
Abstract
Background
Pancreatic ductal adenocarcinoma (PDAC) readily metastasizes to the lymph nodes, liver, lung, and peritoneum; however, gastric and gallbladder metastases are rare. We report a case of metachronous gastric and gallbladder metastases from PDAC.
Case presentation
The patient is a 71-year-old man who underwent distal pancreatectomy for PDAC. Seventeen months after the surgery, a 30-mm nodule was detected at the lesser curvature of the stomach, which was diagnosed as recurrence of PDAC in the lymph nodes. He then received gemcitabine and S-1 combination chemotherapy for 6 months. Because tumor size remained approximately the same and tumor marker levels decreased, total gastrectomy and cholecystectomy were performed. Pathological examination showed well-differentiated tubular adenocarcinoma in the subserosa and muscularis propria of the stomach and gallbladder. The patient remains alive at 41 months after the second surgery with liver metastasis.
Conclusion
We reported a rare case of metachronous gastric and gallbladder metastases from pancreatic body cancer.
Similar content being viewed by others

Background
Prognosis in patients with pancreatic ductal adenocarcinoma (PDAC) remains dismal, with a 5-year survival rate below 10% [1, 2]. The lymph nodes, liver, lung, and peritoneum are the predominant sites of metastasis; however, gastric and gallbladder metastases are very rare. We describe a case of metachronous gastric and gallbladder metastases from pancreatic body cancer.
Case presentation
A 71-year-old man with a history of atrial fibrillation, acute appendicitis, and early esophageal cancer treated with endoscopic submucosal dissection underwent distal pancreatectomy with splenectomy for treatment of pancreatic body cancer (Fig. 1a). Pathological examination showed well-differentiated tubular adenocarcinoma (pT3, pN0, pM0). The Union for International Cancer Control (UICC) stage was established as IIa (Fig. 1b). After surgery, the patient received adjuvant chemotherapy of S-1 for 6 months. Multi-detector row computed tomography (MDCT) showed a 30-mm nodule at the lesser curvature of the stomach 17 months after pancreatectomy during postoperative surveillance (Fig. 2a). Positron emission tomography (PET)/CT showed fluorodeoxyglucose (FDG) uptake in the nodule; maximum standardized uptake value uptake (SUVmax) was 3.5 (Fig. 2b). Upper gastrointestinal endoscopy revealed mucosal irregularity in the posterior wall of the lesser curvature of the gastric body (Fig. 2c) and submucosal tumor in the anterior wall of the stomach antrum (Fig. 2d). Endoscopic ultrasound (EUS) showed the hypoechoic submucosal tumor, which was diagnosed as adenocarcinoma by fine-needle aspiration (FNA) cytology.

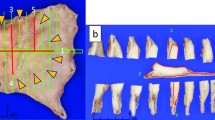
Primary operation for pancreatic body cancer. a Multi-detector row computed tomography (MDCT) showed pancreatic body cancer before the first surgery (arrows). b Pathological findings of the primary tumor were as follows: invasive ductal carcinoma, well-differentiated type, and (T3, N0, M0) stage IIa

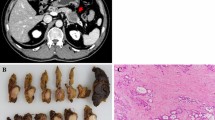
Imaging diagnosis of recurrence. a MDCT showed a 30-mm nodule at the lesser curvature of the stomach. b Positron emission tomography (PET)/CT showed fluorodeoxyglucose (FDG) uptake in the nodule; SUVmax was 3.5. c Upper gastrointestinal endoscopy revealed mucosal irregularity in the posterior wall of the lesser curvature of the gastric body (arrow). d Upper gastrointestinal endoscopy revealed submucosal tumor in the anterior wall of the gastric antrum (arrowhead)
Based on these findings, we diagnosed lymph node metastasis of PDAC invading the gastric wall, and the patient was treated with gemcitabine and S-1 combination (GS) therapy for 6 months. Considering the patient’s age and prior pancreatic resection, we selected GS therapy due to its relatively high response rate and manageable complication rate found in a previous phase III study for unresectable pancreatic cancer (GEST study) [3]. Because the tumor size did not change over 6 months and CA 19-9 decreased from 54 to 28 U/mL, we decided to perform total gastrectomy and prophylactic cholecystectomy for tumor resection.
Macroscopically, two nodules were located in the stomach, with one in the wall of the lesser curvature and the other in the antrum anterior wall (Fig. 3a). Pathological examination showed that these were well-differentiated tubular adenocarcinomas in the subserosa and muscularis propria of the stomach. The tumor was not exposed to the mucosa and serosa, and there was no lymph node involvement (Fig. 3b).

Histological findings of metastases. a Macroscopic findings in the stomach. There were two lesions in the stomach wall (arrow: lesser curvature (25 × 20 mm), arrowhead: anterior wall of antrum (15 × 13 mm). b Pathological examination showed well-differentiated tubular adenocarcinoma in the subserosa and muscularis propria of the stomach; the tumor was not exposed to the mucosa and serosa (arrow), and there was no involvement of lymph nodes. c Macroscopic finding in the gallbladder. A 13 × 5-mm submucosal tumor was found in the neck of the gallbladder (arrow). d Well-differentiated tubular adenocarcinoma located in the subserosa of the gallbladder (arrow)
Surprisingly, there was a tumor in the neck of gallbladder; pathological examination revealed this was a well-differentiated tubular adenocarcinoma in the subserosa (Fig. 3c, d).
As the pathological findings of these tumors were similar to the lesion initially resected by distal pancreatectomy, we diagnosed metachronous gastric and gallbladder metastases from PDAC.
The patient’s postoperative course was uneventful, and the patient was discharged on postoperative day 16. Because of prior S-1 adjuvant therapy after pancreatectomy and GS therapy before gastrectomy/cholecystectomy, we elected to defer further chemotherapy. A liver metastasis was discovered 7 months after the second operation. He was then treated with GS therapy followed by gemcitabine and albumin-bound paclitaxel combination therapy and modified FOLFIRINOX therapy. At 41 months after the second surgery, the patient remained alive.
Discussion
Previous studies have noted that the predominant sites of metastasis for PDAC are the lymph node, liver, lung, and peritoneum [4, 5]. We described a rare case of metachronous gastric and gallbladder metastases from pancreatic body cancer. Gastric metastasis of PDAC is rare. To our knowledge, only three cases have been reported in the English literature [6,7,8]. Oda et al. performed autopsies on 209 patients with PDAC and reported that gastric metastasis was found in only two cases [9].
Generally speaking, there are five metastatic pathways to the stomach: (1) direct invasion, (2) intraoperative seeding, (3) hematogenous metastasis, (4) lymphatic metastasis, and (5) intraluminal or intramural dissemination [10]. In our case, the primary pancreatic tumor was not anatomically near the stomach, and resection with tumor-free margins was performed. In addition, the two metastatic lesions in the subserosa and muscularis propria of the stomach did not expose to the mucosa or serosa. Considering these facts, we thought that gastric metastasis occurred through the hematogenous pathway.
Gallbladder metastasis of PDAC is also rare. This appears to be the first report of resected gallbladder metastasis from PDAC in the English literature. An autopsy study by Kishi et al. demonstrated a 7.4% incidence of gallbladder metastasis among patients with PDAC [11]. Yoon et al. surveyed 417 patients with pathologically confirmed gallbladder malignancies; 20 (4.8%) were metastatic (stomach, n = 8; colorectum, n = 3; liver, kidney, and skin, n = 2 each; and others, n = 3) [12]. In our case, as the tumor was subserosal and did not expose to the mucosa, hematogeneous metastasis was most likely, as with the gastric metastases. Although Yoon et al. also reported that the prognosis of metastatic gallbladder carcinoma was poor, with 8.7 months of median overall survival [12], our case resulted in long-term survival after surgical resection.
There was a possibility that cancer cell seeding by FNA was the cause of gastric metastases. However, we think it unlikely because one of the metastases was located in the antrum, far from the aspiration site, and we also found a gallbladder metastasis which could not have been related to FNA.
Surgical resection for disease relapse of PDAC remains debatable due to lack of evidence of survival benefit. Recently, several studies showed survival benefit of surgical resection for PDAC recurrence. Miyazaki et al. showed a prolonged survival by repeat pancreatomy for isolated local recurrence [13]. Thomas et al. highlighted a single tumor as a key factor benefiting most from re-resection for lung metastasis from PDAC [14].
In the case presented here, we first diagnosed solitary lymph node recurrence of PDAC after pancreatectomy by CT imaging and performed surgical resection after chemotherapy. Unintentionally, two gastric metastases and one gallbladder metastasis were resected with tumor-free margins. This patient’s survival of more than 3 years suggests the benefit of surgical intervention in combination with systemic chemotherapy. However, specific selection criteria for resection for multiple metastases remain unclear.
Conclusions
We reported a case of surgically resected metachronous gastric and gallbladder metastases from pancreatic body cancer. Further studies of surgical resection of PDAC recurrence are needed.
References
Li D, Xie K, Wolff R, Abbruzzese JL. Pancreatic cancer. Lancet. 2004;363(9414):1049–57.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30.
Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clini Oncol. 2013;31(13):1640–8.
Blastik M, Plavecz E, Zalatnai A. Pancreatic carcinomas in a 60-year, institute-based autopsy material with special emphasis of metastatic pattern. Pancreas. 2011;40(3):478–80.
Peixoto RD, Speers C, McGahan CE, Renouf DJ, Schaeffer DF, Kennecke HF. Prognostic factors and sites of metastasis in unresectable locally advanced pancreatic cancer. Cancer Med. 2015;4(8):1171–7.
Takamori H, Kanemitsu K, Tsuji T, Kusano S, Chikamoto A, Okuma T, et al. Metastatic gastric tumor secondary to pancreatic adenocarcinoma. J Gastroenterol. 2005;40(2):209–12.
Sasajima J, Okamoto K, Taniguchi M. Hematogenous gastric metastasis of pancreatic cancer. Case Rep Gastroenterol. 2016;10(1):75–80.
Umezaki N, Hashimoto D, Nakagawa S, Yamao T, Tsukamoto M, Kitano Y, et al. Cystic gastric metastasis from pancreatic cancer. Surg Case Rep. 2018;4(1):31.
Oda KH, Yamao T, Saito D, Ono H, Gotoda T, et al. Metastatic tumors to the stomach: analysis of 54 patients diagnosed at endoscopy and 347 autopsy cases. Endoscopy. 2001;33(6):507–10.
Feczko PJ, Collins DD, Mezwa DG. Metastatic disease involving the gastrointestinal tract. Radiol Clin N Am. 1993;31(6):1359–73.
Kishi KHT, Nakamura K, Yoshimori M, Ohkura H, Ozaki H. Carcinoma of the pancreas: a review of 94 autopsy cases. Jpn J Clin Oncol. 1980;10(2):273–9.
Yoon WJ, Yoon YB, Kim YJ, Ryu JK, Kim YT. Metastasis to the gallbladder: a single-center experience of 20 cases in South Korea. World J Gastroenterol. 2009;15(38):4806–9.
Miyazaki M, Yoshitomi H, Shimizu H, Ohtsuka M, Yoshidome H, Furukawa K, et al. Repeat pancreatectomy for pancreatic ductal cancer recurrence in the remnant pancreas after initial pancreatectomy: is it worthwhile? Surgery. 2014;155(1):58–66.
Thomas RM, Truty MJ, Nogueras-Gonzalez GM, Fleming JB, Vauthey JN, Pisters PW, et al. Selective reoperation for locally recurrent or metastatic pancreatic ductal adenocarcinoma following primary pancreatic resection. J Gastrointest Surg. 2012;16(9):1696–704.
Acknowledgements
Not applicable.
Funding
None
Availability of data and materials
Data sharing is applicable to this article.
Author information
Authors and Affiliations
Contributions
MT drafted the manuscript. HY, AK, KF, TT, SK, ST, MM, and MO contributed in the preoperative check and diagnosis. HY, SK, MT, and KK performed the operation. HY and ST followed up the patient. KS diagnosed the disease as pathologists. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Informed consent was obtained from the patient for the publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Takahashi, M., Yoshitomi, H., Kato, A. et al. A case of successfully resected metachronous gastric and gallbladder metastases from pancreatic body cancer. surg case rep 5, 21 (2019). https://doi.org/10.1186/s40792-019-0581-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-019-0581-1