
Abstract
Background
The aim of the study was to investigate the association of neutrophil-to-lymphocyte (NLR) and platelet-to-lymphocyte ratios (PLR) with standard inflammation parameters, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), complement component C3, anti-double-stranded deoxyribonucleic acid (anti-dsDNA), anti-nucleosome and anti-C1q antibodies, and serum and urinary monocyte-chemoattractant protein-1 (MCP-1) with disease activity in patients with systemic lupus erythematosus (SLE).
Results
This study included 160 patients (145 female and 15 male patients), hospitalized at the Rheumatology Department. A positive correlation between NLR and ESR (p < 0.01), anti-dsDNA antibodies (p < 0.05), and PLR (p < 0.001) was obtained, with a negative correlation with C3 (p < 0.005). PLR shows a positive correlation with ESR (p < 0.001), CRP (p < 0.005), anti-dsDNA antibodies (p < 0.001), anti-nucleosome antibodies (p < 0.05), and urine MCP-1 (p < 0.05), with a negative correlation with C3 (p < 0.005). Univariate analysis showed that all the examined laboratory parameters were independent predictors of disease activity (p < 0.001), while the method of standard multiple regression analysis revealed the most significant ESR and serum MCP-1 (p < 0.05).
Conclusions
NLR and PLR, as inexpensive and accessible biomarkers, can help in routine clinical practice for the estimation of disease activity in SLE patients.
Similar content being viewed by others

Background
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease, affecting the immune complexes and generating numerous proinflammatory cytokines which influence individual cells of the hematopoietic system and the clinical picture [1]. In recent years, thrombocytes, in addition to leukocytes and lymphocytes, have attracted much attention regarding their role in the creation and maintenance of systemic inflammation [2, 3]. Chronic systemic inflammation in immune-mediated diseases, including SLE, is accompanied by the activation of thrombocytes and neutrophils, with the consequential appearance of thrombo-inflammatory lesions, vascular injuries, and organ damage. Thrombocyte activation has an impact on the creation of heterotropic aggregations with neutrophils (in giant cell arteritis) or the activation of neutrophils with neutrophil extracellular traps creation in SLE, small-vessel vasculitis, rheumatoid arthritis, and systemic sclerosis [4]. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are used as standard systemic inflammation markers in autoimmune diseases.
Recently, however, more evidence has been gathered about the potential clinical significance of the analysis of hematological parameters such as neutrophil-to-lymphocyte (NLR) and platelet-to-lymphocyte ratios (PLR), primarily due to their low cost and wide availability for many diseases [5,6,7]. Traditional SLE markers, such as anti-double-stranded deoxyribonucleic acid (anti-dsDNA) antibodies and complement, are not sensitive enough to disease activity changes and cannot predict disease relapses; that is the reason why the search for new non-invasive and easily measurable markers is still underway [8, 9]. It is believed that the lack of reliable and specific biomarkers hampers the discovery of more successful therapeutic modalities, with the assumption that we need a panel of biomarkers useful in SLE diagnosis, disease activity monitoring, prediction of relapse, and assessment of treatment effectivity [10, 11].
The aim of the study was to examine the correlation of NLR and PLR with inflammation parameters including ESR and CRP, complement component C3, anti-dsDNA, anti-nucleosome, anti-C1q antibodies, and additionally with serum and urinary monocyte-chemoattractant protein-1 (MCP-1) in SLE patients. We also wanted to assess the significance of all these parameters as potential disease activity biomarkers in patients with SLE.
Materials
This study included 160 SLE patients (145 women and 15 men), hospitalized at the Rheumatology Department from January to June 2022 as a single-center cross-sectional study. The patients’ diagnosis was made according to the 1997 revision of the American College of Rheumatology Criteria [12]. The patients with primarily hematological disorders with anemia, leukopenia, and thrombocytopenia, as well as those with signs of infection or diabetes, were excluded from the study. Patients were treated according to the recommended therapy for SLE patients including corticosteroid therapy, hydroxychloroquine, azathioprine, mycophenolate mofetil, and pulse doses of cyclophosphamide in accordance with disease activity and involvement of vital organs as previously reported [1].
The degree of disease activity was evaluated in all the patients using the previously recommended Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and by physician global assessment. The degree of organ damage was assessed using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index previously reported and described as SDI [13, 14].
The biochemical parameters and cytokine determination were performed in the Research Center for Biomedicine. ESR is determined manually, by measuring the rate of sedimentation to the bottom of the test tube; CRP was quantitatively determined using a biochemical analyzer (BA400, Spain), while blood counts and leukocyte counts were determined using a hematological analyzer (Sysmex XS1000i, Japan). NLR and PLR were calculated by dividing the absolute number of individual cell populations as previously reported [5, 7].
Anti-dsDNA, anti-nucleosome, and anti-C1q antibodies were determined using the standard sandwich ELISA method. Serum and urine MCP-1 was determined according to the manufacturer’s instructions (R&D Systems, Inc., Minneapolis, USA) using an ELISA reader (Alegria, Orgentec, Germany) as previously described [15]. All analyzed hematological parameters, autoantibodies, and cytokines were analyzed simultaneously in the examined patients.
Statistical analysis
Statistical calculations were performed using the SPSS 20 software package. The descriptive statistical analysis included the classical statistical parameters: arithmetic mean, standard deviation, interval variation (min–max), absolute frequency (n), and index of structure (%). The correlation of parametric data was analyzed using Pearson’s correlation. Univariate and multivariate regression analysis was used to determine the predictive influence of individual variables on outcome. ROC analysis was performed to evaluate the overall performance of NLR and PLR. The level of statistical significance was considered at p ≤ 0.05.
Results
Demographic data of patient examinees are shown in Table 1. The average age in the examined group of patients with SLE was 46.3 ± 10.8 years, while the average age at the time of diagnosis was 36.6 ± 10.6 years. The median of the SLEDAI activity index in these patients was 8 (in the range from 0 to 36) with a mean value of 9.2 ± 7.5. Regarding clinical characteristics of SLE patients, 13 of them (8.1%) were in remission (SLEDAI = 0), 42 (26.2%) had low disease activity (SLEDAI = 1–5), 56 (35.0%) moderate disease activity (SLEDAI = 6–10), 26 (16.3%) had high disease activity (SLEDA = 11–19), and 23 (14.4%) patients had very high disease activity (SLEDAI ≥ 20). In addition, the occurrence of general manifestations such as weakness, malaise, and fatigue was present in 148 patients (92.5%). Arthritis and arthralgia were present in 139 (86.9%) patients, skin changes in 124 (77.5%), serositis in 78 (48.7%), lupus nephritis in 41 (25.6%) patients, and neuropsychiatric manifestations in 24 (15.0%) patients. Valvular changes in the heart were present in 9 (5.6%) patients, and peripheral neuropathy was present in 22 (13.7%) patients. Sjögren’s syndrome was present in 35 (21.9%) patients and secondary antiphospholipid syndrome in 25 (15.6%) patients.
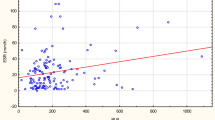
The results of this study showed that there was a positive correlation of the investigated hematological parameter NLR with the values of ESR and anti-dsDNA antibodies, as well as with the finding of PLR, while a negative correlation was found with the values of the C3 component of the complement, as shown in Table 2 in detail. Another examined hematological parameter PLR showed a positive correlation with ESR, CRP, anti-dsDNA antibodies, and anti-nucleosome antibodies as well as with urine MCP-1, while it showed a negative correlation with the C3 component of complement (Table 2). The most significant correlation between NLR and PLR is presented in Fig. 1.

Scatter plot between individual data of NLR and PLR in SLE patients
When the activity of the disease and the demographic data of the examined patients with age were analyzed, the findings showed that there was a negative correlation between the SLEDAI index and the age of the patients as well as with the age at the onset of the disease, but a positive correlation with the global physician assessment as well as with SDI, as shown in detail in Table 3.
The analysis of the examined biochemical and other immunological findings with the prognostic factor SLEDAI showed that there was a positive correlation with ESR, CRP, NLR, PLR, anti-dsDNA, anti-nucleosome antibodies, anti-C1q antibodies, and with cytokine total serum MCP-1 and urine MCP-1, while a negative correlation was observed with the C3 component of complement, as shown in detail in Table 3.
Univariate analysis indicated that all the examined laboratory parameters were independent significant predictors of disease activity in SLE patients. Further analyses using the multivariate regression method evaluated the role of all examined hematological and biochemical parameters as well as cytokines in relation to the SLEDAI index, as shown in detail in Table 4. The studied model was able to account for 21.70% of the variance in the activity index. Based on the results, ESR and serum MCP1 appeared as statistically significant risk factors.
The ROC curve was generated to assess the potential usefulness of NRL and PLR as biomarkers of disease activity in patients with SLE (the cutoff for active disease being SLEDAI ≥ 6).
The area under the ROC curve of NLR (AUC 0.643, p = 0.003) was almost equal to the curve of PLR (AUC 0.645, p = 0.003) (Fig. 2). The calculated cutoff values of NLR and PLR were 1.64 and 114.75, respectively.

ROC curve analysis of NLR and PLR in terms of SLEDAI
Discussion
It has been recently demonstrated that NLR and PLR, as economical, easily accessible, and reproducible biological markers, can be very significant clinically in numerous inflammatory diseases, such as cardiovascular [16,17,18,19], neoplastic [20,21,22,23], chronic inflammatory rheumatic diseases [3, 24,25,26], and psychiatric diseases [27], as well as in the early phases of metabolic syndrome [28]. The association of hematological indexes with SLE is still controversial [6, 25, 29, 30]. Simultaneous determination of NLR and PLR in inflammatory rheumatic diseases has been given preference, since these parameters complement each other. NLR determination can contribute to more effective disease activity monitoring, indicating mostly the presence of leukocyte inflammation, complications of various infections, and severe organ damage in SLE. However, PLR is considered significant in the assessment of the severity of systemic inflammation, with the potential to predict infections and other comorbid conditions, especially in patients with multisystem involvement [3, 25].
The studies that simultaneously determined NLR and PLR in SLE patients have been scarce. Moreover, the are no studies that compared these hematological parameters with diverse antibodies and cytokines as potential biomarkers in SLE.
PLR demonstrated a correlation with a number of studied parameters (positive correlation with ESR, CRP, anti-dsDNA, anti-nucleosome antibodies, urinary MCP-1, and inverse correlation with C3), with a higher degree of statistical significance compared to NLR. These results suggested PLR to be superior to NLR as a biomarker of SLE disease severity. None of the studied hematological parameters showed a correlation with anti-C1q antibodies. Moreover, NLR and PLR showed a positive mutual correlation.
Previous data indicate that the active form of SLE is associated with low values of the C3 complement component [10]. Therefore, it was very interesting to compare the association of NLR and PLR with the C3 complement. The results of this study demonstrated a negative correlation, based on a larger number of respondents. A previous study by Soliman et al. showed a positive correlation of NLR and PLR with ESR, CRP, and anti-dsDNA antibodies but a negative correlation with the C4 complement component [7]. In the paper by Wu et al., only NLR showed a correlation with the C3 and C4 complement components, while PLR did not [5].
Due to their high specificity, anti-dsDNA antibodies represent one of the major criteria in the new 2019 ACR/EULAR classification [31]. In addition, they have been proposed as good markers of disease activity [32,33,34,35]. The results of this study demonstrated a positive correlation of NLR with anti-dsDNA antibodies as well as PLR with anti-dsDNA antibodies. It is thought that the main antigen in SLE is nucleosome and that anti-dsDNA antibodies are just a subpopulation of the nucleosome family of antinuclear antibodies [8]. Anti-nucleosome antibodies directed against intact nucleosomes are responsible for organ damage, and in some studies, they have been demonstrated as better disease activity markers than traditional anti-dsDNA antibodies [36]. In this study, only PLR, but not NLR, was shown to be correlated with these antibodies.
In recent years, anti-C1q antibodies have been among the important SLE biomarkers, as confirmed by the latest European Alliance of Associations for Rheumatology (EULAR) recommendations of 2019, where they have been given special importance in the prediction of proliferative forms of lupus nephritis [37, 38]. Our own results concerning the absence of correlation of the studied hematological parameters with anti-C1q antibodies can be an indirect indication that NLR and PLR are not kidney involvement biomarkers in SLE, but only the biomarkers of general disease activity. In contrast, Liu et al. have recently demonstrated that NLR is a useful biomarker for the prediction of lupus nephritis [39].
In this paper, we analyzed especially the NLR and PLR association with serum and urinary MCP-1, a proinflammatory chemokine involved in lupus nephritis immunopathogenesis and considered as a potential marker of global disease activity [11, 15, 40]. It was demonstrated that urine MCP-1 values were positively correlated with PLR, while NLR was not correlated with either serum or urine MCP-1. Previous studies have not performed similar analyses of the correlation of NLR and PLR with anti-nucleosome and anti-C1q antibodies, or serum and urinary MCP-1 in patients with SLE.
Furthermore, we were especially interested in the impact of aging on disease activity, as well as the impact of earlier disease onset, demonstrating that disease activity was lower in older patients and those with later disease onset. We also demonstrated that disease activity measured by the SLEDAI was positively correlated with global physician assessment and damage index SDI, which was confirmed by other studies’ findings in different regions and in different racial patient groups [41, 42]. The results of this study showed that both studied hematological parameters were positively correlated with SLEDAI. Yolbas et al. could not demonstrate NLR and PLR association with disease activity in SLE patients [6]. The results of certain studies showed the association of NLR and PLR with SLEDAI [5, 7, 26, 29], as well as the association of NLR with lupus nephritis [5, 7].
The results of univariate analysis in our study showed that all the investigated parameters, namely ESR, CRP, NLR, PLR, C3 complement component, anti-dsDNA, anti-nucleosome, anti-C1q antibodies, and serum and urinary MCP-1, were independent predictors of disease activity with an equal high level of statistical significance (p < 0.001), indicating that cost-effective and accessible hematological parameters such as NLR and PLR can easily be the parameters for SLE activity assessment in routine clinical practice. Multivariate regression analysis revealed ESR and serum MCP-1 as the most important predictors of disease activity in SLE. The significance of ESR was also stressed in the LUMINA study, demonstrating that in SLE patients, ESR is a more potent predictor of disease activity and organ damage than anti-dsDNA antibody [43]. Recently published results of a prospective study by Cho et al. showed that NLR (but not PLR) determination was significant for disease activity and severe relapse predictions [44]. In addition, in this study based on 160 patients, the ROC curve showed that both NLR and PLR were well correlated with disease progression, which was analyzed according to SLEDAI criteria, and that they showed statistically significant specificity, which was a novelty in this work.
Limitation
This study was a single-center study.
Conclusions
Therefore, our study showed that in addition to the study of specific autoimmunity markers, their concomitant analysis with the data describing the degree of inflammation could be useful in everyday clinical practice for the assessment of SLE activity. Hematological parameters NLR and PLR can be partially helpful as preliminary markers in daily clinical work in the absence of expensive and specific analyses.
Availability of data and materials
All data and materials are available on reasonable request.
Abbreviations
- Anti-dsDNA:
-
Anti-double-stranded deoxyribonucleic acid
- CRP:
-
C-reactive protein
- MCP-1:
-
Monocyte-chemoattractant protein-1
- EULAR:
-
European Alliance of Associations for Rheumatology
- ESR:
-
Erythrocyte sedimentation rate
- NLR:
-
Neutrophil-to-lymphocyte ratios
- PLR:
-
Platelet-to-lymphocyte ratios
- SLE:
-
Systemic lupus erythematosus
- SLEDAI:
-
Systemic Lupus Erythematosus Diseases Activity Index
References
Fava A, Petri M (2019) Systemic lupus erythematosus: diagnosis and clinical management. J Autoimmun 96:1–13. https://doi.org/10.1016/j.jaut.2018.11.001
Tsokos G, Lo M, Costa Reis P, Sullivan K (2016) New insights into the immunopathogenesis of systemic lupus erythematosus. Nat Rev Rheumatol 12(12):716–730. https://doi.org/10.1038/nrrheum.2016.186
Maugeri N, Rovere-Querini P, Manfredi A (2016) Disruption of a regulatory network consisting of neutrophils and platelets fosters persisting inflammation in rheumatic diseases. Front Immunol 7:182. https://doi.org/10.3389/fimmu.2016.00182
Ramirez GA, Manfredi AA, Maugeri N (2019) Misunderstandings between platelets and neutrophils build in chronic inflammation. Front Immunol 10:2491. https://doi.org/10.3389/fimmu.2019.02491
Wu Y, Chen Y, Yang X, Chen L, Yang Y (2016) Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were associated with disease activity in patients with systemic lupus erythematosus. Int Immunopharmacol 36:94–99. https://doi.org/10.1016/j.intimp.2016.04.006
Yolbas S, Yildirim A, Gozel N, Uz B, Serdar KS (2016) Hematological indices may be useful in the diagnosis of systemic lupus erythematosus and in determining disease activity in Behçet’s disease. Med Princ Pract 25(6):510–516. https://doi.org/10.1159/000447948
Soliman MW, Sherif MN, Ghanima MI, El-Badawy AM (2020) Neutrophil to lymphocyte and platelet to lymphocyte ratios in systemic lupus erythematosus: relation with disease activity and lupus nephritis. Reumatol Clin 16(4):255–61. https://doi.org/10.1016/j.reuma.2018.07.008
Li T, Prokopec S, Morrison S et al (2015) Anti-nucleosome antibodies outperform traditional biomarkers as longitudinal indicators of disease activity in systemic lupus erythematosus. Rheumatology (Oxford) 54(3):449–457. https://doi.org/10.1093/rheumatology/keu326
Zucchi D, Elefante E, Calabresi E, Signorini V, Bortoluzzi A, Tani C (2019) One year in review 2019: systemic lupus erythematosus. Clin Exp Rheumatol 37(5):715–722
Ahearn JM, Liu CC, Kao AH, Manzi S (2012) Biomarkers for systemic lupus erythematosus. Transl Res 159(4):326–42. https://doi.org/10.1016/j.trsl.2012.01.021
Di Battista M, Marcucci E, Elefante E et al (2018) One year in review 2018: systemic lupus erythematosus. Clin Exp Rheumatol 36(5):763–777
Hochberg MC (1997) Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40(9):1725. https://doi.org/10.1002/art.1780400928
Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH (1992) Derivation of the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis Studies in SLE Arthritis Rheum 35(6):630–40. https://doi.org/10.1002/art.1780350606
Gladman D, Ginzler E, Goldsmith C et al (1996) The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index for systemic lupus erythematosus. Arthritis Rheum 39(3):363–369. https://doi.org/10.1002/art.1780390303
Živković V, Cvetković T, Mitić B et al (2018) Monocyte chemoattractant protein-1 as a marker of systemic lupus erythematosus: an observational study. Rheumatol Int 38(6):1003–1008. https://doi.org/10.1007/s00296-017-3888-x
Afari ME, Bhat T (2016) Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther 14(5):573–577. https://doi.org/10.1586/14779072.2016.1154788
Balta S, Celik T, Mikhailidis DP et al (2016) The relation between atherosclerosis and the neutrophil-lymphocyte ratio. Clin Appl Thromb Hemost 22(5):405–411. https://doi.org/10.1177/1076029615569568
Meng LB, Yu ZM, Guo P et al (2018) Neutrophils and neutrophil-lymphocyte ratio: inflammatory markers associated with intimal-media thickness of atherosclerosis. Thromb Res 170:45–52. https://doi.org/10.1016/j.thromres.2018.08.002
Wang Q, Ma J, Jiang Z, Ming L (2018) Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute pulmonary embolism: a systematic review and meta-analysis. Int Angiol 37(1):4–11. https://doi.org/10.23736/S0392-9590.17.03848-2
Ethier JL, Desautels D, Templeton A, Shah PS, Amir E (2017) Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis. Breast Cancer Res 19(1):2. https://doi.org/10.1186/s13058-016-0794-1
Ethier JL, Desautels D, Templeton A, Oza A, Amir E, Lheureux S (2017) Is the neutrophil-to-lymphocyte ratio prognostic of survival outcomes in gynecologic cancers? A systematic review and meta-analysis. Gynecol Oncol 145(3):584–594. https://doi.org/10.1016/j.ygyno.2017.02.026
Bowen R, Little NA, Harmer J et al (2017) Neutrophil-to-lymphocyte ratio as prognostic indicator in gastrointestinal cancers: a systematic review and meta-analysis. Oncotarget 8(19):32171–32189. https://doi.org/10.18632/oncotarget.16291
Li B, Zhou P, Liu Y et al (2018) Platelet-to-lymphocyte ratio in advanced cancer: review and meta-analysis. Clin Chim Acta 483:48–56. https://doi.org/10.1016/j.cca.2018.04.023
Hao X, Li D, Wu D, Zhang N (2017) The relationship between hematological indices and autoimmune rheumatic diseases (ARDs), a meta-analysis. Sci Rep 7(1):10833. https://doi.org/10.1038/s41598-017-11398-4
Gasparyan AY, Ayvazyan L, Mukanova U, Yessirkepov M, Kitas G (2019) The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med 39(4):345–357. https://doi.org/10.3343/alm.2019.39.4.345
Ma L, Zeng A, Chen B, Chen Y, Zhou R (2019) Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in patients with systemic lupus erythematosus and their correlation with activity: a meta-analysis. Int Immunopharmacol 76:105949. https://doi.org/10.1016/j.intimp.2019.105949
Ivković M, Pantović-Stefanović M, Dunjić-Kostić B et al (2016) Neutrophil-to-lymphocyte ratio predicting suicide risk in euthymic patients with bipolar disorder: moderatory effect of family history. Compr Psychiatry 66:87–95. https://doi.org/10.1016/j.comppsych.2016.01.005
Liu CC, Ko HJ, Liu WS et al (2019) Neutrophil-to-lymphocyte ratio as a predictive marker of metabolic syndrome. Medicine (Baltimore) 98(43):e17537. https://doi.org/10.1097/MD.0000000000017537
Qin B, Ma N, Tang Q et al (2016) Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) were useful markers in assessment of inflammatory response and disease activity in SLE patients. Mod Rheumatol 26(3):372–376. https://doi.org/10.3109/14397595.2015.1091136
Yu H, Jiang L, Yao L et al (2018) Predictive value of the neutrophil-to-lymphocyte ratio and hemoglobin in systemic lupus erythematosus. Exp Ther Med 16(2):1547–1553. https://doi.org/10.3892/etm.2018.6309
Aringer M, Costenbader K, Daikh D et al (2019) 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis 78(9):1151–1159. https://doi.org/10.1136/annrheumdis-2018-214819
Nasiri S, Karimifar M, Bonakdar ZS, Salesi M (2010) Correlation of ESR, C3, C4, anti-DNA and lupus activity based on British Isles Lupus Assessment Group Index in patients of rheumatology clinic. Rheumatol Int 30(12):1605–1609. https://doi.org/10.1007/s00296-016-3471-x
Bentow C, Lakos G, Martis P et al (2016) International multi-center evaluation of a novel chemiluminescence assay for the detection of anti-dsDNA antibodies. Lupus 25(8):864–872. https://doi.org/10.1177/0961203316640917
Didier K, Bolko L, Giusti D et al (2018) Autoantibodies associated with connective tissue diseases: what meaning for clinicians? Front Immunol 9:541. https://doi.org/10.3389/fimmu.2018.00541
Schäfer VS, Weiß K, Krause A, Schmidt WA (2018) Does erythrocyte sedimentation rate reflect and discriminate flare from infection in systemic lupus erythematosus? Correlation with clinical and laboratory parameters of disease activity. Clin Rheumatol 37(7):1835–1844. https://doi.org/10.1007/s10067-018-4093-3
Zivković V, Stanković A, Cvetković T, et al (2014) Anti-dsDNA, anti-nucleosome and anti-C1q antibodies as disease activity markers in patients with systemic lupus erythematosus. Srp Arh Celok Lek 142(7–8). https://doi.org/10.2298/SARH1408431Z
Orbai AM, Truedsson L, Sturfelt G et al (2015) Anti-C1q antibodies in systemic lupus erythematosus. Lupus 24(1):42–49. https://doi.org/10.1177/0961203314547791
Fanouriakis A, Kostopoulou M, Alunno A et al (2019) 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis 78(6):736–745. https://doi.org/10.1136/annrheumdis-2019-215089
Liu P, Li P, Peng Z et al (2020) Predictive value of the neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-neutrophil ratio, and neutrophil-to-monocyte ratio in lupus nephritis. Lupus 29(9):1031–1039. https://doi.org/10.1177/0961203320929753
Abujam B, Cheekatla S, Aggarwal A (2013) Urinary CXCL-10/IP-10 and MCP-1 as markers to assess activity of lupus nephritis. Lupus 22(6):614–623. https://doi.org/10.1177/0961203313484977
Stoll T, Sutcliffe N, Mach J, Klaghofer R, Isenberg DA (2004) Analysis of the relationship between disease activity and damage in patients with systemic lupus erythematosus-a 5-yr prospective study. Rheumatology (Oxford) 43(8):1039–1044. https://doi.org/10.1093/rheumatology/keh238
Sutton E, Davidson J, Bruce I (2013) The Systemic Lupus International Collaborating Clinics (SLICC) Damage Index: a systematic literature review. Semin Arthritis Rheum 43(3):352–361. https://doi.org/10.1016/j.semarthrit.2013.05.003
Vilá L, Alarcón G, McGwin Jr G, Bastian H, Fessler B, Reveille J, LUMINA Study Group (2005) Systemic Lupus Erythematosus in a Multiethnic Cohort (LUMINA): XXIX. Elevation of erythrocyte sedimentation rate is associated with disease activity and damage accrual. J Rheumatol 32 (11):2150–5.
Cho J, Liang S, Lim HHS, Lateef A, Hee Tay S, Mak A (2022) Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio reflect disease activity and flares in patients with systemic lupus erythematosus - a prospective study. Joint Bone Spine 89(4):105342. https://doi.org/10.1016/j.jbspin.2022.105342
Acknowledgements
Not applicable.
Funding
This paper is partially supported by the project Ministry of Education, Science and Technological Development of the Republic of Serbia, 451–03-47/2023–01/200111.
Author information
Authors and Affiliations
Contributions
ŽV: conceptualization (lead), data curation (lead), formal analysis (lead), investigation (lead), resources (lead), and writing—original draft (lead). CT: data curation (supporting) and resources (supporting). DBR: data curation (supporting), formal analysis (supporting), investigation (supporting), and methodology (supporting). JV: conceptualization (equal), supervision (lead), and writing—review and editing (lead). All authors reviewed and approved the final version submitted for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Institute for Treatment and Rehabilitation “Niška Banja,” Niš (№ 03–13661/1) and by the Ethics Committee of the University of Niš Faculty of Medicine (№ 01–244-5), and all the examinees gave their informed written consent in compliance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Živković, V., Cvetković, T., Dinić, B.R. et al. Correlation of hematological parameters, antibodies and cytokines with disease activity in systemic lupus erythematosus: a cross-sectional study. Egypt Rheumatol Rehabil 50, 55 (2023). https://doi.org/10.1186/s43166-023-00222-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-023-00222-9