
Abstract
Background
The co-existence of chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) is known as overlap syndrome, and both conditions share common risk factors and are associated with co-morbidities and poor outcomes.
Methodology
Sixty stable COPD patients were included in the study. We assessed body measurements, pulmonary functions to diagnose and assess COPD severity, arterial blood gases, STOB-BANG questionnaire (SBQ), Epworth sleepiness scale (ESS), and polysomnography (PSG) for diagnosis and classification of OSA severity. The aim of the study is to assess predictors of OSA among COPD patients.
Results
The prevalence of overlap syndrome was 70% among studied stable COPD patients, with a male-to-female ratio of 2:1, and SBQ and ESS were statistically higher in overlap syndrome with p values < 0.001 and 0.002, respectively. Oxygen desaturation index (ODI) was 42.72 ± 30.02 for overlap in comparison to 13.18 ± 5.80 for COPD with a significant p value of < 0.001, and T90 was significantly increased in the overlap group (26.75 ± 10.37) than the COPD-only group (1.8 ± 0.98, p value ≤ 0.001). We found a direct correlation between the GOLD stage and severity of OSA in overlap syndrome. The best cutoff value for the detection of overlap syndrome was ESS = 9 (sensitivity = 88.6% and specificity = 62.5%) and SBQ = 5 (sensitivity = 63.6% and specificity = 93.8%).
Conclusion
Overlap syndrome represents 70% of stable COPD patients. A direct relation was found between the GOLD stage and OSA severity in overlap syndrome. ESS and SBQ can be used for screening for OSA in COPD patients but with a lower cutoff value than those used for the general population.
Trial registration
Retrospectively registered, registration number is NCT05605431, date of registration October 29, 2022.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) are common disorders, and the co-existence of both conditions is called overlap syndrome [1]. Smoking, obesity, airway resistance, and inflammation are considered risk factors for both conditions, and interestingly, both COPD and OSA are associated with increased cardiovascular complications with further increased risk in overlap syndrome [2].
Multiple theories could explain that one disorder can predispose or exaggerate the other. For example, in COPD, cigarette smoking and inhaled steroids are linked to myopathy of upper airway dilator muscles. Moreover, in cor pulmonale redistribution of edema fluid in a supine position during sleep can also contribute to or exacerbate OSA [3, 4].
On the other hand, OSA patients might smoke frequently and more heavily to compensate for excessive daytime sleepiness and to help them lose weight, which results in exaggerated airway inflammation and exacerbates COPD [5]. The rationale of the study was to assess the prevalence and predictors of OSA among patients with stable COPD.
Methodology
The present study is an observational cross-section study that was carried out in the Chest Department, Faculty of Medicine, Cairo University, during the period from March 2020 to November 2020. The research ethical committee of Cairo University has approved the study (IRB: MS-81–2020). Based on the following equation [6], the calculated sample size is 60 patients with COPD is enough to detect 66% (± 14%) prevalence of OSA in COPD patients at a 95% level of confidence [7]. Sample size equation; n = (Z1-ɑ/2/d)2 *p*(1-p), where n is the calculated sample size, Zɑ/2 is the critical value that the central 95% of the Z distribution from the tail (= 1.96), p is the estimated prevalence of OSA among COPD patients (about 66%), and d is the width of confidence interval as % (± 14%).
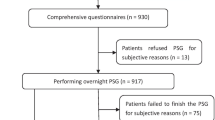
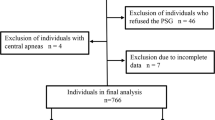
Eighty-two patients with COPD were registered to the study, 22 patients were excluded (7 patients were in exacerbation, 10 refused to do polysomnography, and 5 patients suffered from end organ failure), and 60 COPD patients were registered in the final analysis. COPD diagnosis and severity classification were based on GOLD guidelines 2020 [8]. In symptoms suggestive of sleep apnea, smoking index, history of co-morbidities, body measurements [BMI (in kg/m2), and neck circumferences], Epworth Sleepiness Scale (ESS) is widely used as a subjective measure of a patient’s sleepiness. The test is a list of eight situations in which the patient rates his tendency to become sleepy on a scale of 0, no chance of dozing, to 3, high chance of dozing. When a patient finishes the test, the sum of the values estimates the total score which ranges from 0 to 24, and the eight situations are sitting and reading, watching TV, and sitting inactive in a public place (e.g., a theater or a meeting). As a passenger in a car for an hour without a break, lying down to rest in the afternoon when circumstances permit, sitting and talking to someone, and sitting quietly after lunch without alcohol. In a car, while stopped for a few minutes in traffic, interpretation of the ESS scale as follows: 0–7: It is unlikely that you are abnormally sleepy. 8–9: You have an average amount of daytime sleepiness. 10––15: You may be excessively sleepy depending on the situation. You may want to consider seeking medical attention. 16–24: You are excessively sleepy and should consider seeking medical attention [9].
STOP-BANG questionnaire consisting of 4 self-reportable (STOP: snoring, tiredness, observed apnea, and high blood pressure) and 4 demographic (Bang: [BMI, age, neck circumference, and gender) items—interpretation scores from 0 to 2 low risk of obstructive sleep apnea, 3 to 4 intermediate risk of obstructive sleep apnea, and 5 to 8 high risk of obstructive sleep apnea [10], was evaluated in all participants. Spirometry was done using Master screen PFT 2012, CareFusion 234 GmbH, Germany (V-781267–057 version 03.00). Post-bronchodilator FEV1/FVC and FEV1% were obtained to meet the diagnosis and severity of COPD, respectively, according to GOLD guidelines 2020 [8], arterial blood gases (ABGs), polysomnography study (7 h per night) with detailed analysis, and manual scoring of the recorded data using Medicom-MTD, Model: Encephalan-EEGR-19/26) screen TM plus (cardio-respiratory screening), which is a computer-based high technology polysomnography (level 1). It included electroencephalography (EEG), electrooculography (EOG) electrodes, electromyography (EMG) electrodes for the chin and anterior tibialis muscle, nasal cannula and nasal thermistor, thoracic and abdominal belt, pulse oximetry sensor to detect arterial oxygen saturation (SpO2), ECG electrodes, snoring microphone applied on the neck beside the larynx, and body position sensor. From the recording, the following data are obtained: apnea–hypopnea index (AHI) is the total number of apneas and hypopneas/hour of sleep, and respiratory disturbance index (RDI) is the number of apneas and hypopneas plus RERAS (respiratory effort related arousals). The oxygen desaturation index is the number of desaturation episodes/hour. Oxygen desaturation is defined as a decrease in the mean oxygen saturation of ≥ 4% that lasts for at least 10 s, SpO2 < 90% time (T90 is the percentage of time spent with O2 saturation below 90% from total sleep time). The snoring index is the number of snoring events per hour of sleep, and the arrhythmia index is the number of cardiac arrhythmias/sleep hour. OSA was defined based on the American Academy of Sleep Medicine Guidelines 2014 [11]. The study population was classified based on a concomitant diagnosis of OSA into two groups: the overlap group and the COPD-only group. The aim of the study is to assess predictors of OSA among COPD patients.
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 28 (IBM Corp., Armonk, NY, USA). Data was summarized using mean, standard deviation, median, minimum, and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Mann–Whitney test [12]. For comparing categorical data, a chi-square (χ2) test was performed. The exact test was used instead when the expected frequency was less than 5 [13]. Logistic regression was done to detect independent predictors of overlap syndrome [14]. P values less than 0.05 were considered statistically significant.
Results
The current study included 60 COPD patients, they were classified into two groups: COPD alone (18 patients) and overlap syndrome (42 patients). There was no significant difference between groups regarding age, BMI, neck circumference, pulmonary functions, and ABGs. In the overlap syndrome group, systemic hypertension was detected in (59.5%), diabetes (61.9%), tachyarrhythmia (61.9%), dyslipidemia (47.6%), and ischemic heart disease (35.7%) in comparison to the COPD-only group (38%, 50%,33%, 44%, and 22%, respectively) with no statistical difference. The male-to-female ratio in COPD patients was 1:1, while in overlap syndrome patients was 2:1. Smoking index in the overlap group was 31.93 ± 32.97 versus 13.53 ± 19.69 in COPD alone group with p value = 0.05. ESS and STOP-BANG questionnaires were significantly increased in the overlap group than the COPD-only group (15.67 ± 5.75 versus 9.44 ± 8.48, p value 0.002, and 4.80 ± 1.41 versus 3.13 ± 0.89, p value < 0.001. respectively). Regarding polysomnographic data, O2 desaturation index (ODI) was 30.67 ± 26 and 3.09 ± 3.15 for overlap syndrome and COPD alone, respectively, with significant p value (< 0.001), and T90 was significantly increased in the overlap group (26.75 ± 10.37) than the COPD-only group (1.8 ± 0.98), p value = < 0.001. AHI and RDI were significantly increased in the overlap group (36.18 ± 18.65 and 37.22 ± 18.68, respectively) in comparison to the COPD-only group (2.92 ± 1.02 and 3.73 ± 2.22, respectively) with p value equals < 0.001. It was found that sleep latency was significantly reduced in the overlap group (5.05 ± 1.75) in comparison to the COPD-only group (13.5 ± 1.54), and the p value was < 0.001 (Table 1). The correlation between the degree of airway obstruction and severity of OSA in the overlap group revealed a high statistical difference in the mild OSA group as described in (Table 2). The best cutoff value for detection of overlap syndrome was ESS = 9 with sensitivity = 88.6% and specificity = 62.5% with area under curve = 75.9% (95% CI 59.7 to 92%). The best cutoff value for detection of overlap syndrome using STOP-BANG questionnaire = 4 with sensitivity = 63.6% and specificity = 93.8% with area under curve = 82.8% (95% CI 72.4 to 93.2%) (Table 3).
The significant independent predictors of overlap syndrome are ESS with OR = 1.168 (95% CI 1.018 to 1.341) and STOP-BANG with OR = 2.609 (95% CI 1.278 to 5.324) Table (4).
Discussion
The overlap of both OSA and COPD is associated with common factors affecting the pathophysiology of each disease and its outcome. The current study included 60 stable COPD patients to assess predicting factors of OSA co-existence, and 42 patients (70%) were diagnosed with overlap syndrome.
The prevalence of OSA among COPD patients was variable in previous studies, and it ranges from 35 to 77% [15,16,17,18], with one meta-analysis done by Shawon and his colleagues, reporting OSA prevalence in COPD patients between 2.9 and 65.9%. The difference in the prevalence of OSA among COPD patients may be attributed to differences in the methodology, diagnostic, and demographic criteria [19].
In our study, the mean age of overlap syndrome patients was 56.86 ± 10.20 years and in COPD patients was 52.44 ± 10.20 years with no significant difference, which is consistent with the findings of another study which was conducted on 90 COPD participants. They found that the majority of their overlap syndrome patients were under 60 years (54%) and 12% between 61 and 65 years [20].
We found that overlap syndrome was more prevalent in males (male-to-female ratio 2:1) which is consistent with the finding of one study that showed 62% of overlap syndrome patients were males [21], and in another study, 85.5% of overlap syndrome patients were men [20].
In contrast, another study revealed that the prevalence of overlap syndrome was higher in women, and this could be explained that women in their study were post-menopausal and the gender difference disappears after women go through menopause [22, 23].
The smoking index in the overlap group was 31.93 ± 32.97 versus 13.53 ± 19.69 in the COPD alone group with p value = 0.05. Smoking has an aggravated effect on the risk of development of OSA in COPD patients as smoking can lead to inflammation of the upper airway which in turn could lead to swelling and narrowing and thus increasing the tendency to airway closure [24].
The risk factors for the coexistence of OSA such as age, gender, and smoking may not provide clinical relevance in determining the probability of OSA, especially that in advanced COPD, they may have different predictors from the general population [21].
In the current work, the mean BMI of overlap syndrome patients was 42.81 ± 11.31 kg/m2 and that of COPD patients was 39.12 ± 11.03 kg/m2 with no significant difference between COPD and overlap syndrome patients. This goes with another study, where they found no significant difference in BMI between COPD and overlap syndrome groups [25]. However, in a study done by Gunduz et al., BMI was significantly higher in the overlap syndrome group compared to the COPD group [26].
The findings that there was no significant difference in BMI between overlap syndrome and COPD patients in our research might be explained by the fact that we did not perform additional measures of central adiposity, which may be increased among OSA patients in the setting of a normal or high BMI. It is well known that low body weight is common in COPD patients, but previous data suggested that about 65% of COPD patients might be overweight or obese and that low BMI in advanced COPD carries a poor prognosis [27].
We found no significant difference in neck circumference between COPD and overlap syndrome participants, and it was 42.88 ± 4.98 cm and 46.47 ± 8.43, respectively.
This matches the findings of another study performed on 54 COPD patients where PSG was done to screen for OSA, and the mean neck circumferences were 40.7 cm and 35.1 cm for males and females, respectively, showing that OSA is common in patients with advanced COPD even among those with small neck circumference. The use of corticosteroids in COPD patients is responsible for increased fat deposition in the neck leading to increased OSA risk and may produce changes in airway collapsibility and ventilatory control that overcomes neck size [21].
Our study showed that the most common co-morbidities in overlap syndrome patients were diabetes type 2 and tachyarrhythmia (61.9%) for each of them followed by systemic hypertension (59.5%), hyperlipidemia (47.6%), and ischemic heart disease (35.7%).
Our results matched another study which had demonstrated that overlap syndrome patients suffered from multiple co-morbidities compared to COPD patients and matched for sex, age, and BMI. The most common conditions were diabetes, followed by hypertension, tachyarrhythmia, and dyslipidemia. However, the difference between the type and percent of co-morbidities did not reach a statistically significant level [28].
Asystole (no electrical heart activity and my last 2–6 s) is one of the bradyarrhythmias that may occur in up to 18% of OSA patients even in the absence of cardiac diseases was also reported in literature [29].
Papachatzakis and co-authors concluded that COPD and OSA share common risk factors and pathophysiological mechanisms, and both conditions had systemic inflammatory state, oxidative stress, and endothelial dysfunction which contribute to the development of co-morbidities [28].
We did not find a significant difference between both groups regarding pulmonary functions and ABGs. Similarly, previous studies found no difference between both groups regarding ABGs, and they concluded that ABGs cannot be used to predict OSA in COPD patients [30]. Also, many studies found no significant difference in pulmonary function tests between COPD and overlap syndrome groups [7, 31, 32].
As expected, we found higher RDI, AHI, T90, and ODI in the overlap group than in COPD alone with a significant p value < 0.001. Previous researchers showed the same findings [33, 34]. In well recognized that breathing cessation, nocturnal hypoxemia, sleep fragmentation, and frequent arousals in OSA could activate the sympathetic system, trigger oxidative stress, and result in low-grade systemic inflammatory state. This explains the link between OSA and endothelial dysfunction and cardio-metabolic risks [28].
In contrast, other studies found that ODI is not sensitive or specific for screening for OSA in COPD as it may result in underestimation of OSA, and this may be related to the use of oxygen therapy in some COPD patients making ODI non-diagnostic [30, 35].
Comparison of both groups regarding the ESS and STOP-BANG questionnaire (15.67 ± 5.75, p value 0.002 and 4.80 ± 1.41, p value < 0.001, respectively) revealed a significant increase of both scales in the overlap group as described in Table 2.
The best cutoff value for detection of overlap syndrome was ESS = 9 with sensitivity = 88.6% and specificity = 62.5% and the best cutoff value for detection of overlap syndrome using STOP-BANG questionnaire = 4 with sensitivity = 63.6% and specificity = 93.8% (Table 3). We found that the significant independent predictors of overlap syndrome are ESS and STOP-BANG (Table 4).
This goes with the findings of a previous study conducted by Schreiber et al., where they found a significant increase in ESS in overlap syndrome than COPD patients, with lower cutoff values of ESS (< 10) [30]. Another study found that an ESS cutoff value of 10 was not accurate in predicting or excluding OSA in COPD patients, which means that the usual cutoff values may be misleading and could underestimate OSA prevalence in COPD patients [36], which is matched with our findings.
Previous studies found a higher STOP-BANG questionnaire in the overlap group than in COPD patients, and they concluded that it could be used in screening for OSA in COPD patients [17, 18].
One study revealed that a STOP-BANG questionnaire ≥ 3 can predict OSA in COPD patients while a score ≥ 4 had higher possibility to predict OSA and could be used to predict disease severity [37].
When describing the relation between the severity of airway obstruction and the severity of OSA in the overlap group (as in Table 2), we found a direct correlation between the GOLD stage and severity of OSA with a statistically significant difference of p value < 0.001, 0.040, and 0.004 for mild, moderate, and severe OSA, respectively.
Many studies found a positive association between the severity of OSA and GOLD stages [7, 38, 39] which matches our findings.
On the other hand, studies found an inverse correlation between the degree of airway obstruction and severity of OSA in COPD patients, which means the more severe the obstruction the lower AHI, and they concluded that lower FEV1 could play a protective role against OSA severity [5, 40]. Severe airflow obstruction is associated with increased end-expiratory volume which prevents upper airway collapse and maintains its patency [36], which does not match our results.
However, a more recent study found a lack of relationship between the severity of airway obstruction and the severity of OSA [41].
This conflict of studies regarding the direction of the correlation of severity of both conditions may be related to the difference in the studied population, and whether different phenotypes of OSA and COPD may have a certain relationship, this hypothesis needs further research.
Limitations of the study are as follows: it is a single-center study and has a small number of patients, we did not study the effect of initiating NIV on prognosis and mortality, and we did not identify different OSA and COPD phenotypes which may show different relationships.
Conclusions
Our data revealed that 70% of COPD patients included in the study had overlap syndrome. We found a direct relationship between the GOLD stage and the severity of OSA in the overlap group. ESS and SBQ can be used for screening for OSA in COPD patients but with lower cutoff values ( 8.5 and 4.5, respectively) than used for the general population.
Availability of data and materials
The data of the current study are available from the corresponding author upon reasonable request.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- OSA:
-
Obstructive sleep apnea
- SBQ:
-
STOP-BANG questionnaire
- ESS:
-
Epworth sleepiness scale
- PSG:
-
Polysomnography
- ODI:
-
Oxygen desaturation index
- T90:
-
Percentage of cumulative time with oxygen saturation < 90% in total sleep time
- AHI:
-
Apnea–hypopnea index
- RDI:
-
Respiratory disturbance index
- GOLD:
-
Global initiative of chronic obstructive lung disease
- BMI:
-
Body mass index
- PFT:
-
Pulmonary function test
- FEV1:
-
Forced expiratory volume in the first second
- FVC:
-
Forced vital capacity
- ABGs:
-
Arterial blood gases
- EEG:
-
Electoencephalogram
- EOG:
-
Electrooculogram
- EMG:
-
Electromyogram
- Sao2:
-
Arterial oxygen saturation
- ECG:
-
Electrocardiogram
- RERAs:
-
Respiratory effort-related arousals
- SpO2:
-
Oxygen saturation by pulse oximetry
- NIV:
-
Non-invasive ventilaton
References
Owens RL, Malhotra A (2010) Sleep-disordered breathing and COPD: the overlap syndrome. Respir Care. 55(10):1333–44 discussion 1344-6. PMID: 20875160; PMCID: PMC3387564
Ioachimescu OC, Teodorescu M (2013) Integrating the overlap of obstructive lung disease and obstructive sleep apnoea: OLDOSA syndrome. Respirology 18:421–431
Teodorescu M, Xie A, Sorkness CA, Robbins J, Reeder S, Gong Y, Fedie JE, Sexton A, Miller B, Huard T, Hind J, Bioty N, Peterson E, Kunselman SJ, Chinchilli VM, Soler X, Ramsdell J, Loredo J, Israel E, Eckert DJ, Malhotra A (2014) Effects of inhaled fluticasone on upper airway during sleep and wakefulness in asthma: a pilot study. J Clin Sleep Med 10(2):183–193. https://doi.org/10.5664/jcsm.3450.PMID:24533002;PMCID:PMC3899321
Friedman M, Wilson MN, Pulver T, Pandya H, Joseph NJ, Lin HC, Chang HW (2010) Screening for obstructive sleep apnea/hypopnea syndrome: subjective and objective factors. Otolaryngol Head Neck Surg 142(4):531–535. https://doi.org/10.1016/j.otohns.2009.12.038. PMID: 20304273
Krachman SL, Tiwari R, Vega ME, Yu D, Soler X, Jaffe F, Kim V, Swift I, D’Alonzo GE, Criner GJ, COPDGene Investigators (2016) Effect of emphysema severity on the apnea-hypopnea index in smokers with obstructive sleep apnea. Ann Am Thorac Soc. 13(7):1129–35. https://doi.org/10.1513/AnnalsATS.201511-765OC. PMID: 27078132; PMCID: PMC5015748
Dawson B, Trapp RG (eds) (2004) Basic and clinical biostatistics, 4th edn. McGraw-Hill Professional, New York
Soler X, Gaio E, Powell FL et al (2015) High prevalence of obstructive sleep apnea in patients with moderate to severe COPD. Ann Am Thorac Soc 12:1219. https://doi.org/10.1513/AnnalsATS.201407-336OC11. 150414075541005
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2020 Report. GOLD COPD. https://goldcopd.org/gold-reports/. Accessed 31 Mar 2019. WebCite Cache.
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14(6):540–545. https://doi.org/10.1093/sleep/14.6.540. PMID: 1798888
Chung F, Abdullah HR, Liao P (2016) STOP-Bang questionnaire: a practical approach to screen for obstructive sleep apnea. Chest 149(3):631–638. https://doi.org/10.1378/chest.15-0903. Epub 2016 Jan 12 PMID: 26378880
American Academy of Sleep Medicine (AASM) (2014) International classification of sleep disorders, 3rd edn. American Academy of Sleep Medicine, Darien
Chan YH (2003) Biostatistics102: quantitative data – parametric & non-parametric tests. Singapore Med J 44(8):391–396
Chan YH (2003) Biostatistics 103: qualitative data – tests of independence. Singapore Med J 44(10):498–503
Chan YH (2004) Biostatistics 202: logistic regression analysis. Singapore Med J 45(4):149–153
Steveling EH et al (2014) Predictors of the overlap syndrome and its association with comorbidities in patients with chronic obstructive pulmonary disease. Respiration 88(6):451–457
Hu W et al (2020) Obstructive sleep apnea increases the prevalence of hypertension in patients with chronic obstructive disease. COPD 17(5):523–532
Xiong MQ et al (2019) Analysis of risk factors and consequences for concurrent obstructive sleep apnea in chronic obstructive pulmonary disease patients. Zhonghua Jie He He Hu Xi Za Zhi 42(11):832–837
Zhang P, Chen B, Lou H et al (2022) Predictors and outcomes of obstructive sleep apnea in patients with chronic obstructive pulmonary disease in China. BMC Pulm Med 22:16. https://doi.org/10.1186/s12890-021-01780-4
Shawon MS et al (2017) Current evidence on prevalence and clinical outcomes of co-morbid obstructive sleep apnea and chronic obstructive pulmonary disease: a systematic review. Sleep Med Rev 32:58–68
Jimborean G, Szasz S, Szathmary M, Csipor A, Arghir OC, Nemes RM, Postolache P, Ianos ES (2018) Association between chronic obstructive pulmonary disease and sleep apnea - overlap syndrome- experience of pulmonology clinic Tg. Mures. Romania. Rev Chim 69(4):1014–1017. https://doi.org/10.37358/RC.18.4.6249
Soler X, Liao SY, Marin JM et al (2017) Age, gender, neck circumference, and Epworth sleepiness scale do not predict obstructive sleep apnea (OSA) in moderate to severe chronic obstructive pulmonary disease (COPD): the challenge to predict OSA in advanced COPD. PLoS One 12:e0177289
Smith Robert, Ronald John, Delaive Kenneth, Walld Randy, Manfreda Jure, Kryger Meir H (2002) What are obstructive sleep apnea patients being treated for prior to this diagnosis? Chest 121(1):164–172. https://doi.org/10.1378/chest.121.1.164. ISSN 0012-3692
Shepertycky MR, Banno K, Kryger MH (2005) Differences between men and women in the clinical presentation of patients diagnosed with obstructive sleep apnea syndrome. Sleep 28(3):309–314 PMID: 16173651
McNicholas WT (2009) Chronic obstructive pulmonary disease and obstructive sleep apnea: overlaps in pathophysiology, systemic inflammation, and cardiovascular disease. Am J Respir Crit Care Med 180(8):692–700. https://doi.org/10.1164/rccm.200903-0347PP. Epub 2009 Jul 23 PMID: 19628778
Calderón-Osuna E, Carmona Bernal C, Arenas Gordillo M, Fuentes Pradera MA, Sánchez Armengol A, Capote Gil F (1999) Estudio comparativo de pacientes con enfermedad pulmonar obstructiva crónica con y sin síndrome de apneas obstructivas durante el sueño [A comparative study of patients with chronic obstructive pulmonary disease with and without obstructive sleep apnea syndrome]. Arch Bronconeumol 35(11):539–43. https://doi.org/10.1016/s0300-2896(15)30006-5. Spanish PMID: 10687038
Gunduz C, Basoglu OK, Tasbakan MS (2018) Prevalence of overlap syndrome in chronic obstructive pulmonary disease patients without sleep apnea symptoms. Clin Respir J 12(1):105–112
Koniski ML, Salhi H, Lahlou A, Rashid N, El Hasnaoui A (2015) Distribution of body mass index among subjects with COPD in the Middle East and North Africa region: data from the BREATHE study. Int J Chron Obstruct Pulmon Dis 10:1685–1694
Papachatzakis I, Velentza L, Zarogoulidis P, Kallianos A, Trakada G (2018) Comorbidities in coexisting chronic obstructive pulmonary disease and obstructive sleep apnea - overlap syndrome. Eur Rev Med Pharmacol Sci 22(13):4325–4331. https://doi.org/10.26355/eurrev_201807_15429. PMID: 30024626
Rossi Valentina A, Stradling John R, Kohler Malcolm (2013) Effects of obstructive sleep apnoea on heart rhythm. Eur Respir J 41(6):14391451. https://doi.org/10.1183/09031936.00128412)
Schreiber A, Cemmi F, Ambrosino N, Ceriana P, Lastoria C, Carlucci A (2018) Prevalence and predictors of obstructive sleep apnea in patients with chronic obstructive pulmonary disease undergoing inpatient pulmonary rehabilitation. COPD: J Chronic Obstr Pulmon Dis 15(3):265–270. https://doi.org/10.1080/15412555.2018.1500533
Güllü Z, İtil O, Öztura İ, Aslan Ö, Ceylan E, Baklan B, Ellidokuz H (2002) Kronik Obstrüktif Akciğer Hastalığı ve Obstrüktif Uyku Apne Sendromu Birlikteliği (Overlap sendromu). Toraks Dergisi 3:161–167
Venkateswaran S, Tee A (2014) Overlap syndrome between chronic obstructive pulmonary disease and obstructive sleep apnoea in a Southeast Asian teaching hospital. Singapore Med J 55(9):488
Turcania P, Skrickova J, Pavlik T, Janousova E, Orban M (2015) The prevalence of obstructive sleep apnea in patients hospitalized for COPD exacerbation. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 159(3):422–428
Marin J, Soriano J, Carrizo S, Boldova A, Celli B (2010) Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med 182(3):325–331
Scott AS, Baltzan MA, Wolkove N (2014) Examination of pulse oximetry tracings to detect obstructive sleep apnea in patients with advanced chronic obstructive pulmonary disease. Can Respir J 21(3):171–175
Faria AC, da Costa CH, Rufino R (2015) Sleep apnea clinical score, Berlin questionnaire, or epworth sleepiness scale: which is the best obstructive sleep apnea predictor in patients with COPD? Int J Gen Med 8:275–281. https://doi.org/10.2147/IJGM.S86479
Mengqing X, Weihua H, Minglin D, Meifang W, Junwen C, Hanzhong X et al (2019) The screening value of ESS, SACS, BQ, and SBQ on obstructive sleep apnea in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 14:2497–2505
Putcha N, Crainiceanu C, Norato G et al (2016) Influence of lung function and sleep-disordered breathing on all-cause mortality. A community-based study. Am J Respir Crit Care Med 194(8):1007–1014. https://doi.org/10.1164/rccm.201511-2178OC10
López-Acevedo MN, Torres-Palacios A, Elena Ocasio-Tascón M, Campos-Santiago Z, Rodríguez-Cintrón W (2009) Overlap syndrome: an indication for sleep studies?: a pilot study. Sleep Breath Schlaf Atm 13(4):409–413. https://doi.org/10.1007/s11325-009-0263-512
Zhu J, Zhao Z, Nie Q, Wang Y, Fu Z, Guo X, Hu K (2020) Effect of lung function on the apnea-hypopnea index in patients with overlap syndrome: a multicenter cross-sectional study. Sleep Breath 24(3):1059–1066
Stewart NH, Brittan M, McElligott M, Summers MO, Samson K, Press VG (2022) Evaluating the relationship of airflow obstruction in COPD with severity of OSA among patients with overlap syndrome. Int J Chron Obstruct Pulmon Dis 17:1613–1621. https://doi.org/10.2147/COPD.S355897
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
1) Safy Zahid Kaddah was responsible for the conception and design, revising, and final approval of the article. 2) Yousef Mohamed Amin Soliman is responsible for the acquisition of the data, analysis, drafting of the article, and final approval of the manuscript. 3) Heba Mousa is responsible for the acquisition of the data and analysis, drafting of the article, and final approval of the manuscript. 4) Naglaa Moustafa is responsible for the acquisition of the data and analysis, revising, and final approval of the article. 5) Eman Kamal Ibrahim is responsible for the conception and design, revising and writing, and final approval of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant regulations and guidelines, informed consent was obtained from all participants and/or their legal guardian, and the study was approved by the research ethical committee, Cairo University, with IRB (MS-81–2020).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaddah, S.Z., Soliman, Y.M.A., Mousa, H. et al. Predictors of obstructive sleep apnea in patients with chronic obstructive pulmonary disease. Egypt J Bronchol 17, 70 (2023). https://doi.org/10.1186/s43168-023-00236-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00236-z