 1 patient (3.4%) experienced asymptomatic proximal DVT. No patients had pulmonary embolism. Statistical analysis showed that only FMC concentration on postoperative day 1 was significantly correlated with thrombus volume (p < 0.001, 95% confidence interval 0.41 to 0.839, r = 0.679).
Conclusions
The FMC concentration was a useful early indicator of deep vein thrombosis after knee surgery. Monitoring the FMC concentration could enable selective identification of patients with a high thrombus volume, which is associated with a high risk for pulmonary embolism.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Several surgical options are available for patients with knee osteoarthritis (OA), such as osteotomy, unicompartmental knee arthroplasty (UKA), and total knee arthroplasty (TKA). The choice of surgery is dictated by the degree of deformation, patient lifestyle and activity level. However, various complications have been reported with these surgeries, including venous thromboembolism (VTE), infections, fractures [1, 2], and loosening of the prosthesis [3]. Among them, VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is particularly dangerous and can be life threatening. Although deaths caused by VTE are rare, they still occur. Without thrombophylaxis, the rate of VTE after TKA is reportedly as high as 40–60% [4, 5]. In addition, recent investigations have reported that the rates of DVT after around knee osteotomy also occur ranging from 21.7–41% [6,7,8].
Due to the potential danger associated with DVT, many studies have examined approaches for its prevention and early detection. Fibrin-related markers such as D-dimer and soluble fibrin (SF) / fibrin monomer complex (FMC) are recognized as laboratory tests to assist in the detection of VTE [9]. A D-dimer value of 7.0 on postoperative day 4 or an SF value of 3.6 on postoperative day 1 have been determined as cut-off values for suggesting DVT in the leg after orthopaedic surgery [10]. Monitoring these fibrin-related markers is often combined with examination of the leg by ultrasonography (US), which is the first-choice imaging modality for DVT screening [11]. However, most thrombi detected during these examinations are distal DVT. For distal DVT that develops under prophylaxis, there is still no strong evidence for initiating or prolonging anticoagulation [12, 13]. It has also been reported that these screenings did not reduce the incidence of symptomatic VTE or fatal PE [14]. Furthermore, anticoagulation for the treatment of detected asymptomatic VTE has been reported to increase the risk of serious bleeding events [15]. For these reasons, several guidelines do not recommend postoperative routine screening for DVT [14, 16, 17]. Although this is partially due to the lack of evidence on the timing and methods of screening, currently there is no screening method that can lead to efficient and appropriate treatment. Nevertheless, we are always awaiting the advent of a screening method that can efficiently detect large, life-threatening VTE.
Since most PE which occurs after knee surgery originates from DVT, the size of the DVT may be related to the severity of PE. When a large thrombus is formed, significant activation of the coagulation/fibrinolysis system occurs. Therefore, we hypothesized that thrombotic markers may correlate with thrombus volume.
Hence, the correlation between thrombotic markers and DVT thrombus volume during the perioperative period in patients who underwent knee surgery was investigated in the present study.
Methods
This retrospective study involved 29 patients who underwent around the knee osteotomy (AKO), TKA, UKA due to medial OA or spontaneous osteonecrosis of the knee from April 2018 to March 2020. A total of 12 men and 17 women were enrolled in the study; mean age of the patients was 68.5 years (range 54–83 years), the number of patients in each surgery were AKO:TKA:UKA = 16:9:4. AKO included medial open-wedge high tibial osteotomy, lateral closed-wedge high tibial osteotomy, distal femoral osteotomy, and the combination of femoral and tibial osteotomy (double-level osteotomy). Tourniquet was used in TKA / UKA. No patients had previous history of DVT or PE, and none of the patients received preoperative anticoagulant therapy. All surgeries were performed by 2 experienced orthopaedic surgeons. All patients received post operative physical prophylaxis. Postoperative anticoagulation (oral edoxaban) was given for 14 days only to TKA and UKA patients according to Japanese insurance indications.
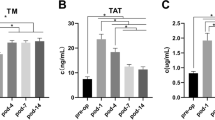
Age, body mass index (BMI), surgical time, and total blood loss during the operation were recorded as the patients’ characteristics. In addition, FMC at 1, and 7 days after surgery (D1, D7), and D-dimer at 4, and 7 days after surgery (D4, D7) were measured.
Duplex doppler US investigations were employed to investigate for the presence of DVT at 7 days after surgery. DVTs were classified as proximal or distal depending on whether the thrombus was located above or below the popliteal vein, respectively. Thrombus volume was calculated by approximation to an elliptic cylinder based on the US measurement [18] (Fig. 1). If several thrombi were present, total thrombus volume was determined by summing respective volumes. Venographic computed tomography (CT) was performed only when proximal DVT was found or when patients experienced chest pain. Finally, the correlation between thrombus volume and age, BMI, operation time, total blood loss during surgery, FMC, and D-dimer was investigated.

Method for estimation of thrombus volume. Thrombus volume was calculated by approximation of the value determined by ultrasonography to an elliptic cylinder [18]. a: Major Axis, b: Minor axis, h: Length. Estimated Thrombus Volume (cm3) = a/2 × b/2 × πh
All data were expressed as mean ± standard deviation (SD). The normal distribution of the evaluation items was tested by Kolmogorov-Smirnov test. Pearson correlation coefficient was used to examine the relationship between each evaluation items and thrombus volume. All statistical analyses were performed using EZR software [19], with p < 0.05 considered statistically significant.
Results
Patients’ characteristics and investigated data are summarized in Table 1. Nine patients (31.0%) had asymptomatic distal DVT, and 1 patient (3.4%) had asymptomatic proximal DVT. In the patient with the proximal DVT, CT scanning confirmed that there was no PE. And none of the other patients had chest pain (Table 2). The incidence of DVT by procedure was 8/16 (50%) in AKO, 2/9 (22.2%) in TKA, 0/4 (0%) in UKA with proximal DVT occurring in TKA patient (Table 3). When compared AKO and arthroplasty patients, there was a tendency toward more DVT occurrence in AKO, but the difference was not significant (p = 0.06). Thrombus locations were as follows: common femoral vein, 1; posterior tibial vein, 3; peroneal vein, 1; soleus vein, 6 (Table 4). One patient had thrombus in both posterior tibial and peroneal vein. There was no complication other than DVT including infection, fracture, or systemic event during the perioperative period.
Kolmogorov-Smirnov test revealed that FMC D1 and D7 were non-normally distributed, but log-normally distributed. So, these data were log-transformed and used for statistical analysis. As a results of Pearson correlation coefficient, only FMC D1 was correlated with the thrombus volume (p < 0.001, 95% confidence interval 0.41 to 0.839, r = 0.679) (Table 5).
Discussion
No markers have been found correlate with the size of post-operative DVT which can result in PE. In the present study, we revealed for the first time that the author know of, FMC D1 was strongly correlated with the volume of DVT thrombus in knee surgery patients. Additionally, routine anticoagulant prophylaxis tended to decrease the prevalence of DVT in patients of TKA/UKA compared to osteotomy patients. However proximal DVT was observed in TKA patient.
Previous report suggested that postoperative routine prophylaxis with anticoagulants has shown some efficacy [20]. However, even under the anticoagulant the prevalence of DVT is still 15% to 30% [21,22,23]. In this study, routine anticoagulant prophylaxis reduced the prevalence of DVT, but proximal DVT still occurred. Because of these facts, there are many reports on postoperative screening method of DVT, although severe PE after orthopaedic surgery is not frequent. Previously reported cut-off values for SF or D-dimer concentrations [9, 10, 24] are useful parameters for early identification of DVT. However, these were negative predictive cut-off values, and DVT identified using these cut-off values are often distal and of low volume. The problem is that, there is no consensus on whether new or extended anticoagulation therapy should be given for these distal DVTs. A recent systematic review showed extended prophylaxis has some efficacy, but concluded that benefit should be weighed against the risk of minor bleeding [25]. Japanese guideline of DVT recommended that, uniform anticoagulation of distal DVT detected by screening should be avoided [12]. So the indication for anticoagulation therapy should be determined based on risk-benefit considerations, but at present the criteria are not clear. Therefore, in our study, we examined factors that correlate with thrombus volume rather than with the presence of DVT. As a result, we found a strong positive correlation between thrombus volume and FMC concentration. A recent study revealed that thrombus volume is strongly correlated with PE severity [26]. So, with the result of present study, the risk of PE can be predicted immediately after surgery only by the blood sampling, and allow us selective intervention only to high risk DVT patients. The results may provide a useful decision criterion for the aforementioned problem with the treatment of distal DVT.
Furthermore, this selective intervention method may have cost-effective advantages. Recent systematic reviews showed that the combination of D-dimer and US are cost-effective method for the diagnosis of DVT [27, 28]. However, D-dimer is usually used to rule-out DVT, and if positive, it is not the criterion for selecting patients to be treated. On the other hand, our screening method, the combination of FMC D1 and US, allows us to select high-risk patients, which can be a criterion for selective intervention. If we can determine not only the presence of DVT, but also the selection of patients to intervene, it may be even more cost-effective than conventional methods of D-dimer and US.
However, the present study has several limitations. First, there is no cut-off value for the thrombus volume causing severe PE. The short-term mortality of PE is reported to be related to the right ventricle / left ventricle ratio as well as the thrombus volume [29], hence thrombus volume that can cause severe PE may vary depending on the patient’s body size. Therefore, the cut-off value for risk discrimination could not be determined. Further research will be necessary to determine the FMC cut-off value for the detection of large thrombus. Second, although US is suitable for DVT screening, it is not 100% sensitive. There are other evaluation methods such as three-dimensional US [30] or CT scanning that are more accurately detect and calculate thrombus volume. However, equipment capable of three-dimensional US is expensive, and CT has the problem of radiation exposure, so the application of these methods for daily screening is limited. We therefore believe that estimating thrombus volume using non-invasive two-dimensional US is more appropriate for clinical DVT screening. Another limitation is small number of patients. We would like to continue further study with more cases in order to improve statistical reliability and to determine cut-off value of FMC D1. Present research will be the first step toward more efficient prevention of PE.
Conclusions
FMC concentration on postoperative day 1 was a useful early indicator of DVT volume after knee surgery. Monitoring FMC could enable selective identification of patients with a high thrombus volume, which is associated with a high risk for pulmonary embolism.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- OA:
-
Osteoarthritis
- TKA:
-
Total knee arthroplasty
- UKA:
-
Unicompartmental knee arthroplasty
- VTE:
-
Venous thromboembolism
- DVT:
-
Deep vein thrombosis
- PE:
-
Pulmonary embolism
- AKO:
-
Around the knee osteotomy
- SF:
-
Soluble fibrin
- FMC:
-
Fibrin monomer complex
- US:
-
Ultrasonography
- BMI:
-
Body mass index
- CT:
-
Computed tomography
- SD:
-
Standard deviation
References
Atrey A, Morison Z, Tosounidis T, Tunggal J, Waddell JP (2012) Complications of closing wedge high tibial osteotomies for unicompartmental osteoarthritis of the knee. Bone Joint Res 1:205–209
Postler A, Lutzner C, Beyer F, Tille E, Lutzner J (2018) Analysis of total knee arthroplasty revision causes. BMC Musculoskelet Disord 19:55
Cherian JJ, Jauregui JJ, Banerjee S, Pierce T, Mont MA (2015) What host factors affect aseptic loosening after THA and TKA? Clin Orthop Relat Res 473:2700–2709
Cordell-Smith JA, Williams SC, Harper WM, Gregg PJ (2004) Lower limb arthroplasty complicated by deep venous thrombosis. J Bone Joint Surg Br 86-B:99–101
Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW et al (2004) Prevention of venous thromboembolism: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 126:338S–400S
Kobayashi H, Akamatsu Y, Kumagai K, Kusayama Y, Ishigatsubo R, Mitsuhashi S et al (2017) The use of factor Xa inhibitors following opening-wedge high tibial osteotomy for venous thromboembolism prophylaxis. Knee Surg Sports Traumatol Arthrosc 25:2929–2935
Kobayashi H, Akamatsu Y, Kumagai K, Kusayama Y, Okuyama H, Hirotomi K et al (2017) Edoxaban is effective in reducing the incidence of asymptomatic phlebographic events following closed-wedge high tibial osteotomy. Orthop Traumatol Surg Res 103:1193–1196
Turner RS, Griffth H, Heatley FW (1993) The incidence of deep-vein thrombosis after upper tibial osteotomy. A venographic study. J Bone Joint Surg Br 75:942–944
Quinlan DJ, Eikelboom JW, Dahl OE, Eriksson BI, Sidhu PS, Hirsh J (2007) Association between asymptomatic deep vein thrombosis detected by venography and symptomatic venous thromboembolismin patients undergoing elective hip or knee surgery. J Thromb Haemost 5:1438–1443
Sudo A, Wada H, Nobori T, Yamada N, Ito M, Niimi R et al (2009) Cut-off values of D-dimer and soluble fibrin for prediction of deep vein thrombosis after orthopaedic surgery. Int J Hematol 89:572–576
Expert Panel on Vascular Imaging, Hanley M, Steigner ML, Ahmed O, Azene EM, Bennett SJ et al (2018) ACR appropriateness criteria suspected lower extremity deep vein thrombosis. J Am Coll Radiol 15:S413–S417
Ito M et al. Guidelines for diagnosis, treatment and prevention of pulmonary thromboembolism and deep vein thrombosis (2017) https://www.j-circ.or.jp/cms/wp-content/uploads/2017/09/JCS2017_ito_h.pdf. Accessed 11 Apr 2022
Kirkilesis G, Kakkos SK, Bicknell C, Salim S, Kakavia K (2020) Treatment of distal deep vein thrombosis. Cochrane Database Syst Rev 4(4):CD013422
Mont MA, Jacobs JJ, Boggio LN, Bozic KJ, Della Valle CJ, Goodman SB et al (2011) Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. J Am Acad Orthop Surg 19:768–776
Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ, American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel (2012) Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141(2 Suppl):7S–47S
Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S et al (2012) Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 141:e278S–e325S
Japanese Orthopedic Association Clinical Guideline Committee, Committee for guideline on the prevention of symptomatic venous thromboembolism (2017) Japanese Orthopaedic association clinical practice guideline on the prevention of venous thromboembolism. Nankodo Co., Ltd, Tokyo
Kurklinsky AK, Kalsi H, Wysokinski WE, Mauck KF, Bhagra A, Havyer RD et al (2011) Fibrin D-dimer concentration, deep vein thrombosis symptom duration, and venous thrombus volume. Angiology. 62:253–256
Kanda Y (2013) Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant 48:452–458
He T, Han F, Wang J, Hu Y, Zhu J (2021) Efficacy and safety of anticoagulants for postoperative thrombophylaxis in total hip and knee arthroplasty: a PRISMA-compliant Bayesian network meta-analysis. PLoS One 16(6):e0250096
Eriksson BI, Wille-Jorgensen P, Kalebo P, Mouret P, Rosencher N, Bosch P et al (1997) A comparison of recombinant hirudin with a low-molecular-weight heparin to prevent thromboembolic complications after total hip replacement. N Engl J Med 337:1329–1335
Mohr DN, Silverstein MD, Murtaugh PA, Harrison JM (1993) Prophylactic agents for venous thrombosis in elective hip surgery: Meta-analysis of studies using venographic assessment. Arch Intern Med 153:2221–2228
Nurmohamed MT, Rosendaal FR, Buller HR, Dekker E, Hommes DW, Vandenbroucke JP et al (1992) Low-molecular-weight heparin versus standard heparin in general and orthopaedic surgery: a meta-analysis. Lancet. 340:152–156
Niimi R, Hasegawa M, Shi DQ, Sudo A (2012) The influence of fondaparinux on the diagnosis of postoperative deep vein thrombosis by soluble fibrin and D-dimer. Thromb Res 130:759–764
Forster R, Stewart M (2016) Anticoagulants (extended duration) for prevention of venous thromboembolism following total hip or knee replacement or hip fracture repair. Cochrane Database Syst Rev 30(3):CD004179
Shen C, Yu N, Wen L, Zhou S, Dong F, Liu M et al (2019) Risk stratification of acute pulmonary embolism based on the clot volume and right ventricular dysfunction on CT pulmonary angiography. Clin Respir J 13:674–682
Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S et al (2006) Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis. Health Technol Assess 10:1–168
Zhang Y, Begum HA, Grewal H, Etxeandia-Ikobaltzeta I, Morgano GP, Khatib R et al (2022) Cost-effectiveness of diagnostic strategies for venous thromboembolism: a systematic review. Blood Adv 25:544–567
Furlan A, Aghayev A, Chang C-CH, Patil A, Jeon KN, Park B et al (2012) Short-term mortality in acute pulmonary embolism: clot burden and signs of right heart dysfunction at CT pulmonary angiography. Radiology. 265:283–293
Zhao L, Prior SJ, Kampmann M, Sorkin JD, Caldwell K, Braganza M et al (2014) Measurement of thrombus resolution using three-dimensional ultrasound assessment of deep vein thrombosis volume. J Vasc Surg Venous Lymphat Disord 2:140–147
Acknowledgements
The authors would like to thank Fuka Oikawa for her valuable assistance with the editing of this manuscript.
Funding
This research was carried out without funding.
Author information
Authors and Affiliations
Contributions
Conception: MA; Design of the work: MA, HK, HS, KS; the acquisition, analysis: MA, YK, IW, TK; interpretation of data: MA, YK, IW, TK; Writing – original draft: MA. Writing – revised: HK, HS, KS, NM, YS. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of author’s hospital. (permit No. 171).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Akagawa, M., Kijima, H., Kimura, Y. et al. Fibrin monomer complex on postoperative day 1 is correlated with the volume of deep vein thrombosis after knee surgery. J EXP ORTOP 9, 47 (2022). https://doi.org/10.1186/s40634-022-00482-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-022-00482-y