
Abstract
Background
Breast cancer (BC) is the most common female cancers in many countries including Syria. Familial breast cancer or previous family cancer history are considered significant risk factors. Therefore, detecting the prevalence and founder mutations in the population facilitates genetic counselling, risk assessment and the development of a cost-effective screening strategy. In this study, we investigated the three germ-line founder mutations in the BRCA1/2 genes: [NM_007294.4 (BRCA1):c.68_69del (p.Glu23fs), NM_007294.4 (BRCA1):c.5266dup (p.Gln1756fs) and NM_000059.4 (BRCA2):c.5946del (p.Ser1982fs)], to examine their incidence and frequency in early-onset breast cancer cases and determine if they are connected to familial breast cancer. One hundred early diagnosed BC females (≤ 40 years old) with no other type of cancer were recruited. Genomic DNA was isolated from peripheral blood samples, and mutations were investigated using the Amplification-Created Restriction Site (ACRS) method.
Results
The family history of cancer was observed in 61% of the cases, of which 35% were breast cancer; however, none of the screened mutations were detected among BC patients.
Conclusions
The investigated germ-line mutations were not common among Syrian female patients with early-onset BC and were not associated with familial BC. Other mutations in the BRCA1/2 genes or other genes may have a contributing role. Future studies and the need to launch nationwide mutation screening tests for BRCA 1/BRCA2 in the Syrian population are recommended.
Similar content being viewed by others

Background
Breast cancer (BC) is the most common and severe female cancer worldwide. Despite rigorous efforts in early detection and treatment, BC remains one of the significant causes of death claiming the lives of hundreds of thousands annually [1]. In Syria, cancer comes third among death causes and BC is the most common cancer in females forming 30% of all cancer cases [2]. The aetiology of BC was intensively studied, and mutations in candidate genes like the tumour suppressor genes BRCA1 and BRCA2 responsible for DNA repair and the maintenance of chromosomal stability were considered major risk factors for breast carcinogenesis [3,4,5]. Family history of cancer especially breast/ovarian cancer is also considered a risk factor and a critical contributor to the BC. Germ-line mutation screening is important to identify women at risk, in addition to its impact on prognosis, diagnosis and targeted therapy [6, 7]. Investigators have discovered that founder mutations are often responsible for the high prevalence of genetic disease in particular populations [8]. Specific germ-line mutations in the BRCA genes were described as founder mutations [4] and have been detected in hereditary breast cancer in many populations such as in Latin America and Korea [9,10,11]. Generally, most of the techniques used for mutation detection are unable to detect the numerous deleterious mutations as large deletions or insertions account for 5–15% of the total mutations. Thus, screening for founder mutations is a cost-efficient approach [12].
Mutation detection studies on BC patients are very limited in Syria. This study focused on the three germ-line founder mutations in the BRCA1/2 genes: NM_007294.4 (BRCA1):c.68_69del (p.Glu23fs), NM_007294.4 (BRCA1):c.5266dup (p.Gln1756fs) and NM_000059.4 (BRCA2):c.5946del (p.Ser1982fs) to examine their incidence and frequency in early-onset breast cancer cases, and determine their association with familial breast cancer.
Methods
Study criteria
One hundred BC female patients with early diagnosis age (≤ 40 years old) and no other type of cancer were recruited into the study. The selection of patients was independent of any previous cancer family history. Patients were informed about the study and asked to sign a written consent before participation. Clinical data were extracted from the pathological and medical reports archived in patients’ own files at al-Biruni University Hospital, where patients receive their treatments. Peripheral blood samples were collected from the patients into EDTA tubes. Samples were collected between August–November 2019 and September 2020. The study protocol was in agreement with the Declaration of Helsinki guidelines1975, as revised in 2000.
Mutation analysis
Genomic DNA extraction
Genomic DNA (gDNA) was isolated from blood samples using Vivantis Technologies, GF-1, Blood DNA Extraction Kit, Malaysia, according to the manufacturer’s instructions. Purity and concentrations were tested by spectrophotometer (Nanodrop 2000, Thermo Scientific). DNA samples were stored at − 80°C until further analysis.
The amplification-created restriction site (ACRS) method
Mutations were screened using the Amplification-Created Restriction Site (ACRS) method. Briefly, the selected method enables the formation or deletion of a restriction enzyme site in a mutated or wild-type (WT) allele using a PCR primer with a mismatched nucleotide. Mutated alleles are differentiated from WT by size. The primers used to amplify the region around the BRCA1 c.68_69del (p.Glu23fs) and BRCA2 c.5946del (p.Ser1982fs) mutations were self-designed using AmplifX pro, and Eurofins Genomics' Oligo Analysis Tool. Primer and sequences are shown in Table 1. All PCR reactions contained: 12.5 μl of One PCR™ Mix (2X) (Gene Direx, Inc), 1 μl of each forward and reverse primers (10 μM), 80 ng of the gDNA, and the appropriate amount of nuclease-free water to reach the final volume 25 μl. Each PCR experiment included a negative control in which gDNA was replaced with the same volume of distilled water for contamination control. The PCR reactions were performed using the Eppendorf Master cycler.
HinfI restriction enzyme 2000 U (Thermo Scientific, USA) and DraIII restriction enzyme 1000 U (BioLabs, USA) were used to identify and cut the WT-modified allele of the BRCA1 c.68_69del (p.Glu23fs) and BRCA2 c.5946del (p.Ser1982fs) mutations, respectively. BstNI restriction enzyme 2000U (Thermo Scientific, USA) was used for the detection of the BRCA1 c.5266dup (p.Gln1756fs) mutation by recognizing and cutting the mutant-modified allele. All digestion reactions contained: 10 µl of the PCR product, 2 µl of the enzyme buffer, 1 µl of the restriction enzyme and 18 µl of nuclease-free water. Digestion reactions were done according to manufacturer’s instructions. Fragments were analysed by3% agarose gel electrophoresis using 100 bp DNA Ladder (Thermo Scientific, GeneRuler), visualized and photographed using a UV transilluminator (Olympus). Validation of BstNI restriction enzyme functionality, and confirmation of restriction site creation for the BRCA1 c.5266dup (p.Gln1756fs) mutation (since no cut is expected for WT genotype), was tested on a sample of a healthy control by DNA sequencing using Big Dye Terminator chemistry (Applied Biosystems, version 3.1) following the manufacturer’s instructions.
Results
One hundred early-onset breast cancer Syrian females participated in this study. Patients' ages at the time of diagnosis ranged between 20 and 40 years, with an average age of 32.5 years old.
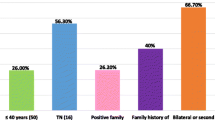
Patients were from the various Syrian governorates, particularly Damascus and its countryside (33%), and none were of Jewish population descendants. According to our findings, 61% of the patients had a family history of cancer (61/100), and over one-third had a positive family history of breast cancer (35/100), as shown in Table 2.
Clinical data retrieved from patients' files showed that 57% of the patients had cancer in the left breast, 40% had cancer in the right breast, and only 3% had bilateral BC. Unfortunately, data regarding the histological grade and type of BC for some patients were missing from their medical files. However, out of 86 patients, 48.84% (42/86) had grade II, 51.16% (44/86) had grade III BC and none had grade I. Of 88 patients, 88.64% (78/88) had ductal carcinoma, 6.82% (6/88) had lobular carcinoma, and 4.55% (4/88) had both ductal and lobular carcinomas. Furthermore, the hormone receptors status was as follows: of 96 patients, ER status was positive in 64.58% (62/96), PR was positive in 59.38% (57/96), and HER2 was positive in 46.88% (45/96). Triple-negative BC phenotype was found in 9 patients (group1), and triple-positive was found in 18(group5). Table 3 displays detailed information about the status of the hormone receptors.
The expected sizes were achieved by amplifying the regions surrounding the three studied mutations using the specifically designed primers. Confirmation of restriction site creation near the sequence variant for the BRCA1 c.5266dup (p.Gln1756fs) mutation was confirmed by DNA sequencing as shown in Fig. 1. None of the three studied germ-line founder mutations in the BRCA1/2 genes were detected in BC patients (Figs. 2, 3, 4).

Sequence alignment result of a healthy control sample against the reference BRCA1 genome using Uber Geneious 4.8.4 bioinformatics tool. Creation of the restriction site near the sequence variant for the BRCA1:c.5266dup (p.Gln1756fs) mutation was successfully generated; the inserted T nucleotide was marked in red

Agarose gel electrophoresis (3%) of PCR and digested products for the detection of the BRCA1:c.68_69del (p.Glu23fs) mutation. HinfI restriction enzyme was used which identifies and cuts the wild-type (WT) modified allele yielding a 150 + 20 bp bands. M: 100 bp DNA Ladder, Lane 1&9: ACRS-PCR amplified product (170 bp), Lanes 2–8: one digest product (150 bp) correspond to homo WT genotype

Agarose gel electrophoresis (3%) of PCR and digested products for the detection of the BRCA1:c.5266dup (p.Gln1756fs) mutation. BstNI restriction enzyme was used which identifies and cuts the mutated modified allele. M: 100 bp DNA Ladder, Lane 1: ACRS-PCR amplified product (273 bp), Lanes 2–7: one undigested product (273bp) correspond to homo WT genotype. Note that if the mutant allele was present two distinctive bands must be recognized (250 + 23 bp)

Agarose gel electrophoresis (3%) of PCR and digested products for the detection of the BRCA2:c.5946del (p.Ser1982fs) mutation. DraIII restriction enzyme was used which identifies and cuts the wild-type (WT) modified allele yielding a 333 + 23 bp bands. M: 100 bp DNA Ladder, Lane 1&6: ACRS-PCR amplified product (356bp), Lanes 2–5: one digest product (333bp) correspond to homo WT genotype
Discussion
Breast cancer commonly occurs as a sporadic event; however, approximately 10–15% of cases are considered to be hereditary. The possibility of developing breast cancer increases when there is a family history and cancer is diagnosed at an early age [15]. Molecular testing has become an integral part of breast cancer management globally; patients are usually offered a genetic test to determine if an inherited cancer syndrome is present [16]. Early diagnosis and treatment can be successfully achieved by the identification of patients at risk for hereditary breast cancer [6]. Furthermore, breast cancer risk is greatly increased due to certain germ-line mutations, like those in the BRCA1 and BRCA2 genes, reaching up to 25% [17]. Previous reports revealed that in particular populations such as the Ashkenazi Jewish, Moroccan, South Asia, and in some European countries, the BRCA1 c.68_69del (p.Glu23fs), the BRCA1 c.5266dup (p.Gln1756fs) and the BRCA2 c.5946del (p.Ser1982fs) mutations are commonly found and are considered as founder mutations [13, 18,19,20,21,22]. In this study, the three germ-line founder mutations mentioned above were investigated for possibly present in 100 early diagnosed breast cancer patients, but none were detected. To the best of our knowledge, this study is the first to investigate the BRCA1 c.5266dup (p.Gln1756fs) mutation and the second to report the status of the two mutations [BRCA1 c.68_69del (p.Glu23fs) and BRCA2 c.5946del (p.Ser1982fs)] among early-onset breast cancer patients in Syria. A previous study by Khalil et al. [23] conducted on 50 Syrian BC patients showed similar results. Therefore, one could conclude that the three studied mutations are not associated with familial breast cancer or have any role in the clinical presentation of early-onset breast cancer in Syrian females. Numerous studies have examined germ-line mutations in the BRCA1/2 genes among diverse populations, and have resulted in contradictory conclusions. For example, none of the screened mutations in our study were found in some neighbouring countries such as Jordan, where the whole coding exons and the flanking intronic regions of the BRCA1/BRCA2 genes were screened. Also in Lebanon, where high-risk breast cancer Lebanese patients were studied, and in Saudi Arabia where Arab breast and ovarian cancer patients were studied [24,25,26]. However, the frequency of the screened mutations in Egypt varied among different studies [27, 28], and interestingly, the two common germ-line founder mutations in the BRCA1 gene were also found in a cohort of familial ovarian cancer Egyptian patients [29]. Furthermore, in Tunisia, the frequency of the BRCA1 c.5266dup (p.Gln1756fs) mutation differed also among early diagnosed patients with a positive family history of breast cancer [30, 31]. Additionally, it was suggested that beside a positive family history or early diagnose, triple-negative breast cancer genotype should be evaluated in the guidelines for genetic analysis of the BRCA1 and BRCA2 genes [32]. Studies found that the BRCA1 c.5266dup (p.Gln1756fs) mutation could be considered as an effective selective criterion for genetic test among triple-negative breast cancer patients [33, 34]. Nevertheless, in our study, this mutation was not found among our patients (group 1). These results suggest that the commonly studied mutations found in some populations may not exist in our population.
Conclusion
The germ-line founder mutations screened in this study were not common, not connected to familial breast cancer or have any role in the clinical presentation of the studied Syrian early-onset breast cancer females. Different founder mutations in the BRCA1/2 genes or in other genes may be responsible. Our findings added substantial data to the scientific literature regarding the Syrian population and emphasized the need to launch a nationwide screening test for BRCA 1/BRCA2 in the Syrian population.
Availability of data and materials
All the datasets were presented in this study, and any additional data are available from the corresponding author on reasonable request.
Abbreviations
- ACRS:
-
Amplification-created restriction site
- BC:
-
Breast cancer
- BRCA1:
-
Breast cancer1 gene
- BRCA2:
-
Breast cancer 2 gene
- DNA:
-
Deoxyribonucleic acid
- EDTA:
-
Ethylenediaminetetraacetic acid
- ER:
-
Estrogen receptor
- HER2:
-
Human epidermal growth factor receptor 2
- gDNA:
-
Genomic DNA
- PCR:
-
Polymerase chain reaction
- PR:
-
Progesterone receptor
- WT:
-
Wild type
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249. https://doi.org/10.3322/caac.21660
Simaan S, Jerf FA (2018) Cancer in Syria (magnitude of the problem). Int J Cancer Treat 1:1–10
Shiovitz S, Korde LA (2015) Genetics of breast cancer: a topic in evolution. Ann Oncol 26(7):1291–1299. https://doi.org/10.1093/annonc/mdv022
Lavoro A, Scalisi A, Candido S, Zanghì GN, Rizzo R, Gattuso G, Falzone L (2022) Identification of the most common BRCA alterations through analysis of germline mutation databases: is droplet digital PCR an additional strategy for the assessment of such alterations in breast and ovarian cancer families? Int J Oncol 60(5):1–13. https://doi.org/10.3892/ijo.2022.5349
Tutt A, Ashworth A (2002) The relationship between the roles of BRCA genes in DNA repair and cancer predisposition. Trends Mol Med 8(12):571–576. https://doi.org/10.1016/s1471-4914(02)02434-6
Liu L, Hao X, Song Z, Zhi X, Zhang S, Zhang J (2021) Correlation between family history and characteristics of breast cancer. Sci Rep 11(1):6360. https://doi.org/10.1038/s41598-021-85899-8
Talwar V, Rauthan A (2022) BRCA mutations: implications of genetic testing in ovarian cancer. Indian J Cancer. https://doi.org/10.4103/ijc.IJC_1394_20
Evans JA (2015) Old meets new: identifying founder mutations in genetic disease. CMAJ 187(2):93–94. https://doi.org/10.1503/cmaj.141509
Ashton-Prolla P, Vargas FR (2014) Prevalence and impact of founder mutations in hereditary breast cancer in Latin America. Genet Mol Biol 37:234–240. https://doi.org/10.1590/s1415-47572014000200009
Ewald IP, Izetti P, Vargas FR, Moreira MAM, Moreira AS, Moreira-Filho CA et al (2011) Prevalence of the BRCA1 founder mutation c.5266dupin Brazilian individuals at-risk for the hereditary breast and ovarian cancer syndrome. Hered Cancer Clin Pract 9:1. https://doi.org/10.1186/1897-4287-9-12
Kang E, Kim SW (2013) The Korean hereditary breast cancer study: review and future perspectives. J Breast Cancer 16(3):245–253. https://doi.org/10.4048/jbc.2013.16.3.245
Neuhausen SL (2000) Founder populations and their uses for breast cancer genetics. Breast Cancer Res. https://doi.org/10.1186/bcr36
Dillenburg CV, Bandeira IC, Tubino TV, Rossato LG, Dias ES, Bittelbrunn ACS (2012) Prevalence of 185delAG and 5382insC mutations in BRCA1, and 6174delT in BRCA2 in women of Ashkenazi Jewish origin in southern Brazil. Genet Mol Biol 35:599–602. https://doi.org/10.1590/S1415-47572012000400009
Rohlfs EM, Learning WG, Friedman KJ, Couch FJ, Weber BL, Silverman LM (1997) Direct detection of mutations in the breast and ovarian cancer susceptibility gene BRCA1 by PCR-mediated site-directed mutagenesis. Clin Chem 43(1):24–29. https://doi.org/10.1093/clinchem/43.1.24
Huber-Keener KJ (2022) Cancer genetics and breast cancer. Best Pract Res Clin Obstet Gynaecol 82:3–11. https://doi.org/10.1016/j.bpobgyn.2022.01.007
Litton JK, Burstein HJ, Turner NC (2019) Molecular testing in breast cancer. Am Soc Clin Oncol Educ Book 39:e1-7. https://doi.org/10.1200/edbk_237715
Petrucelli N, Daly MB, Pal T (1998–2024) BRCA1- and BRCA2-associated hereditary breast and ovarian Cancer. In: Adam MP, Feldman J, Mirzaa GM, et al (eds) GeneReviews®. University of Washington, Seattle. https://www.ncbi.nlm.nih.gov/books/NBK1247/
Cox DM, Nelson KL, Clytone M, Collins DL (2018) Hereditary cancer screening: case reports and review of literature on ten Ashkenazi Jewish founder mutations. Mol Genet Genomic Med 6(6):1236–1242. https://doi.org/10.1002/mgg3.460
Quiles F, Teulé À, Martinussen Tandstad N, Feliubadaló L, Tornero E, Del Valle J et al (2016) Identification of a founder BRCA1 mutation in the Moroccan population. Clin Genet 90(4):361–365. https://doi.org/10.1111/cge.12747
Kharel S, Shrestha S, Yadav S, Shakya P, Baidya S, Hirachan S (2022) BRCA1/BRCA2 mutation spectrum analysis in South Asia: a systematic review. J Int Med Res 50(1):3000605211070757. https://doi.org/10.1177/03000605211070757
Hamel N, Feng BJ, Foretova L, Stoppa-Lyonnet D, Narod SA, Imyanitov E et al (2011) On the origin and diffusion of BRCA1 c. 5266dupC (5382insC) in European populations. Eur J Hum Genet 19(3):300–306. https://doi.org/10.1038/ejhg.2010.203
Heramb C, Wangensteen T, Grindedal EM, Ariansen SL, Lothe S, Heimdal KR et al (2018) BRCA1 and BRCA2 mutation spectrum—an update on mutation distribution in a large cancer genetics clinic in Norway. Hered Cancer Clin Pract 16:1. https://doi.org/10.1186/s13053-017-0085-6
Khalil H, Monem F (2018) Identification of three BRCA1/2 mutations and a study of the likelihood of an association with certain characteristics in Syrian familial breast cancer patients. Middle East J Cancer 9(4):274–281. https://doi.org/10.30476/mejc.2018.42135
Abu-Helalah M, Azab B, Mubaidin R, Ali D, Jafar H, Alshraideh H et al (2020) BRCA1 and BRCA2 genes mutations among high risk breast cancer patients in Jordan. Sci Rep 10:1. https://doi.org/10.1038/s41598-020-74250-2
Farra C, Dagher C, Badra R, Hammoud MS, Alameddine R, Awwad J et al (2019) BRCA mutation screening and patterns among high-risk Lebanese subjects. Hered Cancer Clin Pract 17(1):4. https://doi.org/10.1186/s13053-019-0105-9
Alhuqail A-J, Alzahrani A, Almubarak H, Al-Qadheeb S, Alghofaili L, Almoghrabi N et al (2018) High prevalence of deleterious BRCA1 and BRCA2 germline mutations in Arab breast and ovarian cancer patients. Breast Cancer Res Treat 168(3):695–702. https://doi.org/10.1007/s10549-017-4635-4
Abou-El-Naga A, Shaban A, Ghazy H, Elsaid A, Elshazli R, Settin A (2018) Frequency of BRCA1 (185delAG and 5382insC) and BRCA2 (6174delT) mutations in Egyptian women with breast cancer compared to healthy controls. Meta Gene 15:35–41. https://doi.org/10.1016/j.mgene.2017.11.002
Mogahed SHG, Hamed YS, Moursy YEI, Saied MHM (2020) Analysis of heterozygous BRCA1 5382ins founder mutation in a cohort of Egyptian breast cancer female patients using pyrosequencing technique. Asian Pac J Cancer Prevent. https://doi.org/10.31557/APJCP.2020.21.2.431
Rizk MM, El-etreby NM, El-Attar LM, Elzyat EA, Saied MH (2022) A case–control study of BRCA1 founder mutations 185delAG and 5382insC in a cohort of Egyptian ovarian cancer patients using pyrosequencing technique. Egypt J Med Hum Genet 23:1. https://doi.org/10.1186/s43042-022-00226-8
Riahi A, Ghourabi ME, Fourati A, Chaabouni-Bouhamed H (2017) Family history predictors of BRCA1/BRCA2 mutation status among Tunisian breast/ovarian cancer families. Breast Cancer 24(2):238–244. https://doi.org/10.1007/s12282-016-0693-4
Mahfoudh W, Bouaouina N, Ahmed SB, Gabbouj S, Shan J, Mathew R et al (2012) Hereditary breast cancer in Middle Eastern and North African (MENA) populations: identification of novel, recurrent and founder BRCA1 mutations in the Tunisian population. Mol Biol Rep 39(2):1037–1046. https://doi.org/10.1007/s11033-011-0829-8
Robertson L, Hanson H, Seal S, Warren-Perry M, Hughes D, Howell I et al (2012) BRCA1 testing should be offered to individuals with triple-negative breast cancer diagnosed below 50 years. Br J Cancer 106(6):1234–1238. https://doi.org/10.1038/bjc.2012.31
Mahfoudh W, Bettaieb I, Ghedira R, Snoussi K, Bouzid N, Klayech Z et al (2019) Contribution of BRCA1 5382insC mutation in triple negative breast cancer in Tunisia. J Transl Med. https://doi.org/10.1186/s12967-019-1873-8
Samusieva A, Serga S, Klymenko S, Rybchenko L, Klimuk B, Zakhartseva L et al (2022) Contribution of BRCA1 5382insC mutation to triplene-gative and luminal types of breast cancer in Ukraine. Breast Cancer Res Treat 195(3):453–459. https://doi.org/10.1007/s10549-022-06692-3
Acknowledgements
The authors would like to acknowledge all participants for taking part in the study. The authors also thank the medical teams of nurses and technicians at al Biruni University Hospital, for their assistance.
Funding
This research was funded from university resources, Grant No. 2948.
Author information
Authors and Affiliations
Contributions
SWZ contributed to study design, collected blood samples, performed molecular study, analysed data and results and revised the manuscript. GC was involved in study design, analysed data and results and contributed to writing and revising the manuscript. MS was involved in revising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Damascus University in Syria. All methods were carried out in accordance with the Declaration of Helsinki. All participants were fully informed about the study, and informed consent was obtained from each participant before admitted into the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wahabi Alzahabi, S., Saifo, M. & Abou Alchamat, G. BRCA mutations: screening for germ-line founder mutations among early-onset Syrian breast cancer patients. Egypt J Med Hum Genet 25, 18 (2024). https://doi.org/10.1186/s43042-024-00492-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-024-00492-8