
Abstract
Background
Low-income countries bear a growing and disproportionate burden of oral diseases. With the World Health Organization targeting universal oral health coverage by 2030, assessing the state of oral health coverage in these resource-limited nations becomes crucial. This research seeks to examine the political and resource commitments to oral health, along with the utilization rate of oral health services, across 27 low-income countries.
Methods
We investigated five aspects of oral health coverage in low-income countries, including the integration of oral health in national health policies, covered oral health services, utilization rates, expenditures, and the number of oral health professionals. A comprehensive search was conducted across seven bibliographic databases, three grey literature databases, and national governments’ and international organizations’ websites up to May 2023, with no linguistic restrictions. Countries were categorized into “full integration”, “partial integration”, or “no integration” based on the presence of dedicated oral health policies and the frequency of oral health mentions. Covered oral health services, utilization rates, expenditure trends, and the density of oral health professionals were analyzed using evidence from reviews and data from World Health Organization databases.
Results
A total of 4242 peer-reviewed and 3345 grey literature texts were screened, yielding 12 and 84 files respectively to be included in the final review. Nine countries belong to “full integration” and thirteen countries belong to “partial integration”, while five countries belong to “no integration”. Twelve countries collectively covered 26 types of oral health care services, with tooth extraction being the most prevalent service. Preventive and public health-based oral health interventions were scarce. Utilization rates remained low, with the primary motivation for seeking care being dental pain relief. Expenditures on oral health were minimal, predominantly relying on domestic private sources. On average, the 27 low-income countries had 0.51 dentists per 10,000 population, contrasting with 2.83 and 7.62 in middle-income and high-income countries.
Conclusions
Oral health care received little political and resource commitment toward achieving universal health coverage in low-income countries. Urgent action is needed to mobilize financial and human resources, and integrate preventive and public health-based interventions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Oral diseases, such as dental caries, periodontal disease, and oral cancer, stand out as the most prevalent health conditions, posing a major global public health challenge [1]. It was estimated that approximately 3.5 billion people suffered from oral diseases worldwide [2]. Oral diseases could lead to pain, swelling, mastication difficulties, and susceptibility to other medical conditions such as atherosclerosis, cardiovascular disease, diabetes, and malnutrition [3,4,5,6]. Oral diseases can also affect self-esteem, reduce social interaction, and even result in stigmatization [7]. Moreover, they are closely linked to substantial productivity loss and lower educational attainments. Evidence indicates that the global productivity loss due to oral diseases reached an estimated US$ 323 billion in 2019 [7]; additionally, children with poor oral health are 52% more likely to exhibit poor academic performance and 43% more likely to experience school absenteeism [8].
Resources for oral health care and the burden of oral diseases are unevenly distributed across regions, countries, and socioeconomic groups [7]. In 2019, 88% of the direct costs of oral health care were spent for only 22.5% of the world’s population, mainly residing in high-income countries [7]. Meanwhile, more than three-quarters of those with oral conditions lived in low- and middle-income countries (LMICs) [7]. In Rwanda, for example, 54.3% of its population had untreated dental caries according to its first National Oral Health Survey [9]. Due to high out-of-pocket spending, disadvantaged households paying for necessary oral health care are more likely to experience catastrophic health expenditures and face impoverishment than their better-off counterparts [10, 11]. In addition, countries with public dental care coverage have lower socioeconomic inequalities in dental care utilization than those without such programs [12].
To tackle these challenges, the global community has launched a series of initiatives for oral health. In 2021, the World Health Assembly (WHA) adopted a resolution urging the integration of oral health into national policies and universal health coverage (UHC) [13]. This resolution was followed by the release of the Global Strategy on Oral Health during the 2022 WHA, which envisions achieving UHC for oral health for all individuals and communities by 2030 [14]. As a critical step towards implementing this strategy, the World Health Organization (WHO) released the Global Oral Health Action Plan (2023–2030), providing guidance for member states to operationalize objectives at the national and sub-national levels [15]. On December 15, 2023, the WHO added Noma (Cancrum Oris) to its list of neglected tropical diseases, marking a significant step toward prioritizing political and resource commitments for this severe and potentially fatal oral disease [16].
In addition to these initiatives, a notable effort is the WHO Global Oral Health Status Report [7]. This report reviews the status of oral disease burden, oral health policies, and resource investments over countries. While groundbreaking, the report and its country profiles only provide a summary of the existence of national oral health policies using a binary “yes-or-no” question without providing further details, such as the covered oral health services in their national policies. In addition, the report does not examine oral health service utilization rates or analyze oral health expenditures over the years. To address these gaps, especially for low-income countries, we conducted a scoping review to examine universal oral health coverage in low-income countries through five key questions: (1) the integration of oral health in national health policies; (2) the inclusion of clinical and public oral health care services in government-defined essential health service lists; (3) oral health care utilization rates; (4) oral health care expenditures; and (5) the number of oral health care professionals.
Methods
Search strategy
We conducted a scoping review to examine the universal coverage for oral health care in low-income countries. We followed the World Bank 2020 income classification [17] in identifying the 27 low-income countries (countries with gross national income [GNI] per capita of 1,045 US dollars or less) as listed in Table 1. We looked for evidence from peer-reviewed publications, grey literature, websites of national governments and international organizations, and WHO databases. We reported this scoping review in accordance with the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [18]. We registered the protocol of this scoping review a priori in Open Science Framework (https://osf.io/5pbhm/).
For peer-reviewed publications, we systematically searched seven bibliographic electronic databases: PubMed, Embase (Elsevier), Web of Science (Clarivate), EconLit (EBSCO), Global Health (EBSCO), WHO Global Index Medicus, and Dentistry and Oral Sciences Source. Two librarian coauthors (JC and MB) developed keyword search strings and adapted them for different databases. Table 2 shows the search string for PubMed. Search strings for other bibliographic databases are presented in Web Appendix 1. As shown in Table 2, the string consists of three groups of keywords: keywords and MeSH terms representing “oral”, “dental”, and “teeth”; keywords representing health care or the three UHC dimensions, such as “care”, “health”, “service”, “finance”, “coverage”, “spending”, “utilization”; and keywords and MeSH terms referring to the 27 low-income countries. We searched for the presence of keywords in titles and abstracts of publications. The search covered the period from January 2010 to May 2023 to capture the recent data.
We conducted a comprehensive search for grey literature from four sources. First, we searched the WHO Country Planning Cycle Database [19], WHO Non-communicable Diseases Document Repository [20], and WHO MiNDbank database [21] to identify countries’ most recent National Health Policies, Strategies, and Plans (NHPSPs), National Health Service Packages, National Non-communicable Disease Strategic Plans, and National Oral Health Strategic Plans. A NHPSP outlines a country’s political and resource commitment to ensuring the health of its population [22], while a National Health Service Package specifies government-defined essential public and clinical health services to be delivered at different health care levels [23]. By examining National Non-communicable Disease Strategic Plans, we assessed the extent to which countries align with WHO’s recommendations on recognizing and addressing oral health issues through the lens of common risk factors shared with other non-communicable diseases. Additionally, through searching National Oral Health Strategic Plans, we provided baseline information on the progress toward the international commitment of having operational national oral health policies by 2030 [15].
Second, we conducted searches to identify oral health content in national health policies beyond the four policy types mentioned above. This was done by using the WHO publication database [24] and the Google search engine with predefined strings. The Google search was applied to the websites of national health departments and WHO country profiles [25] (see details for the Google search in Web Appendix 2). Third, we searched three grey literature databases, including the PAIS Index, OECD iLibrary, and World Bank eLibrary (see details in Web Appendix 3). Both Google and grey literature database searches covered the period from January 2010 to May 2023. Fourth, we examined the websites and reports of major non-governmental organizations and foundations that provide international oral health care services, such as Global Dental Relief [26], Smiles for Everyone Foundation [27], and Global Child Dental Fund [28]. We utilized a snowball strategy to scrutinize the reference lists of searched peer-reviewed and grey literature.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) the setting in one or multiple of the 27 low-income countries; (2) containing any information related to the integration of oral health in national health policies, the inclusion of clinical and public oral health care services in government-defined essential health service lists, oral health care utilization rates, oral health care expenditures, and the number of oral health care professionals, and (3) full-text availability. We did not impose any language restrictions, using Google Translate for publications or literature not originally written in English. To provide policy makers with the most recent information, we replaced outdated policies of countries with their most recent versions, if available. We excluded clinical trial studies.
Literature review and evidence extraction
For peer-reviewed publications, titles and abstracts of searched studies were imported into reference management tools (EndNote and Zotero). Duplicates were removed. All remaining titles and abstracts were uploaded to the Covidence platform (https://www.covidence.org/), where three coauthors independently screened and selected studies for full-text review. The selected full-text studies were subsequently retrieved and assigned to two groups of coauthors for data extraction, with each group consisting of two members. To ensure accuracy, the two coauthors of each group independently reviewed the same studies and cross-checked each other’s work. For grey literature, as most of it does not have a structured abstract, we were not able to remove duplicates with reference management tools. Therefore, we assigned the full text of all the searched grey literature to four groups of coauthors, with each group consisting of two members, to conduct a literature review and data extraction in duplicate.
We used a pilot-tested template in the form of Excel spreadsheets to record the extracted information. This template included fields for “title”, “author(s)”, “publication year”, “study location”, “study design”, “study aim”, “data source”, “data collected year”, and “main findings”. Discrepancies between group members on review and data extraction were discussed and addressed at team meetings. Additional details on data extraction can be found in Web Appendix 4.
Evidence synthesis and analysis
We started with assessing a country’s integration of oral health into national health policies. We categorized the 27 low-income countries into three groups: first, “full integration”, defined as countries that have developed national oral health policies, thereby fulfilling target 1.1 of the WHO Global Oral Health Action Plan (2023–2030) related to establishing operational national oral health policies [15]; second, “partial integration”, defined as countries that lack such specific policies but aggregately mention oral health keywords at least five times across other national health policies; and third, “no integration”, defined as countries that lack national oral health policies and aggregately mention oral health keywords less than five times across other national health policies. In order to identify countries as “partial integration” and “no integration”, we followed previous studies [29, 30] and created a list of oral health keywords through a review of significant literature on oral health. We conducted searches for each keyword and counted the frequency of their appearance in each included national health policy document. We only counted when a keyword appeared in the context of oral health. For example, the keyword “abscess” will be counted if it pertains to dental abscesses but will not be counted if it refers to abscesses within other tissues of the body (see keywords in Web Appendix 5). The threshold of at least five mentions was established as a significant number in previous studies that assessed the policy inclusion of surgery [29, 30]. Since countries’ NHPSPs and National Non-communicable Disease Strategic Plans are the main policies demonstrating countries’ political commitments to health, we also offered a more detailed summary of oral health content within these two policy types, which is presented in the Appendix.
In terms of assessing oral health services included in countries’ essential service packages, we focused on the national health policies that include a list of government-defined essential clinical and public health services, such as National Health Service Packages, and summarized the covered oral health care services. This analysis aimed to provide insights into the extent to which oral health has received practical priority within essential healthcare coverages outlined in national policies.
To assess oral health care utilization rates, we narratively summarized utilization rates found in both peer-reviewed publications and grey literature. Additionally, we summarized the primary reasons for seeking oral health care services and the most frequently administered interventions. We also summarized the determinants and inequalities of oral health care utilizations.
We used two international data sources to assess oral health expenditures: (1) the WHO Global Oral Health Status country profiles [31], which documented per capita expenditures on outpatient dental care in 2019, aggregated from both public and private sources, and (2) the WHO Global Health Expenditure Database [32], which recorded dental outpatient expenditures per capita financed by domestic public, private, and external sources between 2016 and 2020. We downloaded data from these two sources in May 2023. We identified thirteen low-income countries with available data from both data sources and compared their recorded values.
To assess the workforce, we obtained data on the number of dentists, dental prosthetic technicians, dental assistants and dental therapists per 10,000 population from the WHO National Health Workforce Account [33]. We downloaded data for the years spanning from 2010 and 2021. Countries varied in terms of years with available data. Using countries’ most recent data, we calculated the average densities of dentists, dental prosthetic technicians, dental assistants and dental therapists in low-income countries and compared them with those in middle-income and high-income countries. We downloaded the workforce data in July 2023.
Web Appendix 6 presents a summary of the information sources used to gather evidence for analyzing each of the five research questions.
Results
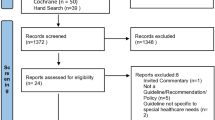
As shown in the PRISMA flowchart (Fig. 1), our systematic search of the seven electronic bibliographic databases yielded a total of 4242 studies. After removing duplicates, studies published before 2010, and those deemed irrelevant based on title and abstract screening, a full-text review for eligibility was given to 65 studies. From this full-text review, we identified twelve peer-reviewed papers that met our inclusion criteria. For grey literature, we obtained 3345 records from multiple sources. After a full-text review of each literature, we excluded 3241 records that did not meet the inclusion criteria, as well as 20 outdated policies that had been replaced by their more recent versions. Consequently, we included 84 pieces of grey literature. Together with the peer-reviewed studies, our scoping review ultimately included 96 articles.

PRISMA flowchart
Characteristics of the 96 included articles
Figure 2 illustrates the distribution of the 96 included articles across countries. Notably, Rwanda stands out with the highest number of included articles at ten, followed closely by Afghanistan and Ethiopia at six. The remaining countries generally have articles ranging from one to five. We included one peer-reviewed article and one grey literature (the WHO Global Oral Health Status Report) that examined oral health resources in multiple low-income countries.

Distribution of the 96 included articles across countries
For the twelve peer-reviewed papers, Table 3 demonstrates that nine out of them are questionnaire- and screening-based research that provided information on oral health care utilization, while three discussed the current stock or the development of oral health professionals. Out of the 84 pieces of grey literature, 28 consist of the WHO Global Oral Health Status Report and its associated country profiles, while the remaining 56 comprise the most recent national health policies with oral health care information. Figure 3 illustrates that the 56 national health policies belong to nine policy types, with NHPSPs being the most frequent type, followed by the National Non-communicable Disease Strategic Plan, National Health Service Package, National Oral Health Strategic Plan, and other national health policies. Appendix 7 summarizes oral health information for each of the 56 national health policies.

Distribution of the 56 included policy documents over policy types. *RMNCH: Reproductive, Maternal, Newborn and Child Health
Integration of oral health in national health policies
We identified nine countries as “full integration” as they have established their national oral health policies, including Burkina Faso [34,35,36], Congo DR [37], Guinea-Bissau [38], Madagascar [39,40,41,42], Mali [43, 44], Mozambique [45,46,47], Niger [48, 49], Rwanda [50,51,52,53,54,55,56], and Uganda [57, 58]; thirteen countries as “partial integration” as they do not have such specific policies but mention oral health keywords more than five times across their other national health policies, including Afghanistan [59,60,61,62,63], Burundi [64,65,66], the Central African Republic [67, 68], Chad [69], Eritrea [70, 71], Ethiopia [72,73,74], Gambia [75,76,77], Guinea [78], Liberia [79], Malawi [80], Sierra Leone [81, 82], Somalia [83], and Togo [84, 85]; five countries as “no integration” as they do not have national oral health policies and mention oral health keywords less than five times across their other national health policies, including North Korea [86], South Sudan [87], Sudan [88], Yemen [89], and the Syrian Arab Republic. For the Syrian Arab Republic, we identified its WHO oral health country profile but did not locate any national health policies with oral health content. Our detailed analyses of the integration of oral health in NHPSPs (Appendix 8) and National Non-communicable Disease Strategic Plans (Appendix 9) show that oral health is largely overlooked in these two overarching policy types in low-income countries.
Oral health care services included in government-defined essential health service lists
We identified thirteen countries with lists of government-defined essential clinical and public health care services. Except Burundi, all the other twelve countries mentioned the coverage of oral health care services, resulting in a collective offering of 26 different types of oral health care services (Table 4). By country, Rwanda distinguished itself by offering the most extensive array of oral services to its population (12 types) [52,53,54]. It is followed by Ethiopia (11 types) [73], Sierra Leone (8 types) [81], Liberia (5 types) [79], Madagascar and Mozambique (4 types, respectively) [40, 45], Afghanistan, Malawi, and Somalia (3 types, respectively) [59, 80, 83], Eritrea (2 types) [71], as well as Gambia and Sudan (1 type, respectively) [76, 88].
Tooth extraction emerged as the predominant intervention, appearing in the health service lists of seven countries [40, 52, 73, 79,80,81, 83]. Four countries covered dental abscess drainage [52, 73, 79, 83], making this procedure the second most frequently provided intervention. In contrast, as preventive measures, services on oral health knowledge awareness [45, 73, 81], dental scaling [54], fluoride use expansion [45], and oral disease screening [53] were only covered by a small number of countries. Of particular concern, only Sierra Leone explicitly covered Atraumatic Restorative Treatment (also called Alternative Restorative Treatment) (ART) [81]. As ART has been recommended by the WHO as a cost-effective approach to address dental caries in resource-limited settings [23, 90], its rare coverage indicates a consistently insufficient supply in low-income countries. Additionally, information was limited regarding what segment of the population was covered by essential oral health care services. We identified only four countries with explicit information on the age characteristics of the covered population, including Liberia [79], Mozambique [45], and Eritrea [71], covering oral health care services for school-age children; only Eritrea and Ethiopia, however, explicitly covered oral health care services for the elderly and the detection of cleft lip and palate for newborns, respectively [71, 73].
Information was scarce regarding the cost-sharing structure of oral health care services. Among the countries that included coverage of oral health care services, only Ethiopia explicitly outlined a cost-sharing arrangement. In Ethiopia, the detection of cleft lip and palate in newborns, along with the promotion of awareness regarding proper oral hygiene practices, is provided at no cost. However, other oral health care services, such as tooth extraction, involve a cost-sharing mechanism [73]. Unfortunately, detailed information on the specifics of the cost-sharing mechanism is lacking.
Utilization rates of oral health care service
We identified seven countries with available information on the utilization rates of oral health care services. Among countries with nationally sampled populations, the individual rate was 2.0% in Mozambique among its general population (past 12 months usage) [46], 2.1% in Burkina Faso among adults (past 6 months usage) [91], 13.4% in Sudan among adults (past 12 months usage) [92], and 29.4% in Rwanda among its general population (ever usage) [9]; Sierra Leone witnessed various utilization rates of ever usage for school children at different ages, ranging from 3.0% for the 6-years-old, 34.0% for the 12-years-old, to 27.0% for the 15-years-old [93]. On the other hand, for populations sampled at the subnational or institutional level, the estimated rates ranged from 7.4% in Ethiopia’s Areka town among school children (past 12 months usage) [94], 10.6% in Ethiopia’s Mekelle city among school children (past 12 months usage) [95], 9.0% in Sudan’s Khartoum State among aged 16 and above for regular checkups and 37% among the elderly attending primary healthcare centers (past 12 months usage) [96, 97], to 52.0% in Uganda’s Nebbi District among adults (past 12 months usage) [98].
In terms of reasons for seeking oral health care services, a significant proportion of the surveyed population reported dental pain, such as 66.9% in Sudan and 98.7% in Rwanda [9, 92], or reported that they would only seek care when facing oral health conditions (e.g., school children in Sierra Leone) [93]. In the realm of treatments, tooth extraction was the most frequently administered intervention for alleviating dental pain, rather than other restorative dental care procedures. Concretely, among the individuals who sought oral health care services, 73.7% of those in Uganda’s Nebbi District had tooth extraction as their sole treatment [98], while the percentage was 55.0% in Sudan’s Khartoum State [97], and 52.0% in Mozambique [46]. In Ethiopia’s Areka town, 41.4% of those who have visited dental clinics went for emergency dental pain treatment and 8.6% for tooth extraction [94]. See details in Table 3 and Web Appendix 7.
We identified three peer-reviewed papers with information on the determinants and inequalities of dental service utilization. Among the socioeconomic determinants, adults residing in urban areas, those from wealthier households, or school children born to mothers with higher educational attainment are consistently more likely to use dental care services compared to those living in rural areas, from less wealthy households, or children born to mothers with lower education levels [91, 92, 95].
Oral health care expenditures
Oral healthcare expenditures in low-income countries are low. Based on WHO’s Global Oral Health Status country profiles [31], only North Korea, the Syrian Arab Republic, and Sudan allocated more than one US dollar per capita in 2019 on dental outpatient care, while all the other countries spent an amount ranging from zero to 0.5 US dollars per capita (Fig. 4). On the other hand, according to the WHO Global Health Expenditure Database [32], fourteen countries spent an average of 0.19 US dollars per capita for dental outpatient care for the most recent year of available data. Among these fourteen countries, nine predominantly relied on the domestic private sector to bear expenditures, with only Afghanistan, Gambia, and South Sudan financing more than half of their expenditures from domestic government sources (Fig. 5).

Per capita expenditures on dental outpatient care in 2019 based on Global Oral Health Status Report. Note: Currency in US dollar

Most recent per capita expenditures on dental outpatient care based on Global Health Expenditure Database. Note: Currency in 2020 US dollar
When considering time trends, only five countries—Afghanistan, Burkina Faso, Gambia, Niger, and South Sudan—exhibited an upward trend in government expenditures from 2016 to 2020, while Sierra Leone, Sudan, and Uganda reduced their government funds during the same period. Out of the eight countries that received external funds, four experienced a decline in annual receipts. These countries are Afghanistan, Guinea, Sierra Leone, and South Sudan. Interestingly, these reductions did not lead to significant decreases in the overall expenditures on dental outpatient care in Afghanistan and South Sudan, attributed to the increased financial support from their respective domestic governments (Web Appendix 10).
Furthermore, we observed significant discrepancies in the recorded per capita expenditures on dental outpatient care in 2019 between the two data sources. These disparities are particularly notable for countries such as Afghanistan, Chad, Sierra Leone, South Sudan, and Sudan. Although the WHO Global Health Expenditure Database includes expenditures financed by external sources as an additional component, the magnitude of such expenditures is much smaller compared to the disparities. For instance, in 2019, the disparity for Serra Leone was 1.11 US dollars per capita, whereas the external expenditure was only 0.01 US dollars per capita (Web Appendix 11).
Number of oral health professionals
Our literature review identified three papers highlighting a significant shortage of oral health professionals in low-income countries [99,100,101]. For the WHO National Health Workforce Account [33], from 2010 to 2021, twenty-six low-income countries reported workforce data on dentists, while only twelve countries reported data on dental prosthetic technicians, and sixteen countries reported data on dental assistants and dental therapists. Somalia is the only country that did not report any oral health workforce data.
On average, the most recent dentist density is remarkably low, standing at 0.51 per 10,000 population across low-income countries (Fig. 6). This number is less than one-fifth of the density in middle-income countries (2.83) and represents a mere one-fifteenth of the density in high-income countries (7.62) [33]. By individual country, only five low-income countries exceeded the average line of 0.51. These countries are the Syrian Arab Republic (6.61), North Korea (2.19), Sudan (2.13), Afghanistan (0.71), and Eritrea (0.54). The remaining countries exhibited considerably low dentist densities, ranging from 0.01 to 0.21 dentists per 10,000 population.

Most recent number of dentists per 10,000 population in 27 low-income countries. (Data source: WHO National Health Workforce Accounts Data Portal)
We also observed that some countries relied on other types of professionals, encompassing dental prosthetic technicians, dental assistants, and dental therapists, rather than predominantly on dentists to deliver oral health care services. For example, Sierra Leone’s workforce is primarily composed of dental prosthetic technicians. In countries such as Uganda, Malawi, Guinea-Bissau, Gambia, Burkina Faso, Mali, Togo, and Liberia, there is a higher prevalence of dental assistants and dental therapists compared to dentists (Fig. 7). However, the average density of other dental professionals in low-income countries remained remarkably low, with only 0.07 dental prosthetic technicians and 0.08 dental assistants and dental therapists per 10,000 population, compared to 0.46 and 0.83 in middle-income countries and 2.11 and 5.88 in high-income countries.

Most recent number of dentists, dental prosthetic technicians, and dental assistants and therapists per 10,000 population in 27 low-income countries. (Data source: WHO National Health Workforce Accounts Data Portal)
We grouped findings of the five study aspects by country in Web Appendix 12. For oral health expenditures, we summarized countries’ most recent data on per capita expenditures on oral outpatient care in Web Appendix 12.
Discussion
Given the rising prevalence of oral diseases worldwide and the recent international commitment to achieving universal coverage for oral health by 2030, our study offers timely information on the universal coverage states for oral health in 27 low-income countries. Overall, we identified that there are limited sources of information on oral health in low-income countries, highlighting an urgent need to intensify efforts in progress monitoring and strengthening oral health care systems.
The extent of integrating oral health in national health policies varies across the 27 low-income countries. Notably, only nine countries have developed national oral health policies; thirteen countries lack such specific policies but have significantly incorporated oral health within their other national health policies. However, as a particular concern, five countries lack both national oral health policies and an adequate mention of oral health within their other national health policies, indicating neglect of political commitment to oral health in these nations. Furthermore, our study revealed that only five low-income countries (Afghanistan, Burkina Faso, Eritrea, Gambia, and Madagascar) have explicitly included oral health in national health policies designed for maternal, children, and elderly health [35, 42, 62, 71, 75]. This small number reflects that the concept of treating oral disease as a progressive condition throughout the life course received little attention from policy makers in low-income countries.
In addition, we identified a large deficiency in oral health service provision in low-income countries. According to WHO, the African region faces a substantial disease burden from seven oral diseases, including dental caries, periodontal diseases, oral cancers, noma, oral manifestation of HIV and AIDS, orofacial trauma, and cleft lip and palate [23]. Accordingly, the WHO recommended the inclusion of three key interventions—oral urgent treatment, affordable fluoride toothpaste, and atraumatic restorative treatment—in the basic package of oral care for resource-limited settings [90]. However, we found that only four low-income countries explicitly included some of these three key interventions in their government-defined essential health care service lists, and no low-income countries listed noma and the management of the oral manifestation of HIV and AIDS. In contrast, we observed a skewed prioritization toward invasive clinic procedures, such as tooth extraction and dental abscess drainage, rather than preventive interventions delivered in a public health approach, for example, the usage of affordable fluoride toothpaste. This finding reconfirmed the deep-seated Westernized model of dentistry in low-income countries, which relied on a clinical interventionist philosophy but oversight addressing oral health issues in an upstream and community-based approach [1].
An example of an upstream public health approach that we identified is the integration of fluoride usage and school interventions in Mozambique. In its Health Sector Strategic Plan 2014–2019 [45], Mozambique prioritized access to fluorides through the widespread use of fluoride toothpaste, water fluoridation, and fluoride-based mouthwash for children aged 6–12. Additionally, in its National Oral Health Strategy 2019–2024 [46], the country advanced oral health education and daily interventions such as tooth brushing in schools. These public health strategies hold the potential to enhance the accessibility and affordability of effective upstream interventions, empower individuals with self-care skills for oral hygiene, and cultivate health behaviors that favor oral health [15]. We advocate for low-income countries to share experiences on advancing oral health prevention, promotion, and management services, and to implement the WHO Global Oral Health Action Plan 2023–2030 according to their national priorities and context. This approach mirrors the efforts of South-East Asian countries, as highlighted in the Report for the Regional Meeting for Implementing the Action Plan for Oral Health 2022–2023, where countries emphasized interactions and experience sharing on oral health systems across the region [102].
In addition, our study indicates that data on oral health care utilization, oral health care expenditure, and workforce are very limited in low-income countries, reflecting countries’ low level of investment in progress monitoring and system strengthening for oral health. For example, we only observed three countries (Afghanistan, Burundi, and Rwanda) that included the development of oral health professionals in their national health human resource plans [56, 61, 64]. Furthermore, despite the evidence that out-of-pocket expenditures for oral health care are among the main drivers of catastrophic health expenditures [10, 11], most low-income countries with available expenditure data still require a dominant proportion of payments to be borne by the domestic private sector. Considering that most low-income countries simultaneously lack a provision for WHO-recommended interventions, our study unveiled a worrisome situation of spending valuable out-of-pocket resources on the less-effective and sometimes harmful measures, like the removal of the uvula and dental buds for children [103]. Relying on traditional oral health interventions has been demonstrated as not financially sustainable in low-income countries [104], and we call for policy makers to reconfigure the oral health system and better reorientate public and private financial resources toward recommended evidence-based interventions. Furthermore, the discrepancies in expenditure data between international data sources underscore the need for increased efforts within the international community to coordinate endeavors in data collection. Such coordination is essential in providing policy makers with aligned and reliable measurement results, thereby supporting evidence-based policymaking when allocating financial resources to oral health.
Our study has several limitations. First, when searching for national policies containing oral health information, we used the websites of countries’ health departments and WHO’s existing databases. This approach may overlook oral health information contained in policies released by other departments, such as the education departments. Second, we employed public-facing websites and databases to download national health policy documents. This approach does not eliminate the possibility that oral health policies might be outlined in government internal documents that are not publicly accessible. Additionally, there remains the chance that updated versions of the accessible documents exist, but their existence is unknown to us. For future analyses, we recommend using personal contact to identify dedicated government staff responsible for oral health to locate relevant policy documents.
Conclusions
Our study provides a comprehensive examination of five aspects of universal health coverage for oral health care in low-income countries. Policy integration for oral health care significantly varied across the 27 low-income countries while most countries do not have dedicated national oral health policies and lack services that tackle oral health within the framework of common risk factors with non-communicable diseases. Tooth extraction and other invasive interventions are dominant in low-income countries, with only a few countries adhering to WHO recommendations on the provision of preventive and public health measures for oral health, which is concerning. Financial and human resources are scarce in low-income countries, and more political and resource commitment is needed to reverse the low utilization rates in low-income countries.
Availability of data and materials
All data relevant to the study are included in the article or uploaded as supplementary information.
Abbreviations
- LMICs:
-
Low- and Middle-Income Countries
- NHPSPs:
-
National Health Policies, Strategies, and Plans
- UHC:
-
Universal Health Coverage
- WHO:
-
World Health Organization
- WHA:
-
World Health Assembly
References
Peres MA, Macpherson LM, Weyant RJ, Daly B, Venturelli R, Mathur MR, Listl S, Celeste RK, Guarnizo-Herreño CC, Kearns C, Benzian H. Oral diseases: a global public health challenge. The Lancet. 2019;394(10194):249–60.
Kassebaum NJ, Smith AG, Bernabé E, Fleming TD, Reynolds AE, Vos T, Murray CJ, Marcenes W, GBD 2015 Oral Health Collaborators. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96(4):380–7.
Bale BF, Doneen AL, Vigerust DJ. High-risk periodontal pathogens contribute to the pathogenesis of atherosclerosis. Postgrad Med J. 2017;93(1098):215–20.
Meurman JH, Sanz M, Janket SJ. Oral health, atherosclerosis, and cardiovascular disease. Crit Rev Oral Biol Med. 2004;15(6):403–13.
Lamster IB, Lalla E, Borgnakke WS, Taylor GW. The relationship between oral health and diabetes mellitus. J Am Dent Assoc. 2008;1(139):19S-24S.
Algra Y, Haverkort E, Kok W, Etten-Jamaludin FV, Schoot LV, Hollaar V, Naumann E, Schueren MD, Jerković-Ćosić K. The association between malnutrition and oral health in older people: a systematic review. Nutrients. 2021;13(10):3584.
Global oral health status report: towards universal health coverage for oral health by 2030. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO.
Ruff RR, Senthi S, Susser SR, Tsutsui A. Oral health, academic performance, and school absenteeism in children and adolescents: a systematic review and meta-analysis. J Am Dent Assoc. 2019;150(2):111–21.
Morgan JP, Isyagi M, Ntaganira J, Gatarayiha A, Pagni SE, Roomian TC, Finkelman M, Steffensen JE, Barrow JR, Mumena CH, Hackley DM. Building oral health research infrastructure: the first national oral health survey of Rwanda. Glob Health Act. 2018;11(1):1477249.
Bernabé E, Masood M, Vujicic M. The impact of out-of-pocket payments for dental care on household finances in low- and middle-income countries. BMC Public Health. 2017;17(1):1–8.
Masood M, Sheiham A, Bernabé E. Household expenditure for dental care in low- and middle-income countries. PLoS ONE. 2015;10(4):e0123075.
Listl S. Countries with public dental care coverage have lower social inequalities in the use of dental services than countries without such coverage. J Evid Based Dent Pract. 2015;15(1):41–2.
World Health Organization. Oral Health. World Health Assembly Resolution WHA74/A74.R5. Geneva: World Health Organization, 2021. https://apps.who.int/gb/ebwha/pdf_files/WHA74/A74_R5-en.pdf. Accessed June 2023.
World Health Organization. Landmark global strategy on oral health adopted at World Health Assembly 75. https://www.who.int/news-room/feature-stories/detail/landmark-global-strategy-on-oral-health-adopted-at-world-health-assembly-75.
World Health Organization. Draft Global Oral Health Action Plan (2023–2030). https://www.who.int/publications/m/item/draft-global-oral-health-action-plan-(2023-2030).
World Health Organization. Neglected tropical diseases. https://www.who.int/health-topics/neglected-tropical-diseases#tab=tab_1
World Bank. World Bank Country and Lending Groups. Washington, DC: World Bank, 2020. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed May 2023.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MD, Horsley T, Weeks L, Hempel S. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
World Health Organization. The country planning cycle database. https://extranet.who.int/countryplanningcycles/. Accessed May 2023.
World Health Organization. Non-communicable disease document repository. https://extranet.who.int/ncdccs/documents/Db. Accessed May 2023.
World Health Organization. WHO MiNDbank. https://extranet.who.int/mindbank/. Accessed May 2023.
World Health Organization. Supporting national health policies, strategies, plans. https://www.who.int/activities/supporting-national-health-policies-strategies-plans.
World Health Organization. Promoting Oral Health in Africa: Prevention and control of oral diseases and noma as part of essential noncommunicable disease interventions. https://iris.who.int/handle/10665/205886.
World Health Organization Publications. https://www.who.int/publications. Accessed May 2023.
World Health Organization Country Profile. https://www.who.int/countries. Accessed May 2023.
Global Dental Relief. https://www.globaldentalrelief.org/. Accessed May 2023.
Smailes for Everyone Foundation. https://www.smilesforeveryone.org/. Accessed May 2023.
Global Child Dental Fund. https://www.gcdfund.org/. Accessed May 2023.
Citron I, Chokotho L, Lavy C. Prioritisation of surgery in the National Health Strategic Plans of Africa: a systematic review. World J Surg. 2016;40:779–83.
Landrum K, Cotache-Condor CF, Liu Y, Truche P, Robinson J, Thompson N, Granzin R, Ameh E, Bickler S, Samad L, Meara JG. Global and regional overview of the inclusion of paediatric surgery in the national health plans of 124 countries: an ecological study. BMJ Open. 2021;11(6):e045981.
World Health Organization. Global oral health status report. Country profiles. https://www.who.int/team/noncommunicable-diseases/global-status-report-on-oral-health-2022. Accessed May 2023.
World Health Organization. Global Health Expenditure Database. https://apps.who.int/nha/database/Select/Indicators/en. Accessed May 2023.
World Health Organization. National Health Workforce Account. https://apps.who.int/nhwaportal/Home. Accessed May 2023.
Burkina Faso. Ministere De La Sante. Programme National Des Maladies Non Transmissibles Unite De Sante Orale. Plan D’action Triennal De Lutte Contre Les Maladies Bucco-Dentaires Et Le Noma 2015–2017 [Burkina Faso. Ministry of Health. National Non-Communicable Diseases Program Oral Health Unit. Three-Year Action Plan for the Fight Against Oral Diseases and Noma 2015–2017]. https://extranet.who.int/ncdccs/Data/BFA_B8_Plan%20%20d'Action%20National%20%20Triennal%20Noma%20BURKINA%20FASO%20VF.pdf. Accessed May 2023.
Burkina Faso. Ministere De La Sante. Plan stratégique de santé des personnes âgées 2016–2020 [Burkina Faso. Ministry of Health. Strategic Plan for the Health of the Elderly 2016–2020]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/burkina_faso/plan_strategique_de_sante_des_personnes_agees_2016_-_2020.pdf. Accessed May 2023.
Burkina Faso. Ministere De La Sante. Plan Strategique Integre De Lutte Contre Les Maladies Non Transmissibles 2016–2020 [Burkina Faso. Ministry of Health. Integrated Strategic Plan for the Fight Against Non-Communicable Diseases 2016–2020]. https://extranet.who.int/ncdccs/Data/BFA_B3_Plan%20SIMNT_FINAL_27-09-2016_F.pdf. Accessed May 2023.
République Démocratique du Congo. Ministere De La Sante. Plan Stratégique de la Santé Bucco-Dentaire 2021–2022. [Democratic Republic of Congo. Health Ministry. Oral Health Strategic Plan 2021–2022]. https://extranet.who.int/ncdccs/Data/COD_B8_s21_DRC_Plan%20Strategique%20SBD%202021%202022.docx. Accessed May 2023.
Guiné Bissau. Ministério Da Saúdepública. Programa Nacional de Luta contra Noma Plano de Ação das Atividades 2016. [Guinea-Bissau. Ministry of Public Health. National Program to Fight against Noma Action Plan 2016] https://extranet.who.int/ncdccs/Data/GNB_B8_Plan%20op%c3%a9rationnel%20NOMA2016_GNB.pdf. Accessed May 2023.
Madagascar. Ministere De La Sante Publique. Politique Nationale de Sante Bucco-Dentaire 2010-2020. [Madagascar. Minister of Public Health. National Oral Health Policy 2010-2020]. https://extranet.who.int/ncdccs/Data/MDG_B8_PNSBD%20final_photos%2005_%20juin_10(1).doc. Accessed May 2023.
Madagascar. Ministre de la Sante Publique. Plan de Développement du Secteur Santé 2015–2019. [Madagascar. Minister of Public Health. Health Sector Development Plan 2015–2019]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/madagascar/pdss_2015.pdf. Accessed May 2023.
Madagascar. Ministre de la Santé Publique. Politique Nationale de Lutte Intégrée contre les Maladies Non Transmissibles et de Prévention du Handicap 2017. [Madagascar. Minister of Public Health. National Policy for Integrated Control of Non-Communicable Diseases and Prevention of Disability 2017] https://extranet.who.int/ncdccs/Data/MDG_B3_2%20DOC%20PolitiqueMNT_PH_020718_.pdf. Accessed May 2023.
Madagascar. Ministre de la Santé Publique. Plan Stratégique National de Santé des Personnes Âgées 2018. [Madagascar. Minister of Public Health. National Strategic Plan for Health of the Elderly 2018]. http://www.sante.gov.mg/ministere-sante-publique/wp-content/uploads/2021/07/Plan-Strat%C3%A9gique-National-de-la-Sant%C3%A9-des-Personnes-Ag%C3%A9es-Madagascar.pdf. Accessed May 2023.
Mali. Ministère de la Santé et de l’Hygiène Publique. Ministère du Travail et des Affaires Sociales et Humanitaires. Ministère de la Promotion de la Femme, de la Famille et de l’Enfant. Plan Décennal de Développement Sanitaire et Social (PDDSS) 2014–2023. [Mali. Ministry of Health and Public Hygiene. Ministry of Labor and Social and Humanitarian Affairs. Ministry for the Promotion of Women, Families and Children. Ten-year Health and Social Development Plan 2014–2023]. https://www.childrenandaids.org/sites/default/files/2018-05/Mali_Nat%20Health%20Plan_2014-2023%20fr.pdf. Accessed May 2023.
Mali. Plan Stratégique de Santé Bucco-Dentaire 2018-2022. [Mali. Oral Health Strategic Plan 2018-2022]. https://extranet.who.int/ncdccs/Data/MLI_B8_Plan%20d'Action%20Sant%c3%a9%20Bucco-Dentaire%202018-2022.pdf. Accessed May 2023.
Mozambique. Ministry of Health. Health Sector Strategic Plan 2014–2019. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/mozambique/mozambique_-_health_sector_strategic_plan_-_2014-2019.pdf. Accessed May 2023.
República De Moçambique. Ministério Da Saúde. Direcção Nacional De Assistência Médica Estratégia Nacional de Saúde Oral 2019-2024. [Mozambique. Ministry of Health. National Directorate of Medical Assistance National Oral Health Strategy 2019-2024]. https://extranet.who.int/ncdccs/Data/MOZ_B8_ESTRATEGIA%20NACIONAL%20DE%20SAUDE%20ORAL_%202019%20-%202024%20-final%20Moz.pdf. Accessed May 2023.
República De Moçambique. Ministério Da Saúde. Plano Estratégico Multissectorial de Prevenção e Controlo de Doenças Não Transmissíveis 2020–2029. [Mozambique. Ministry of Health. Strategic Plan Multisectoral of Prevention and Control of Non-Communicable Diseases 2020–2029]. https://extranet.who.int/ncdccs/Data/MOZ_B3_s21_Plano%20Estrat%c3%a9gico%20Multissetorial%20de%20Prevencao%20e%20Controlo%20das%20DNTs%202020-2029%20FINALISSIMA.pdf. Accessed May 2023.
République Du Niger. Ministere De La Sante Publique. Plan Stratégique National Multisectoriel de Lutte contre les Maladies Non Transmissibles 2019–2021. [Niger. Ministry of Health. National Strategic Plan Multisectoral Fight Against Non-Communicable Diseases 2019–2021]. https://extranet.who.int/ncdccs/Data/NER_B3_s21_EXE%20-%20Doucument%20complet%20Valid%c3%a9%20PNLCMNT.pdf. Accessed May 2023.
République Du Niger. Ministere De La Sante Publique. Plan Stratégique National Intégré de Lutte contre les Maladies Bucco-Dentaires et le Noma (PSNILMBD/N) 2021–2025. [Niger. Ministry of Health. Integrated National Strategic Plan for the Fight Against Oral Diseases and Noma 2021–2025]. https://extranet.who.int/ncdccs/Data/NER_B8_s21_PLAN%20Strat%c3%a9gique%20MBD-N.docx. Accessed May 2023.
Rwanda. Ministry of Health. National Community Health Strategic Plan 2013–2018. https://extranet.who.int/mindbank/item/7440. Accessed May 2023.
Rwanda. Ministry of Health. Rwanda non-communicable diseases policy 2015. https://extranet.who.int/ncdccs/Data/RWA_B3_NCDs_Policy.2015.pdf. Accessed May 2023.
Rwanda. Ministry of Health. Health service packages for public health facilities 2017. Available from https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Legal_Framework/Public_health_Facilities_service_packages_in_Rwanda-1.pdf. Accessed May 2023.
Rwanda. Ministry of Health. Fourth health sector strategic plan 2018–2024. https://extranet.who.int/mindbank/item/7442. Accessed May 2023.
Rwanda. Ministry of Health. Service packages for upgraded health centers Rwanda health care system 2019. https://www.moh.gov.rw/index.php?eID=dumpFile&t=f&f=11803&token=c8fe376a7aa067259c7fe35ce5d7c6e078c74f5b. Accessed May 2023.
Rwanda. Ministry of Health. National oral health strategic plan 2019–2024. https://moh.prod.risa.rw/fileadmin/user_upload/Moh/Publications/Strategic_Plan/National_Oral_Health_Strategic_Plan_2019-2024.pdf. Accessed May 2023.
Rwanda. 10-year Government Program: National Strategy for Health Professionals Development 2020–2030. https://www.rbc.gov.rw/fileadmin/user_upload/strategy/RWANDA%20National%20Strategy%20for%20Health%20Professions%20Development%20%28NSHPD%202020-2030%29.pdf. Accessed May 2023.
Uganda. Ministry of Health. Health Sector Development Plan 2015–2020. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/uganda/health_sector_development_plan_2015-16_2019-20_0.pdf. Accessed May 2023.
Uganda. Ministry of Health. National Oral Health Policy. https://extranet.who.int/ncdccs/Data/UGA_B8_National%20Oral%20Health%20Policy.pdf. Accessed May 2023.
Islamic Republic of Afghanistan. Ministry of Public Health. The Essential package of hospital services for Afghanistan 2005/1384. https://platform.who.int/docs/default-source/mca-documents/policy-documents/guideline/afg-cc-46-01-guideline-2005-eng-essential-hospital-services.pdf. Accessed May 2023.
World Health Organization. WHO MiNDbank. https://extranet.who.int/mindbank/item/5613. Accessed May 2023.
Islamic Republic of Afghanistan 2011. Ministry of Public Health. Afghanistan National Health Workforce Plan 2012–2016. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/afghanistan/afghanistan_hrhplan_2012-2016_draft.pdf. Accessed May 2023.
Islamic Republic of Afghanistan. Ministry of Public Health. National Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCAH) Strategy 2017–2021. https://rmncah-moph.gov.af/wp-content/uploads/2017/11/National-RMNCAH-Strategy-2017-2021-English-Final.pdf. Accessed May 2023.
Islamic Republic of Afghanistan. Ministry of Public Health. Normative costing of basic package of health services (BPHS) 2020. https://moph.gov.af/sites/default/files/2020-11/BPHS%20Costing%20final%20Report%207-Nov-%202020_.pdf. Accessed May 2023.
Republique Du Burundi. Ministere De La Sante Publique Et De La Lutte Contre Le Sida. Profil De Ressources Humaines En Sante Du Burundi 2011. [Republic of Burundi. Ministry of Public Health and the Fight Against AIDS. Profile of Human Resources in Health of Burundi 2011]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/burundi/profil_rh_vf_22_janvier_20121.pdf. Accessed May 2023.
Republique Du Burundi. Politique Nationale de Sante 2016–2025. [Republic of Burundi. National Health Policy 2016–2025]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/burundi/pns_2016_2025_burundi.pdf. Accessed May 2023.
Republique Du Burundi. Ministere De La Sante Publique Et De La Lutte Contre Le Sida. Plan D’Action Multisectoriel De Prevention Et De Controle Des Maladies Non Transmissibles 2019–2023. [Republic of Burundi. Ministry of Public Health and the Fight Against AIDS. Multisectoral Action Plan for the Prevention and Control of Non-Communicable Diseases 2019–2023]. https://extranet.who.int/ncdccs/Data/BDI_B3_PAM%20FINAL%2023%2007%202019.pdf. Accessed May 2023.
République Centr Africaine. Ministere De La Sante Publique. Document De Politique Nationale De Prevention Et De Lutte Contre Les Maladies Non Transmissibles 2014. [Central African Republic. Minister of Public Health. National Policy Document for the Prevention and Fight Against Non-Communicable Diseases 2014]. https://extranet.who.int/ncdccs/Data/CAF_B3_POLITIQUE%20MNT%20REPUBLIQUE%20CENTRAFRICAINE.pdf. Accessed May 2023.
République Centr Africaine. Ministere De La Sante Publique. Plan de Transition du Secteur Santé en République Centrafricaine 2015–2017. [Central African Republic. Minister of Public Health. Health Sector Transition Plan 2015–2017]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/central_african_republic/rca_-ptss_revise_final_26092016.pdf. Accessed May 2023.
République du Tchad. Ministère de la Santé Publique. Plan Multisectoriel de Lutte et de Contrôle des Maladies Non Transmissibles 2017-2021. [Republic of Chad. Minister of Public Health. Multisectoral Plan for the Fight and Control of Non-Communicable Diseases 2017-2021]. https://extranet.who.int/ncdccs/Data/TCD_B3_PLAN%20MULTISEC%20MNT.pdf. Accessed May 2023.
Eritrea. Ministry of Health. The Second Health Sector Strategic Development Plan II 2017–2021. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/eritrea/eritrea_hssdp_ii_21022017.pdf. Accessed May 2023.
Eritrea. Ministry of Health. Strategic Plan for the Implementation of Reproductive, Maternal, Newborn, Child and Adolescent Health and Healthy Ageing Programmes in Eritrea 2022–2026. https://www.afro.who.int/sites/default/files/2022-09/2022_RMNCAH_Eritrea.pdf. Accessed May 2023.
Ethiopia. Ministry of Health. Health Sector Transformation Plan 2015–2020. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/ethiopia/hstp_ethiopia.pdf. Accessed May 2023.
Ethiopia. Ministry of Health. Essential Health Services Package 2019. https://www.uib.no/sites/w3.uib.no/files/attachments/essential_health_service_package_ethiopia_2019_0.pdf. Accessed May 2023.
Ethiopia. Ministry of Health. National Strategic Plan for the Prevention and Control of Major Non-Communicable Diseases 2021-2025. https://extranet.who.int/ncdccs/Data/ETH_B3_s21_National_Strategic_Plan_for_Prevention_and_Control_of_NCDs2021.pdf. Accessed May 2023.
Gambia. Ministry of Employment and Social Welfare. National Ageing policy ageing with security and dignity 2010. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/gambia/national_ageing_policy_2010.pdf. Accessed May 2023.
Gambia. Ministry of Health and Social Welfare. National health strategic plan 2014–2020. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/gambia/gnhsp_-_final_draft_13oct2014.pdf. Accessed May 2023.
Gambia. Ministry of Health. National multi-sectoral strategy and costed action plan for non-communicable disease prevention and control in The Gambia 2022–2027. Available from https://www.afro.who.int/sites/default/files/2022-07/National%20Multi-sectoral%20Strategy%20and%20Costed%20Action%20Plan%20for%20NCD%20prevention%20and%20control%20-Gambia%202022-27.pdf. Accessed May 2023.
Guinee. Ministere De La Sante. Plan national de développement sanitaire 2015–2024. [Guinea. Ministry of Health. National Health Development Plan 2015–2024]. https://extranet.who.int/countryplanningcycles/sites/default/files/public_file_rep/GIN_Guinea_Plan-national-de-developmment-sanitaire_2015-2024.pdf. Accessed May 2023.
Liberia. Ministry of Health. Essential Package of health services for universal health coverage 2022. https://www.dcp-3.org/sites/default/files/resources/MOH%20EPHS%20for%20UHC_Final%20Version%2020221121.pdf. Accessed May 2023.
Malawi. Ministry of Health. Health Sector Strategic Plan II 2017–2022. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/malawi/health_sector_strategic_plan_ii_030417_smt_dps.pdf. Accessed May 2023.
Sierra Leone. Ministry of Health and Sanitation. Basic package of essential health services 2015–2020. https://mohs2017.files.wordpress.com/2017/06/gosl_2015_basic-package-of-essential-health-services-2015-2020.pdf. Accessed May 2023.
Sierra Leone. Ministry of Health and Sanitation. Non-communicable disease (NCDs) Strategic Plan 2020-2024. https://extranet.who.int/ncdccs/Data/SLE_B3_s21_NCD%20strategic%20plan%202020-2024%2023Feb2020%20FINAL%20signed%20CF%20(1).docx. Accessed May 2023.
Somalia. Ministry of Health and Human Services. Essential package of health services 2020. https://reliefweb.int/attachments/981c3ca3-6914-3d40-824a-bac5889d906c/somalia_ephs_web.pdf. Accessed May 2023.
République Togolaise. Ministere De La Sante Et De La Protection Sociale. Plan National de Developpment Sanitaire 2017–2022. [Togo. Ministry of Health and Social Protection. National Health Development Plan 2017–2022]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/togo/togo_pnds_2017-2022_version_definitive_210217_en_edition.pdf. Accessed May 2023.
République Togolaise. Ministere De La Sante Et De L’Hygiene Publique. Politique et Plan Stratégique Multisectoriel de Lutte contre les Maladies Non Transmissibles 2018–2022 [Togo. Ministry of Health and Public Hygiene. Policy and Multisectoral Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2018–2022]. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/togo/togo_pnds_2017-2022_version_definitive_210217_en_edition.pdf. Accessed May 2023.
Democratic People’s Republic of Korea. Ministry of Public Health. Medium term strategic plan for the development of the health sector DPR Korea 2016–2020. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/democratic_peoples_republic_of_korea/dpr_korea_medium_term_strategic_plan_2016-20.pdf. Accessed May 2023.
South Sudan. Ministry of Health. National Health Policy 2016–2026. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/south_sudan/south_sudan_national_health_policy_2016_to_2025_2.pdf. Accessed May 2023.
Sudan. National Health Sector Strategic Plan II 2012–2016. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/sudan/sudan_national_health_sector_strategic_plan_nhssp_2012-2016.pdf. Accessed May 2023.
Yemen. Ministry of Public Health & Population. National Health Strategy 2010–2025. Available from https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/yemen/nat_health_strategy_-_yemen_eng.pdf. Accessed May 2023.
Frencken JE, Holmgren CJ, Helderman WH. Basic package of oral care. WHO Collaborating Centre for Oral Health Care Planning and Future Scenarios; 2002. http://www.chdentalinstitute.org/images/bpoc.pdf.
Diendéré J, Ouattara S, Kaboré J, Traoré I, Zeba AN, Kouanda S. Oral hygiene practices and their sociodemographic correlates among adults in Burkina Faso: results from the First National Survey. BMC Oral Health. 2022;22(1):1–6.
Pengpid S, Peltzer K. Prevalence and correlates of dental service utilisation among a national general adult population sample in Sudan. BMC Oral Health. 2021;21(1):1–8.
Ghotane SG, Challacombe SJ, Don-Davis P, Kamara D, Gallagher JE. Unmet need in Sierra Leone: a national oral health survey of schoolchildren. BDJ open. 2022;8(1):16.
Bassa S, Workie SB, Kassa Y, Tegbaru DW. Prevalence of dental caries and relation with nutritional status among school-age children in resource limited setting of southern Ethiopia. BMC Oral Health. 2023;23(1):84.
Mohammed HM, Mehari MA, Asgedom AA. Predictors of low dental service utilization among school children in Mekelle, Northern Ethiopia: a cross-sectional study. BMC Oral Health. 2023;23(1):41.
Salih MA, Ali RW, Nasir EF. Oral health status and associated factors among Sudanese older adults: a cross-sectional study. Gerodontology. 2022;39(4):408–17.
Khalifa N, Allen PF, Abu-bakr NH, Abdel-Rahman ME, Abdelghafar KO. A survey of oral health in a Sudanese population. BMC Oral Health. 2012;12:1–9.
Ocwia J, Olum R, Atim P, Laker F, Okot J, Sereke SG, Baluku JB, Kiguli S, Bongomin F. Oral health seeking behaviors of adults in Nebbi District, Uganda: a community-based survey. BMC Oral Health. 2021;21:1–7.
Binagwaho A, Kyamanywa P, Farmer PE, Nuthulaganti T, Umubyeyi B, Nyemazi JP, Mugeni SD, Asiimwe A, Ndagijimana U, Lamphere McPherson H, Ngirabega JD. The human resources for health program in Rwanda—a new partnership. N Engl J Med. 2013;369(21):2054–9.
Ghotane SG, Don-Davis P, Kamara D, Harper PR, Challacombe SJ, Gallagher JE. Needs-led human resource planning for Sierra Leone in support of oral health. Hum Resour Health. 2021;19:1–7.
Gallagher JE, Mattos Savage GC, Crummey SC, Sabbah W, Varenne B, Makino Y. Oral health workforce in Africa: a scarce resource. Int J Environ Res Public Health. 2023;20(3):2328.
Report of the Regional Meeting for Implementing the Action Plan for Oral Health, 2022–2030. New Delhi: World Health Organization, Regional Office for South-East Asia; 2023. Licence: CC BY-NC-SA 3.0 IGO.
Agbor AM, Naidoo S. A review of the role of African traditional medicine in the management of oral diseases. Afr J Tradit Complement Altern Med. 2016;13(2):133–42.
Kathmandu RY. The burden of restorative dental treatment for children in third world countries. Int Dent J. 2002;52(1):1–9.
Acknowledgements
Not applicable.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
YL, DS, AJ, and CL contributed to study conceptualization. YL, DS, AJ, DL, NA, YZ, JC, MB, JW, XL, ZC, and CL contributed to literature search and review, data extraction, and formal analysis. YL and JW contributed to figure and table creation under CL’s supervision. YL, AJ, JW, and CL contributed to writing the original draft. DS, DL, NA, YZ, JC, MB, XL, and ZC contributed to manuscript review and editing. YL and JW directly accessed and verified the underlying data reported in the manuscript. All authors had access to the data for this study and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Luan, Y., Sardana, D., Jivraj, A. et al. Universal coverage for oral health care in 27 low-income countries: a scoping review. glob health res policy 9, 34 (2024). https://doi.org/10.1186/s41256-024-00376-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41256-024-00376-9