
Abstract
Background
Decompensated liver disease (DCLD) has high mortality, and its prediction is important to prognosticate and prioritize patients for liver transplantation. MELD, MELD variants, and CTP were widely tested for mortality prediction with few drawbacks. The aim of the study is to propose a new prognostic model for DCLD which is better than the existing scores.
Materials and methods
Retrospective study with 321 DCLD patients were enrolled. Patient relatives were telephonically contacted regarding date of death, and mortality at 3 months was assessed. Logistic regression was done, coefficient of beta of independent variables were found out, and a new CHIBA score was proposed.
CHIBA score = creatinine × 0.6 + HE × 0.4+ INR × 0.8 + bilirubin × 0.125 + ascites × 1.2) where C stands for creatinine, H for hepatic encephalopathy, I for INR, B for bilirubin, and A for ascites.
Results
CHIBA score has AUROC of 0.793 (at a cutoff of > 5.5, it has a sensitivity of 66% and specificity of 76%) compared to MELD-Na of 0.735 (cutoff > 25, sensitivity 65%, and specificity 72%); MELD of 0.727 (cutoff > 17 sensitivity of 80.37% and specificity of 55.14%); I-MELD of 0.72; MESO index of 0.72; and UKELD of 0.686. For validation, 214 patients were selected, and AUROC of CHIBA score in the validation cohort was 0.77. At a cutoff of > 5.5, it has a sensitivity of 60% and specificity of 77%.
Conclusion
CHIBA score is superior to MELD and MELD variants in predicting 3-month mortality, and it is validated in an external cohort. It can be calculated at bedside as it is a simple score with no logarithmic variables in it.
Similar content being viewed by others
Introduction
Decompensated liver disease (DCLD) is one of the most common cause of mortality worldwide, though the etiology varies from place to place. With emergence of NAFLD, the incidence of DCLD is increasing at an alarming rate. Though many therapies for DCLD had been tried, most of them were not able to provide a curative therapy. Liver transplantation is the only curative therapy for DCLD. Because of scarcity of cadaveric donors, identification of most suitable recipients who requires the transplantation is at most important. Many studies have investigated factors predicting survival in patients with cirrhosis [1, 2]. Many scoring systems were proposed for better allocation of organ for transplantation and to decrease the mortality in transplant waiting list. Among them, the most important was MELD and MELD variants. MELD was introduced by Malinchoc for TIPSS patients [3]. But later, it was found to be effective for allocating organs for transplantation candidates based on MELD score [4, 5]. The problem with MELD is that creatinine (one component of MELD) may vary according to muscle mass, and its levels in females were less compared to males leading to increased mortality of females in transplantation list. Another drawback of MELD is that it gives maximum weightage for INR which vary with time to time even in same patient. Drawback also includes MELD exceptions like HCC for which mortality cannot be accurately predicted with MELD. To overcome these drawbacks of MELD, various modifications were put forward, and the most important among this was MELD-Na [6, 7]. MELD and its variants are complicated scores with logarithmic variables in it, and it is not able to calculate at bedside. Another predictor model of mortality in CLD patients was CTP score [8]. The problem with CTP score was that it is a subjective score, and that it is not a dynamic score like MELD and does not rate other factors such as renal and pulmonary dysfunction [9, 10] which are common in decompensated cirrhosis.
Numerous studies compared MELD and CTP regarding prediction of 3- and 6-month mortality with varying results. In this study, we compared CTP, MELD, and MELD variants like MELD-Na, UKLED, I-MELD, and MESO score in a cohort of DCLD in predicting 3-month mortality and proposed a new score which can predict mortality better than the existing scores (Table 1).
Materials and methods
It was a retrospective study in a population of DCLD patients with age more than 18 years admitted in Department of Medical Gastroenterology, Trivandrum Medical College, from June 2016-January 2019 after excluding patients with hepatocellular carcinoma, extrahepatic malignancy, and high DF alcoholic hepatitis and patients who died in the same admission.
The study was approved by the Institutional Ethics Review Board of the Hospital, and informed written consent was provided by all patients. Data is collected from the electronically generated discharge summary and telephonic conversation. Clinical and biochemical parameters were collected on the date of admission. Ascites was evaluated clinically and with ultrasound or CT. Hepatic encephalopathy was evaluated clinically at the time of the assessment and using the electronic records and were classified according to the West Haven criteria (grades 1–4). Patient’s bystanders were telephonically contacted regarding mortality at 3 months from the time of admission, and death time from date of admission was assessed. Based on admission variables, MELD, CTP, and MELD variants were calculated. Logistic regression of significant variables was done, and a new score (CHIBA score) was proposed (CHIBA score = creatinine × 0.6 + HE × 0.4 + INR × 0.8 + bilirubin × 0.125 + ascites × 1.2). C stands for creatinine, H for hepatic encephalopathy, I for INR, B for bilirubin, and A for ascites. Ascites was further divided into absent or mild with a score of 0, moderate −1, and tense 2. Hepatic encephalopathy is absent with score of 0, grade 1 West Haven score of 1, grade 2 score of 2, and grades 3 and 4 a score of 3. For validation of the CHIBA score, 214 patients were taken which was comparable to the test cohort. AUROC of CHIBA score in the validation cohort was found out.
Statistical analysis
Continuous variables were compared using Student’s t-tests, and categorical variables were compared using chi-squared tests or Fisher’s tests. The predictive ability for each model was evaluated according to areas under receiver-operating characteristics curves (AUROC). Comparisons of AUROCs were performed by MedCalc software version 12.4. The p-value was considered significant when it was less than 0.05.
Results
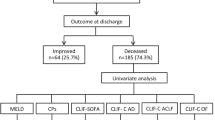
Three-hundred twenty-one patients were taken up for the study (Fig. 1). For validation, 214 patients were taken. Baseline characteristics of the test group and validation cohort were given in Table 2.

Consort diagram of the test group
Among the quantitative study variables analyzed by t-test hemoglobin, platelet count, albumin, creatinine, bilirubin, sodium level, INR, portal vein diameter, liver span, and spleen span were statistically significant in predicting 3-month mortality (Table 3).
Among the qualitative variables analyzed by chi-square test, hepatic encephalopathy and ascites were significant in predicting 3-month mortality (Table 4).
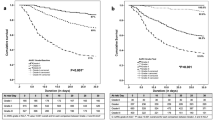
AUROC was plotted in comparing CTP, MELD, and MELD variants in predicting 3-month mortality. In predicting 3-month mortality, the AUROC of CTP was 0.769; Child was (as our study was on DCLD, only Child B and C were taken) 0.659; MELD was 0.727; MELD-Na was 0.735; I-MELD was 0.723; MESO was 0.727; and UKLED was 0.686 (Table 5 and Fig. 2).

AUROC of new score
CTP had maximum AUROC in predicting 3-month mortality (0.767, cutoff of > 11 with sensitivity of 71% and specificity of 73.8%) followed by MELD-Na (0.735, cutoff of > 25 with sensitivity of 65% and specificity of 72%).
Logistic regression analysis of significant variables was done, and new score (CHIBA score) was proposed (Table 6).
CHIBA score = creatinine × 0.6 + HE × 0.4 + INR × 0.8 + bilirubin × 0.125 + ascites × 1.2. C stands for creatinine, H for hepatic encephalopathy, I for INR, B for bilirubin, and A for ascites. Ascites was further divided into absent or mild with a score of 0, moderate −1, and tense 2. Hepatic encephalopathy is absent with score of 0, grade 1 West Haven score of 1, grade 2 score of 2, and grades 3 and 4 a score of 3.
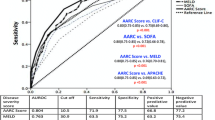
It had AUROC of 0.793 (at a cutoff of ≥ 5.5, it has sensitivity of 66% and specificity of 76) (Fig. 2).
Validation of new score
The sample size for the validation cohort was calculated by the formula 4PQ/D2/prevalence.
P is sensitivity, Q is 1-P, and D is 20% of P. Death at 3 months was 33%. The sample size was calculated to be 156. For validation, 214 patients were taken, and the baseline characteristics of the validation cohort are shown in Table 2. It was comparable to the test cohort. AUROC of CHIBA score in the validation cohort was 0.77. At a cutoff of > 5.5, it has a sensitivity of 60% and specificity of 77% (Fig. 3, Table 7).

AUROC of validation cohort
Discussion
There is need for precise prognostic indicators for survival of DCLD patients which is important to guide clinical decision. The MELD score has been used as a prognostic tool for patients with DCLD and found to be beneficial in predicting 3- and 12-month survival of DCLD patients. However, MELD score has shown less prognostic accuracy as compared with the CTP score [11]. Though there are comparison studies between CTP, MELD, and MELD variants even in the Indian population, a study comparing almost every validated MELD variants, MELD, and CTP are very few in the literature. Another aim of this study was to propose a new score that can predict mortality better than the existing models in the Indian population.
Data from our study showed that the presence of ascites and hepatic encephalopathy was significant in predicting 3-month mortality. Hepatic encephalopathy, which denotes excessive portosystemic shunting, was also a significant factor of 3-month mortality in our study which is comparable to previous studies [12, 13].
CTP had maximum AUROC in predicting 3-month mortality (0.767, cutoff of > 11 with a sensitivity of 71% and specificity of 73.8%) followed by MELD-Na (0.735, cutoff of > 25 with a sensitivity of 65% and specificity of 72%). CTP was found to have an important prognostic factor for DCLD patients [14,15,16], and hence, CTP score with many subjective components is still a very important prognostic marker in DCLD which is proved by our study. Our results confirmed that the predictive power of the standard MELD can be augmented by addition of sodium, as demonstrated higher AUCs for MELD-Na, MESO index, and I-MELD which are in agreement with the study by Biselli et al. [17]. The problem with MELD score is that it has logarithmic variables, and its calculation is not possible at the bedside. Variants like MESO and I-MELD were derived from MELD which makes these scores unsuitable for bedside calculations. CHIBA score is simple, and its derivation involves only simple calculation, and hence, it is easy to calculate CHIBA score at bedside. Moreover, CHIBA score has ascites and hepatic encephalopathy as its components. One of the drawbacks of the MELD is that it is not able to predict mortality accurately in those with ascites, and this was partially overcome with the advent of MELD-Na. Ascites and hepatic encephalopathy likely to increase the predictive power of CHIBA over MELD, and MELD variants as later were shown to be less effective in these situations. Besides, although iMELD had the highest AUC by incorporating age and Na to raise their prognostic ability, it did not reveal significant superiority to other MELD-based systems.
New CHIBA score has an AUROC of 0.793 (at a cutoff of > 5.5, sensitivity 66%, and specificity 76%) better than all other predictor models. A study by Zou et al. [18] evaluated the inhospital mortality in relation to ALBI, CTP, and MELD scores in 631 cirrhotic patients and found that the albumin-bilirubin (ALBI) score had the best AUC (0.808, 0.785, 0.787, respectively). The new CHIBA score was validated in an external cohort with a sample size of 214. AUROC of CHIBA score in the validation cohort was 0.77 which is better than previous studies [19, 20]. At a cutoff of > 5.5, it has a sensitivity of 60% and specificity of 77% in predicting 3-month mortality. Our results showed excellent reproducibility, suggesting that new CHIBA score is generalizable to patients with similar conditions from different regions. The CHIBA score can be easily calculated from routine physical examination and laboratory testing and is thus available even in lower resource settings. Although the study results were encouraging, this study still had potential limitations. As this study is a retrospective study, further refinement should be pursued to validate this score by prospective studies.
Conclusion
CHIBA score is superior to MELD and MELD variants in predicting 3-month mortality, and it is validated in an external cohort. It can be calculated at the bedside and does not require mobile applications as it is a simple score with no logarithmic variables and better than all existing prognostic models for DCLD.
Availability of data and materials
Yes
References
Huo TI, Lin HC, Wu JC et al (2005) Different model for end-stage liver disease score block distributions may have a variable ability for outcome prediction. Transplantation 80:1414–1418
Christensen E (2004) Prognostic models including the Child–Pugh, MELD and Mayo risk scores: where are we and where should we go? J Hepatology. 41:344–350
Malinchoc M, Kamath PS, Gordon FD et al (2000) A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 31(864–71):2
Bernardi M, Gitto S, Biselli M (2011) The MELD score in patients awaiting liver transplant: strengths and weaknesses. J Hepatology 54:1297–1306
Magder LS, Regev A, Mindikoglu AL (2012) Comparison of seven liver allocation models with respect to lives saved among patients on the liver transplant waiting list. Transpl Int 25:409–415
Huo TI, Wang YW, Yang YY et al (2007) Model for end-stage liver disease score to serum sodium ratio index as a prognostic predictor and its correlation with portal pressure in patients with liver cirrhosis. Liver Int 27:498
Kim WR, Biggins SW, Kremers WK et al (2008) Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med 359:1018
Oellerich M, Burdelski M, Lautz HU et al (1991) Assessment of pre-transplant prognosis in patients with cirrhosis. Transplantation 51:801–806
Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R (1973) Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 60:646–649
Castera L, Pauwels A, Levy VG (1996) Prognostic indicators in patients with liver cirrhosis admitted to an intensive care unit. Gastroenterol Clin Biol. 20:263–268
Kamath PS, Wiesner RH, Malinchoc M et al (2001) A model to predict survival in patients with end-stage liver disease. Hepatology 33:464–470
Del Olmo JA, Pena A, Serra MA, Wassel AH, Benages A, Rodrigo JM (2000) Predictors of morbidity and mortality after the first episode of upper gastrointestinal bleeding in liver cirrhosis. J Hepatol 32:19–24
Cooper GS, Bellamy P, Dawson NV, Desbiens N, Fulkerson WJ Jr, Goldman L et al (1997) A prognostic model for patients with end-stage liver disease. Gastroenterology 113:1278–1288
Wu SL, Zheng YX, Tian ZW et al (2018) Scoring systems for prediction of mortality in decompensated liver cirrhosis: a meta-analysis of test accuracy. World J Clin Cases 6:995–1006
Ying L, Jing Z, Zhongfeng W (2017) Prognostic factors for patients with hepatitis B virus-related acute-on-chronic liver failure. Linchuang Gandanbing Zazhi 33:497–501
D’Amico G, Garcia-Tsao G, Pagliaro L (2016) Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol 44:217–231
Biselli M, Gitto S, Gramenzi A et al (2010) Six score systems to evaluate candidates with advanced cirrhosis for orthotopic liver transplant: which is the winner? Liver Transplantation 16:964
Zou D, Qi X, Zhu C et al (2016) Albumin-bilirubin score for predicting the in-hospital mortality of acute upper gastrointestinal bleeding in liver cirrhosis: a retrospective study. Turk J Gastroenterol 27:180–181
Huo TI, Lin HC, Huo SC, Lee PC, Wu JC, Lee FY et al (2008) Comparison of four model for end-stage liver disease-based prognostic systems for cirrhosis. Liver Transpl 14:837–844
Koo JK, Kim JH, Choi YJ, Lee CI, Yang JH, Yoon HY et al (2013) Predictive value of refit model for end-stage liver disease, refit model for end- stage liver disease, and pre-existing scoring system for 3-month mortality in Korean patients with cirrhosis. J Gastroenterol Hepatol 28:1209–1216
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Dr. SA, first and corresponding author; made substantial contributions to the conception and design of the work, acquisition, analysis, and interpretation of data; and also have drafted the work after revising it. Dr. JV, co-author and helped in analysis of results and data collection. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Ethics Review Board of the Hospital, and informed written consent was provided by all patients.
Consent for publication
Given by all authors
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sathar, S.A., Vargheese, J. CHIBA score: a novel model for predicting 3-month mortality in a cohort of Decompensated Liver Disease (DCLD). Egypt Liver Journal 13, 13 (2023). https://doi.org/10.1186/s43066-023-00243-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-023-00243-1