
Abstract
Background
Contrast-enhanced MRI is frequently used as a baseline modality and indispensable tool for early diagnosis and follow-up of different brain lesions. Herein, we aimed to evaluate the diagnostic impact of contrast-enhanced FLAIR compared to the widely used post-contrast T1W sequence in terms of demyelinating and infectious brain lesions detection in clinical practice and explore its value in monitoring disease activity for selecting appropriate therapy. MR Imaging was performed using 1.5 Tesla device. Both T1W and FLAIR sequences were obtained prior to and after administration of intravenous gadolinium-based contrast agent. Both qualitative and quantitative approaches were used for image analysis by two independent radiologists.
Results
Sixty patients were prospectively enrolled in this study. Our participants were subdivided into two categories, either demyelinating (45 multiple sclerosis) or infectious lesions (13 meningitis/meningoencephalitis and 2 pyogenic abscess). By comparing the two post-contrast sequences, CE-FLAIR revealed greater enhancement in 38 cases (63.34%), equal enhancement in 17 cases (28.33%) and less enhancement in 5 cases (8.33%). For lesion conspicuity: good delineation observed in (61.67%), fair delineation in (25%) and no delineation in (13.33%). Lesion-to-background contrast ratio was statistically significant in CE-FLAIR with excellent inter-class correlation.
Conclusion
CE-FLAIR should be added in conjunction with or as a superior alternative to conventional CE-T1W sequence to optimize lesion detection and improve diagnostic reliability particularly in demyelinating and infectious lesions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Although T1-weighted sequence is typically used as the gold standard for post-contrast MRI examinations, contrast-enhanced FLAIR (CE-FLAIR) is increasingly used currently [1].
Contrast enhancement observed on FLAIR can be explained by the combined synergistic effects of T2 prolongation of various lesions and T1 shortening of gadolinium [2].
FLAIR images have an inherent T1-weighting component which allows for contrast enhancement. CE-FLAIR has been shown to be particularly sensitive in depiction of leptomeningeal enhancement, related to T1-shortening effect of gadolinium, slow-flowing superficial blood vessels and probably magnetization transfer effects [3].
A range of intracranial disorders have been studied using post-contrast FLAIR to improve the diagnostic sensitivity [4].
The aim of this study is to determine the added value of CE-FLAIR particularly in diagnosis and follow-up of demyelinating and infectious brain lesions and evaluate its usefulness in comparison with conventional CE-T1W images in clinical practice.
Methods
Subjects
This prospective study was approved by institutional research and ethical committee of Mansoura University and conducted between December 2018 and October 2020. The study group comprised of 60 patients who were referred from the neurology department to MRI unit of diagnostic radiology department at Mansoura university hospital (MUH). Written informed consent was obtained from subjects before MRI examinations.
Image acquisition
All MRI examinations were conducted using 1.5 Tesla device (Philips, Intera) with standard head coil and patient in supine position. Initially, conventional axial pre-contrast MRI sequences (fast spin echo (FSE) T1-weighted images, T2-weighted image, FLAIR, diffusion-weighted images (DWI) and apparent diffusion coefficient (ADC) were acquired.
Afterward, gadolinium-DTPA (Magnevist) was injected into the antecubital vein at a dose of 0.1 mmol/kg body weight. Post-contrast T1W images were obtained as the first post-contrast sequence about 1 min after contrast administration. Post-contrast T1W images were first acquired in the axial, sagittal and coronal planes. Then, axial or coronal post-contrast FLAIR images were consecutively acquired with nearly 3–4 min delay and with scanning parameters identical to pre-contrast ones.
All images were obtained with slice thickness of 5 mm, interslice gap of 1 mm and field of view 230 mm. Imaging parameters for pre- & post-contrast T1W images were: TR: 581 ms, TE: 15 ms and flip angle: 70 while those for pre- & post-contrast FLAIR were: TR: 11000 ms, TE: 110 ms and TI: 2800 ms.
Subtraction FLAIR images were obtained immediately after completing all examinations, at the technologist's workstation.
Image analysis
The resulting pool of scans was independently reviewed by two radiologists (M.G. and S.A.). Conventional sequences were initially interpreted as routine brain MRI examination to look for any obvious abnormalities. Then, the two radiologists reviewed pre- and post-contrast FLAIR alongside the corresponding subtraction images while staying blinded to the conventional CE-T1W images to identify any abnormal enhancement. Subsequently, both post-contrast sequences were compared simultaneously. Images were evaluated both qualitatively and quantitatively and correlated with clinical and laboratory data.
Qualitative evaluation includes detection of abnormal contrast enhancement, describing the location, pattern and degree of enhancement as well as the number of enhancing lesions in each sequence independently. The degree of enhancement was recorded as being either superior, equivocal or inferior. Lesion conspicuity refers to the ability to distinguish an enhancing lesion from normal adjacent brain tissue or from its initial high signal in pre-contrast FLAIR and was rated as either: no, fair or good delineation.
Quantitative estimation was performed by measuring the signal intensities which were obtained in the region of interest (ROI) by placing a cursor using customized co-registration software in both non-enhanced and contrast-enhanced T1W as well as FLAIR sequences and taking automated mathematical values. Signal of the corresponding lesions in pre-contrast FLAIR was considered as a baseline for determination of the degree of enhancement in CE-FLAIR.
Contrast enhancement index (CEI) was calculated using this formula: I* = I−I0 where I* is CEI, I is the lesion SI on CE-FLAIR, and I0 is the lesion SI on pre-contrast FLAIR. The average of two measurements was taken.
For pre- and post-contrast images of both T1W and FLAIR sequences, the lesion-to-background contrast ratio, defined as the difference between the lesion and background signal intensities divided by the background signal, was determined.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Corp. Released 2013. IBM SPSS Statistics for Windows, version 22.0. Armonk, NY: IBM Corp. Qualitative data were described using number and percentage. Quantitative data were described using the median for nonparametric data and the mean, standard deviation for parametric data using Kolmogorov–Smirnov test. P-value of equal to or less than 0.05 was considered significant.
Qualitative data, Monte Carlo simulation test was used as an alternative when the conditions for Chi-square test (more than 25% of cells with value less than 5) were not valid.
Quantitative data: nonparametric tests: Wilcoxon signed rank test was used to compare 2 independent groups.
The Spearman's rank-order correlation is used to determine the strength and direction of a linear relationship between two non-normally distributed continuous variables and / ordinal variables [5] .
Inter-class correlation was used to detect agreement between continuous variables with correlation coefficient > 0.7 was considered excellent agreement. The ICCs were classified using a system suggested by McGraw and Wong.
An inter-observer reliability analysis using the kappa statistics was performed to determine consistency among observers. Kappa agreement was calculated by cross-tabulation for categorical variables with Kappa (0.41–0.60: moderate, 0.61–0.80: substantial and 0.81–0.99: 0 perfect agreement).
Results
60 patients participated in this study, of whom 37 (61.67%) were females and 23 (38.33%) were males. Patients' ages ranged from 15 to 55, with a mean of roughly 38.32 ± 17.65.
Subjects were divided into two distinct groups based on the final imaging diagnosis: either demyelinating lesions comprised of 45 MS (multiple sclerosis) cases or infectious lesions that included 13 subjects with meningitis/meningoencephalitis and 2 subjects with abscess.
Qualitative assessment
As regards the degree of enhancement, qualitative comparison between CE-FLAIR and CE-T1WI by the second observer revealed that: superior enhancement in CE-FLAIR was noted in 38 cases, while equivocal enhancement was depicted in 17 cases. Less enhancement was described in 5 cases. As Table 1 shows, there is excellent agreement between the first and second observers with Kappa agreement (0.943) and percentage of agreement (96.73%).
Lesion conspicuity was described in three categories: good delineation was noted in most cases (n = 37, 61.67%), fair delineation in (n = 15, 25%) and no delineation in (n = 8, 13.33%) (Fig. 1).

Lesion conspicuity among studied cases
For subjects diagnosed with MS (n = 45), our results showed that 43 cases have positive enhancing lesions while two cases have no enhancing lesions at all. Table 2 illustrates the number of cases with positive or negative enhancement in each sequence. From our practice, it is noteworthy that all cases with active enhancing lesions were positive in CE-FLAIR, yet none of the cases showed positive enhancement in CE-T1WI only. In addition, excellent inter-observer reliability was noted with Kappa agreement (0.929) and percentage of agreement (97.5%).
Quantitative assessment
A statistically significant difference was found in the signal intensity of the lesion between pre- and post-contrast FLAIR images. Post-contrast FLAIR images showed higher median (765), ranging (from 345 to 3511). CEI (contrast enhancement index) described as the median difference between signal intensity in both pre- and post-contrast FLAIR was found to be 273, ranging (from 53 up to 1715). Furthermore, excellent interclass correlation was noted as shown in Table 3.
The lesion-to-background contrast ratio was found to be statistically higher in CE-FLAIR compared to non-contrast FLAIR, with higher median (0.96) ranging (from 0.23 to 3.04) found in CE-FLAIR. Also, this ratio was statistically significant with higher values in CE-FLAIR compared to CE-T1WI. (Summarized in Table 4).
Discussion
In the last decade, CE-FLAIR has emerged as a useful sequence to evaluate a wide range of pathologies. The nullification of CSF signal, inconspicuous vascular enhancement as compared to T1WI and some degree of T1 relaxation effect makes meningeal enhancement easily discernible on CE-FLAIR images [6].
Furthermore, CE-FLAIR has higher sensitivity for detection of low gadolinium concentrations than CE-T1WI [7]. This indicates that faintly enhancing lesions on CE-T1WI might be more clearly delineated on CE-FLAIR [8].
The primary objective of this study was to explore the diagnostic utility of CE-FLAIR particularly in the context of demyelinating and infectious brain lesions (Fig. 2).

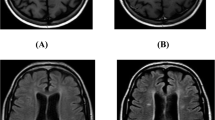
A 28-year-old female patient presented with fever, neck stiffness and altered mental status was diagnosed as viral meningoencephalitis. 1, 2, 3 rows: Axial cuts at same levels. (1) Non-contrast FLAIR images show abnormal high signal intensity at right caudate head (A) and medial aspects of both temporal lobes (B) with faint high signal at perimesencephalic cisterns (C). (2) Post-contrast FLAIR images revealed significant leptomenningeal enhancement (arrows) at both sylvian fissures (D) and perimesencephalic cisterns (E and F) as well as increased brightness of the right caudate head and medial temporal lobes as compared to corresponding pre-contrast images. (3) Post-contrast T1W images where minimal enhancement of perimesencephalic cisterns depicted in H, yet it would be confused with normal vascular enhancement. No significant abnormal enhancement noted in G and I.
A total of 60 subjects were enrolled in this study, they were classified based on diagnostic imaging findings and further correlated with both clinical and laboratory findings into two groups: firstly, demyelination group which included 45 subjects diagnosed with MS (75%) who were the majority of our participants. While the second group included 15 subjects with infectious lesions (25%): 13 cases with meningitis/meningoencephalitis and 2 cases with abscess.
In our evaluation of the degree of enhancement, qualitative comparison between CE-FLAIR and CE-T1WI revealed that obvious superior enhancement could be discerned in 63.34% (38 cases) on CE-FLAIR. On the other hand, 8.33% (5 cases) exhibited less enhancement on CE-FLAIR while equivocal enhancement was depicted in 28.33% (17 cases). These observations appear to be quite consistent with the results obtained by Athar et al. [9] where CE-FLAIR revealed better enhancement in 57.6% (19 subjects) and less enhancement in 18.2% (6 cases). However, in the remaining 24.2% (8 cases) both sequences were considered equivalent as they do not reveal any abnormality.
Moreover, our results showed excellent inter-observer agreement as regards the qualitative comparison of CE-FLAIR and CE-T1W sequences.
A glance at our results regarding the lesion conspicuity compared to those conducted by Athar et al. [9] clearly demonstrates that cases with good delineation tended to be higher in our study. Our observers were able to easily determine the clear outline of the enhancing lesion in CE-FLAIR in 61.67% of subjects compared to 39.4% reported in Athar's study. This could be relatively attributed to different sample sizes.
Most previous studies relied on the qualitative evaluation of lesion detection, which is necessarily observer dependent, few used a quantitative comparison. In concordance with previous studies by Zhou et al. [10] and Kim et al. [11], we have also used quantitative parameters to compare CE-FLAIR and CE-T1W sequences. Hence, we have tried to statistically prove our observations regarding the added potential merits of CE-FLAIR in order to avoid any bias or creating subjective data based merely on qualitative analysis.
Our measurements of the signal intensity revealed statistically significant difference (p < 0.001) between corresponding pre- and post-contrast FLAIR images. This confirmed positive enhancement.
In our study, CE-FLAIR significantly outperformed non-enhanced FLAIR and CE-T1W sequences in terms of the lesion-to-background contrast ratio (p 0.001). This enabled improved delineation of the enhancing lesions by CE-FLAIR images. The improved intrinsic soft tissue contrast resolution in FLAIR relative to T1W images may account for the higher contrast ratio reported by CE-FLAIR. Furthermore, CE-FLAIR images do not demonstrate enhancement of normal meninges and slow blood flow in superficial cortical vessels as do T1W images. Consequently, CE-FLAIR tends to provide higher detection rates and efficacy and allows better reliability in identification and distinction of sulcal or meningeal pathologies.
In the study by Kim et al. [11], higher lesion-to-background contrast ratio has been observed on CE-FLAIR compared to CE-T1W images. These findings are typically in line with our results. Furthermore, Zhou et al. [10] reported that the contrast enhancement ratio on post-contrast T1WI was considerably higher while gray-white matter contrast was lower (p = 0.02) in comparison with post-contrast FLAIR.
In a study conducted by Azad et al. [12], by comparing the net meningeal enhancement on CE-FLAIR to the T1W fat saturation sequence, a statistically significant difference was observed (p < 0.001). These results are conformed to the data obtained by our study.
MRI has been incorporated into the McDonald criteria as an indispensable tool in the diagnosis of MS [13]. Gadolinium-based MRI is regarded as the best indicator of disease activity and response to therapy [14,15]. As active MS lesions are associated with focal disruption of blood brain barrier due to perivascular inflammation, injection of contrast leads to significant shortening of T1 relaxation time of these lesions with subsequent increased signal intensity [16]. Previous studies indicated that injection of gadolinium can intensify T1 effect on FLAIR leading to increased signal intensity of lesions in this sequence [17]. To our knowledge, few studies have evaluated the role of CE-FLAIR in detecting enhancing brain lesions in MS patients.
Out of our observations of 45 subjects with MS, 43 cases showed active enhancing lesions on CE-FLAIR (Fig. 3), 36 of them revealed enhancement on CE-FLAIR only and 7 had positive enhancing lesions on both CE-FLAIR and CE-T1W sequences. Since we aimed at exploring the ability of CE-FLAIR to add diagnostic information about the number, size, location and degree of enhancement of MS lesions compared to the conventional CE-T1W images, image analysis encompasses both qualitative and quantitative methods as well as subtraction imaging. In initial qualitative assessment, lesions subjectively perceived to be of considerably higher signal intensity in post-contrast FLAIR images compared to corresponding pre-contrast ones were described as ultrabright and considered as having positive enhancement. This indicates that the signal of the corresponding lesions in pre-contrast FLAIR was assumed as a baseline for determination of the degree of enhancement. But to others, this may seem to reflect the subjective nature of visual identification of ultrabright lesions particularly due to the fact that MS lesions basically demonstrate initial high signal in non-enhanced FLAIR. Consequently, our observers reviewed and compared these lesions with the signal intensity quantification approach through measuring signal intensity of MS lesions in both pre- and post-contrast FLAIR sequences (Fig. 4). In addition, lesions of outstanding brightness were easily identified and confirmed using subtraction images. Our findings were supported by clinical data.

A 32-year-old female patient with history of MS, follow-up MRI is requested as active disease is clinically suspected. Each row is composed of images at the same level. A and B: axial pre-contrast FLAIR shows multiple high signal intensity plaques seen at periventricular white matter (A) as well as centrum semiovale and subcortical white matter of both cerebral hemispheres (B). C and D: axial post-contrast FLAIR where plaques appear more bright (yellow arrows) and the left subcortical lesion in D becomes more clearly demonstrated and even larger in size (red arrow). E and F: Subtraction FLAIR images confirmed the enhancement of the lesions (arrows). G and H: axial post-contrast T1WI: no definite enhancing lesions could be detected

A 31-year-old female patient presented by numbness, weakness and fatigue. A Coronal pre-contrast FLAIR shows: few foci of high signal intensity at subcortical and periventricular white matter. B Coronal post-contrast FLAIR shows nodular enhancement at two lesions (arrows) which appear ultrabright than in A, with the lesion at right temporal lobe not visualized in post-contrast T1WI (E). C and D Coronal pre- and post-contrast FLAIR at the same level as A and B with measurements of the signal intensity shown, denoting the difference between pre- and post-contrast images and confirming presence of enhancement. E Coronal post-contrast T1WI shows subtle non-clearly demonstrated incomplete ring enhancement of the left periventricular lesion in comparison with B. Diagnosis: MS with radiological signs of activity
It was worthy of attention that CE-FLAIR provided better detection rates and a higher number of acute enhancing MS plaques in the supra-tentorial region compared to contrast-enhanced T1W sequence which is the gold standard sequence. In addition, we noticed that CE-FLAIR could depict enhancing MS lesions with greater conspicuity and remarkable degree of enhancement than early CE-T1WI. These observations were in concordance with the findings of prior studies done by Abdolmohammadi et al. [18] and Bagheri et al. [16]. Furthermore, subtraction images aided in reducing false positive results, reduced interpretation time and improved detection accuracy of very small and even faintly enhancing lesions, this was consistent with the findings of the research conducted by Zivadinov et al. [19]. Also, the quantitative approach proved to more reliably predict the enhancement compared with visual identification of ultrabright lesions in clinical practice.
From our practice, it is interesting to note that 36 out of 43 MS subjects with active enhancing lesions demonstrated positive enhancement only on CE-FLAIR without any evidence of enhancement on CE-T1W images. Even if there is only one enhancing lesion, it will indicate active disease and will result in a relevant change in clinical management and modulating therapy. A similar finding was observed by Bagheri et al. [16] but in a lower number of participants. Hence, the most important conclusion to emerge from the analysis of our MS cases is that CE-FLAIR should be incorporated as a routine imaging sequence in evaluation of MS patients particularly if despite clinically suspected active disease, no enhanced lesion is found in routine CE-T1WI. Therefore, it could serve as a promising imaging marker for prediction of ongoing disease activity that could subsequently affect management and clinical care.
On the light of our analysis of 15 cases diagnosed with CNS infection, we noticed that the diagnostic superiority of CE-FLAIR in terms of detection of leptomeningeal enhancement was particularly striking. Moreover, CE-FLAIR exhibited better wall enhancement with greater mural thickness and more distinct and sharper delineation from the surroundings in two subjects diagnosed with pyogenic abscess (Fig. 5). Overall, our results postulated that CE-FLAIR depicted superior enhancement as well as valuable diagnostic findings in comparison with conventional CE-T1WI in infectious brain lesions. These results were equivalent to the studies done by Ahmed [20] and Rastogi and Jain [21] who supported the fact that CE-FLAIR has insignificant vascular enhancement relative to meningeal enhancement, making it easier to detect meningeal inflammation and improving diagnostic precision in cases of early meningitis, which is essential for better patient care and favorable outcome. The signal from slow-flowing vessels is suppressed on FLAIR due to lack of inflow enhancement. Thus, it offers a distinct advantage in overcoming the limitations of T1WI and any appreciable linear enhancement in the cortical sulci is likely due to enhanced meninges rather than adjacent enhanced vessels[6]. Reviewing results of multiple researchers confirmed that CE-FLAIR confers greater reliability in early detection of leptomeningeal infection compared to conventional CE-T1W sequence (Fig. 6) which has some limitations that makes early diagnosis of meningitis a major challenge in some cases.

A 14-year-old boy presented with acute fever, ataxia and dizziness with history of mastoiditis was diagnosed as right cerebellar abscess. A axial pre-contrast FLAIR shows: a well circumscribed right cerebellar hemisphere lesion with central intermediate signal intensity of its content and high signal intensity of the surrounding mild vasogenic edema. B Axial post-contrast FLAIR shows: thicker walled and more bright ring enhancement of the lesion (more marked at its medial aspect) than in post-contrast T1WI (B). Also it is clearly delineated from the background edema. C axial pre-contrast T1WI shows: a well-defined right cerebellar hemisphere lesion with low signal intensity of the internal content. D axial post-contrast T1WI shows thin smooth ring enhancement of the lesion. E axial subtraction FLAIR image. F axial DWI showing restricted content of the right cerebellar lesion

A 25-year-old male presented by acute fever, headache, vomiting and neck stiffness was diagnosed as tuberculous meningitis. A axial pre-contrast FLAIR: shows minimal sulcal hyperintensity. B axial CE-FLAIR: depicts pronounced leptomeningeal enhancement around basal cisterns, with additional thin sheet of dural enhancement. C axial pre-contrast T1WI. D axial CE-T1WI: shows subtle sulcal & leptomeningeal enhancement around basal cisterns not appreciated as in B and could be easily confused with normal vascular enhancement
Our study has some limitations, firstly: the sample size is comparatively moderate. Secondly, CE-FLAIR was acquired as the second post-contrast sequence. An alternating randomized order of the two post-contrast sequences is advised in future studies to prevent any bias that may be related to potentially increased enhancement with increased duration after contrast injection. However, since CE-FLAIR is more sensitive to even small concentration of gadolinium, our results would have been even better if CE-FLAIR was firstly acquired. Although subtraction images were highly informative, they may be amenable to patient motion or CSF pulsation artifacts which were encountered in few cases. Hence, correlation with quantitative approach was of utmost significance to avoid any misleading signal.
Despite these limitations, our results provide important new insight into the emerging role of CE-FLAIR in early diagnosis and follow-up of demyelinating and infectious lesions.
Conclusions
CE-FLAIR provides better enhancement and improved contrast-to-background resolution as well as superior lesion detection capabilities in comparison with routine CE-T1W sequence. We emphasize that it offers additional diagnostic data that would directly contribute to early diagnosis and better management. Hence, it should be integrated as a clinically valuable and reliable imaging marker in all brain MRI examinations particularly in the context of demyelination and infection.
Availability of data and materials
The authors confirm that all data supporting the finding of the study are available within the article, and the raw data and data supporting the findings were generated and available on reasonable request from the corresponding author.
Abbreviations
- CE-FLAIR:
-
Contrast-enhanced FLAIR
- ROI:
-
Region of interest
- CEI:
-
Contrast enhancement index
- MS:
-
Multiple sclerosis
References
Fukuoka H, Hirai T, Okuda T et al (2010) Comparison of the added value of contrast-enhanced 3D fluid-attenuated inversion recovery and magnetization-prepared rapid acquisition of gradient echo sequences in relation to conventional postcontrast T1-weighted images for the evaluation of leptomening. Am J Neuroradiol 31(5):868–873. https://doi.org/10.3174/ajnr.A1937
Kim SC, Park SW, Ryoo I, Jung SC, Yun TJ (2014) Contrast-enhanced FLAIR (Fluid-Attenuated Inversion Recovery) for evaluating mild traumatic brain injury. PLoS ONE 9(7):102229. https://doi.org/10.1371/journal.pone.0102229
McKinney A, Palmer C, Short J, Lucato L, Truwit C (2006) Utility of fat-suppressed FLAIR and subtraction imaging in detecting meningeal abnormalities. Neuroradiology 48(12):881–885. https://doi.org/10.1007/s00234-006-0145-5
Dickinson PJ, Jones-Woods S, Cissell DD (2018) Abrogation of fluid suppression in intracranial postcontrast fluid-attenuated inversion recovery magnetic resonance imaging: A clinical and phantom study. Veterinary Radiology and Ultrasound 59(4):432–443. https://doi.org/10.1111/vru.12605
Watanabe H (2011) Applications of Statistics to Medical Science (1) Fundamental Concepts. J Nippon Med Sch 78(5):274–279. https://doi.org/10.1272/jnms.78.274
Ahmad A, Azad S, Azad R (2015) Differentiation of leptomeningeal and vascular enhancement on post-contrast FLAIR MRI sequence: role in early detection of infectious meningitis. J Clin Diagn Res 9(1):TC08-TC12. https://doi.org/10.7860/JCDR/2015/11519.5387
Park YW, Ahn SJ (2018) Comparison of contrast-enhanced T2 FLAIR and 3D T1 black-blood fast spin-echo for detection of leptomeningeal metastases. Invest Magn Reson Imaging 22(2):86. https://doi.org/10.13104/imri.2018.22.2.86
Lee EK, Lee EJ, Kim S, Lee YS (2016) Importance of contrast-enhanced fluid-attenuated inversion recovery magnetic resonance imaging in various intracranial pathologic conditions. Korean J Radiol 17(1):127–141. https://doi.org/10.3348/kjr.2016.17.1.127
Athar I, Khan SALI, Butt MA et al (2019) Comparison between post contrast T1 weighted and T2 weighted flair axial sequences in various intracranial pathologies. Int J Sci Eng Res 10(December):872–883
Zhou ZR, Shen TZ, Chen XR, Peng WJ (2006) Diagnostic value of contrast-enhanced fluid-attenuated inversion-recovery MRI for intracranial tumors in comparison with post-contrast T1W spin-echo MRI. Chin Med J 119(6):467–473
Kim JH, Yi KS, Choi CH, Woo ST, Cha SH (2018) Does multiphasic contrast enhanced fluid attenuated inversion recovery magnetic resonance imaging enhance the detectability of small intracerebral metastases? J Korean Soc Radiol 78(3):179. https://doi.org/10.3348/jksr.2018.78.3.179
Azad R, Tayal M, Azad S, Sharma G, Srivastava RK (2017) Qualitative and quantitative comparison of contrast-enhanced fluid-attenuated inversion recovery, magnetization transfer spin echo, and fat-saturation T1-weighted sequences in infectious meningitis. Korean J Radiol 18(6):973–982. https://doi.org/10.3348/kjr.2017.18.6.973
Suthiphosuwan S, Kim D, Bharatha A, Oh J (2017) Imaging markers for monitoring disease activity in multiple sclerosis. Curr Treat Options Neurol 19:18. https://doi.org/10.1007/s11940-017-0453-6
McDonald WI, Compston A, Edan G et al (2001) Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Ann Neurol 50(1):121–127. https://doi.org/10.1002/ana.1032
Miller DH, Filippi M, Fazekas F et al (2004) Role of magnetic resonance imaging within diagnostic criteria for multiple sclerosis. Ann Neurol 56(2):273–278. https://doi.org/10.1002/ana.20156
Bagheri MH, Meshksar A, Nabavizadeh SA, Borhani-Haghighi A, Ashjazadeh N, Nikseresht AR (2008) Diagnostic value of contrast-enhanced fluid-attenuated inversion-recovery and delayed contrast-enhanced brain MRI in multiple sclerosis. Acad Radiol 15(1):15–23. https://doi.org/10.1016/J.ACRA.2007.07.022
Goo HW, Choi CG (2003) Post-contrast FLAIR MR imaging of the brain in children: Normal and abnormal intracranial enhancement. Pediatr Radiol 33(12):843–849. https://doi.org/10.1007/s00247-003-1057-8
Abdolmohammadi J, Pourasl M, Zandkarimi M (2017) Evaluation the sensitivity of FLAIR and DWI post-inject comparison with delay enhance T1w in detection of active MS lesions. Eur Congr Radiol. https://doi.org/10.1594/ecr2017/C-2793
Zivadinov R, Ramasamy DP, Hagemeier J et al (2018) Evaluation of leptomeningeal contrast enhancement using pre-and postcontrast subtraction 3D-FLAIR imaging in multiple sclerosis. Am J Neuroradiol 39(4):642–647. https://doi.org/10.3174/ajnr.A5541
Ahmed M (2018) Comparison of gadolinium based T1 weighted and flair Mr sequences for the assessment of leptomeningeal enhancement in meningoencephalitis. Int J Radiol 5(1):163–171. https://doi.org/10.17554/j.issn.2313-3406.2018.05.49
Rastogi R, Jain S (2016) Can postcontrast-T2FLAIR be a boon over postcontrast-T1GRE images in MR brain imaging? J Neuroinfectious Dis. https://doi.org/10.4172/2314-7326.1000219
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
MG suggested the research idea, ensured the original figures, collected data in all stages of manuscript and performed image analysis and comparison. SA contributed to evaluation of radiological findings and revised the results. LG supervised the study with significant contribution to manuscript revision. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the institutional research and ethical committee at Faculty of Medicine, Mansoura University. Informed written consents were obtained from all subjects.
Consent for publication
All participants included in the research gave written consent to publish the data obtained in this study. The authors agreed to publish the paper.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gad, M., Elsorogy, L.G. & Moustafa, S.A.F. Diagnostic utility of contrast-enhanced FLAIR MRI in imaging of demyelinating and infectious brain lesions. Egypt J Radiol Nucl Med 54, 104 (2023). https://doi.org/10.1186/s43055-023-01049-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01049-2