
Abstract
Background
Vitamin K is associated with reduced cardiovascular disease risk such as heart failure, possibly by carboxylation of matrix-gla protein (MGP), a potent inhibitor of vascular calcification. The relationship of vitamin K intake or status with cardiac structure and function is largely unknown. Therefore this study aims to investigate the prospective association of vitamin K status and intake with echocardiographic measures.
Methods
This study included 427 participants from the Hoorn Study, a population-based cohort. Vitamin K status was assessed at baseline by plasma desphospho-uncarboxylated MGP (dp-ucMGP) with higher concentrations reflecting lower vitamin K status. Vitamin K intake was assessed at baseline with a validated food-frequency questionnaire. Echocardiography was performed at baseline and after a mean follow-up time of 7.6, SD=±0.7 years. We used linear regression for the association of vitamin K status and intake with left ventricular ejection fraction (LVEF), left atrial volume index (LAVI) and left ventricular mass index (LVMI), adjusted for potential confounders.
Results
The mean age was 66.8, SD=±6.1 years (51% were male). A high vitamin K status was prospectively associated with decreased LVMI (change from baseline to follow-up: -5.0, 95% CI: -10.5;0.4 g/m2.7) for the highest quartile compared to the lowest in women (P-interaction sex=0.07). No association was found in men. Vitamin K status was not associated with LVEF or LAVI. Vitamin K intake was not associated with any of the echocardiographic measures.
Conclusions
This study showed a high vitamin K status being associated with decreased LVMI only in women, while intakes of vitamin K were not associated with any cardiac structure or function measures. These results extend previous findings for a role of vitamin K status to decrease heart failure risk.
Similar content being viewed by others


Introduction
Vitamin K is a fat-soluble vitamin occurring in two biologically active forms; phylloquinone (vitamin K1) and menaquinones (vitamin K2) [1]. Vitamin K1 is mainly derived from green leafy vegetables, while vitamin K2 mainly occur in fermented animal products like cheese and meat. Vitamin K functions a co-factor for carboxylation (activation) of gla-proteins [2].
Matrix-gla protein (MGP) is a vitamin-K dependent protein and a potent inhibitor of vascular calcification [3]. Luo et al. showed that MGP knock-out mice died within 6-8 weeks due to massive calcification [3]. In humans, loss-of-function mutations in the gene coding for MGP result in the Keutel syndrome, which is characterized by abnormal calcification of cartilaginous tissues associated with malformations of skeletal tissues and arterial calcification [4]. Furthermore, animal and human intervention studies showed that vitamin K supplementation may reduce vascular calcification by carboxylating MGP [5,6,7].
Uncarboxylated MGP, as measured by desphospho-uncarboxylated MGP (dp-ucMGP) has been suggested as a marker for vitamin K status, with high concentrations indicating a low vitamin K status [5]. Although currently no single gold-standard marker is available to estimate vitamin K status, dp-ucMGP is considered the most suitable to assess vascular vitamin K status and measure vitamin K deficiency, as its concentrations correlate with long-term vitamin K intake [8, 9]. High concentrations of dp-ucMGP have been associated with increased vascular calcification [10] and risk of cardiovascular outcomes [11, 12], despite some conflicting results related to specific forms of cardiovascular disease (CVD) [13, 14]. Indeed, in a couple of studies the association between dp-ucMGP concentrations and coronary artery disease and stroke was absent [13] or appeared to be inverse [14]. Conversely, Dalmeijer et al. showed that the association between dp-ucMGP and CVD risk was mainly driven by heart failure (HF) and peripheral artery disease [11]. Use of vitamin K antagonists is also associated with increased vascular calcification in animal models [15, 16]. On the other hand, a higher vitamin K intake has been associated with a reduced risk of vascular calcification and CVD in prospective population-based cohorts [17].
Studies on the relationship of vitamin K intake or status with cardiac structure and function are, however, scarce. Objectively measured aspects of cardiac structure and function such as left ventricular mass index (LV, LVMI) or ejection fraction (LVEF) reflect the underlying hemodynamic alterations associated with HF, and echocardiography represents the gold standard for their assessment. In patients with HF, high dp-ucMGP concentrations were associated with the degree of LV systolic dysfunction [18] and with mortality [19]. Conversely, a high vitamin K intake has been associated with a reduced HF mortality [20]. Finally, three cross-sectional studies investigated the relation of vitamin K status with cardiovascular function, indicating significant associations between higher concentrations of dp-ucMGP and reduced LVEF [21], higher carotid-femoral pulse wave velocity [22] and depressed LV diastolic function [23]. However, prospective studies investigating the relationship between vitamin K status and intake with cardiac structure and function are currently lacking.
Therefore, the aim of this study is to investigate the association of vitamin K status and vitamin K intake with cardiac structure and function in a prospective, population-based cohort, the Hoorn Study.
Materials/subjects and methods
Study population
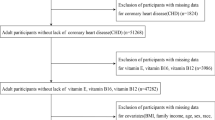
The Hoorn Study is a prospective observational cohort study in Dutch older adults initiated in 1989 with the aim to estimate the prevalence of pre-diabetes and diabetes in the general population. Adults living in Hoorn, in the region of the West-Friesland in The Netherlands, aged 50–75 years and able to provide consent were considered eligible. Among the eligible 11,500 participants, 3,553 were randomly selected from the municipal registry and 71.5% of those agreed to participate. After the exclusion of 56 participants of non-Western origin, 2,484 were included (age 61.7±6.7, 54.1% female) [24]. More detailed information on the research design, procedures and methods, has been published previously [24]. Participants of the Hoorn Study have been followed up via several visits. We included 831 participants who participated in extensive cardiovascular examinations in the year 2000-2001, considered as baseline. This group was oversampled for individuals with impaired glucose tolerance (IGT) and type 2 diabetes mellitus to enable investigation of effect modification by glucose tolerance status [24]. After 8 years of follow-up (2007-2009), a repeated echocardiogram was obtained in 438 participants (details about loss to follow up are displayed in Additional file 1).
Participants with unsatisfactory echocardiograms at follow-up, and with missing data on vitamin K status or intake for the respective analyses were excluded, resulting in 405 participants for analyses on vitamin K status and 427 participants for analyses on intake (Additional file 1). We did not have complete data on all three echocardiographic outcomes, which resulted in different analytic samples for each outcome measure with n=301 for LVEF, n=309 for LV mass index (LVMI) and of n=324 for left atrial volume index (LAVI) for vitamin K status and of n=312 for LVEF, n=324 for LVMI and n=335 for LAVI for vitamin K intake. All participants provided written informed consent and the local ethics committee of the VU University Medical Center approved the study.
Vitamin K status
Study personnel collected morning blood samples in a 8-12 h fasted state. Citrated samples were stored at -80°C until assessment of biochemical measures. Vitamin K status was measured at baseline by plasma dp-ucMGP concentration. The analysis of dp-ucMGP were performed after the follow-up visits were completed, which was approximately 8-9 years after storage. Information on the stability of the biomarker during storage are not directly available from this study but from previous studies that used and tested the same procedure, showing a correlation of 0.67 for dp-ucMGP measurements taken over 5 years apart [10]. Dp-ucMGP concentration was measured by a sandwich ELISA with the capture of antibody directed against the nonphosphorylated MGP sequence 3 to 15 (mAb-dpMGP; VitaK BV, Maastricht, the Netherlands). High levels of dp-ucMGP reflect a low vitamin K status [5]. The interassay coefficient of variation was 9.9%.
Vitamin K intake
At baseline, dietary intake was assessed using a self-administered validated food frequency questionnaire (FFQ) [25], allowing the estimation of the average daily intake of 178 foods over 77 main food categories in the year preceding enrolment. The 1993 Dutch food consumption table (NEVO) was used to calculate energy and nutrient intakes [26]. This table does not include information on vitamin K content of all food products. Therefore, the vitamin K1, short chain vitamin K2 and long chain vitamin K2 concentrations in a series of Dutch foods were assessed at the R&D Group VitaK, Maastricht University. These values were supplemented with earlier analyses by Schurgers and Vermeer and the U.S. food composition database [27]. Finally the vitamin K database was completed by estimating vitamin K1 and vitamin K2 content through recipes and ingredient information. The relative validity of the FFQ for vitamin K, with this database, has been assessed against 12 monthly 24-hour recalls among 121 men and women [27]. At the time dietary intake was assessed, the most commonly used dietary supplements in the Netherlands did not include vitamin K and vitamin K supplements were thus not questioned in the food-frequency questionnaire. Therefore, vitamin K intake reflected only dietary sources. The relative validity for energy adjusted vitamin K1, vitamin K2, short- and long- chain vitamin K2 intake were 0.34, 0.56, 0.32 and 0.66, respectively.
Echocardiography
Experienced ultrasound analysts performed the echocardiographic imaging at baseline (2000/2001) and at follow-up (2007/2009), using the HP SONOS 5500 echocardiography system (2-4 MHz transducer, Andover, MA, USA) according to a standardized protocol consisting of two-dimensional, M-mode and pulsed wave Doppler assessments [28]. All echocardiograms were evaluated afterwards by a senior cardiologist.
Cardiac structure was measured by LVMI, which was calculated from linear dimensions by using the American Society of Echocardiography recommended formula and indexed to height2.7 [28]. LV systolic function was determined by LVEF (%), which was calculated using the modified Simpson’s rule [28]. As a marker of LV diastolic function the left atrial volume was measured at end-systole and indexed by body surface area resulting in LAVI (mL/m2) [29].
Covariates
At baseline, participants were asked to fill out questionnaires about lifestyle factors, medical history (including family history of diabetes (yes/no), medication use (yes/no), disease history and diabetes-related complaints (yes/no), and smoking status (never/former/current smokers) [24]. Physical activity (h/day), including commuting activities, leisure time physical activity and occupational activities, was assessed by using the Short Questionnaire to Assess Health-enhancing physical activity (SQUASH), which has been previously validated [30]. Dietary intake of other nutrients than vitamin K was based on self-report using by the same validated FFQ [25]. Educational level was self-reported based on the highest ascertainment, and stratified according to three categories: 1) low (no/primary education); 2) middle (secondary education); 3 high (tertiary education). Information on prior and incident CVD was based on self-report in combination with medical records. CVD included myocardial infarction, angina pectoris, heart failure, stroke, transient ischemic attack and peripheral artery disease. In our morbidity and mortality registration, cardiovascular events were coded according to the International Classification of Diseases, Injuries and Causes of Death, ninth revision, including ICD-9 codes 390–459, and 798. Weight was divided by height squared to calculate body mass index (BMI, kg/m2). Blood pressure (mmHg) was measured twice at the left upper arm in a sitting position using an oscillometric device and averaged (Collin Press-Mate, BP-8800). Glucose tolerance status (NGT, IGT or diabetes) was determined using the results of an oral glucose tolerance test combined with the fasting glucose levels, according to the WHO 1999 criteria [31]. The estimated glomerular filtration rate (eGFR, mL/min) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI 2009) equation [32]. Plasma brain natriuretic peptide (BNP) was determined in spare frozen EDTA samples, which had been stored at –80°C for 4 years. BNP was determined in pmol/L (equivalent to 3.5 pg/mL) using an immunoradiometric assay kit (Shionoria, Osaka, Japan) with inter- and intra-assay variability coefficients in the relevant range <10% [33].
Statistical analyses
All analyses were performed using SPSS Statistics, version 22.0 and R software version 3.1.1 (R-Foundation Statistical Computing). Variables were summarized as arithmetic mean and standard deviation for normally distributed data or as median with IQR range for data not normally distributed. Two-sided P-values of <0.05 were considered statistically significant. Vitamin K status and energy-adjusted intakes of all forms of vitamin K were categorized into quartiles. For vitamin K status the quartile with the highest dp-ucMGP concentrations and thus the lowest vitamin K status was used as the reference category. For quartiles of vitamin K intake, the lowest quartile was used as the reference category. Baseline characteristics were summarized by quartiles of vitamin K status and intake. Differences across quartiles of vitamin K status or intake were assessed by ANOVA for continuous measures and by a chi-square test for categorical variables.
Missing values for any covariates were present in 279 and 301 participants respectively for analyses on vitamin K status and intake, ranging from 0.2% for HbA1c to 2.9% for presence of CVD, and only BNP had 20.1% missing data. Multiple imputations were used combining ten iterations into one imputation model.
The longitudinal association of vitamin K status and intake with LVEF, LVMI and LAVI at follow-up were estimated using linear regression models adjusted for follow-up duration, glucose tolerance status and baseline value of the echocardiographic outcome. We additionally adjusted for confounders in a stepwise manner. Model 1 was adjusted for age and sex. Model 2 was additionally adjusted for BMI, smoking, physical activity, systolic blood pressure, presence of CVD, cholesterol, HbA1c and education. For vitamin K intake, we additionally adjusted for dietary factors associated with vitamin K intake: total energy intake, protein, saturated fat, fiber, calcium and vitamin C. All nutrients were modeled as continuous variables and adjusted for total energy intake by using the residual method [34]. The median level of vitamin K status or intake in each quartile was included as a continuous factor in the analysis to assess the P-trend over the categories.
We also included the quadratic term of continuous vitamin K status or intake along with the continuous term to assess evidence for deviation of a linear relationship. In case this quadratic term was significant, we used spline regression to explore the functional forms of the prospective associations between continuous vitamin K status or intake and echocardiographic measures.
Sex, glucose tolerance status and prior CVD were assessed as effect modifiers by including interaction terms in the fully adjusted models. Wald tests were used to assess whether the models with the interaction terms differed significantly from the initial models. A p-value <0.10 was considered statistically significant; in case interaction was present we stratified the results [35].
Sensitivity analyses were conducted by excluding cases with incident CVD during follow-up and by adjusting the final model for changes over time in smoking, physical activity and BMI. Finally, to investigate selection bias due to loss to follow-up, baseline characteristics of participants and dropouts were tested by an independent t-test for continuous variables and a chi-square test for categorical variables. Furthermore, a sensitivity analysis was performed using inverse-probability weighting for the longitudinal models.
Results
Baseline characteristics
Our study population for vitamin K status of 405 participants had a mean age of 66.8±6.1 years and 50.9% was male. At baseline, participants with a higher vitamin K status were younger, more frequently male, more frequently current smokers, had a lower systolic blood pressure and lower BMI than those with a low vitamin K status (Table 1). Among the 427 participants for vitamin K intake analyses, those with a high vitamin K intake were younger, less frequently male, lower educated, more physically active and had higher intakes of protein, fiber, vitamin C and calcium than those with a low vitamin K intake (Additional file 2). Those excluded in this study were older, had lower vitamin K status, higher prevalence of diabetes and prior CVD and slightly higher BMI and systolic blood pressure. Additionally, they showed a slightly worse cardiac structure and function, in particular a higher LVMI and a larger LAVI than those included in the analysis (Additional file 3).
Vitamin K status
Mean vitamin K status was 578±410 pmol/L and showed a distribution somewhat skewed to the right. The mean follow-up time was 7.6 ±0.7 years.
In the linear regression models, including interaction terms for sex, glycemic status or previous CVD showed only evidence of interaction between vitamin K status and sex for LVMI (P=0.07) and results are therefore stratified by sex. Including a quadratic term in the model was statistically significant (P=0.018), suggesting evidence for a non-linear association. We observed a significant inverse relationship between vitamin K status and decreased LVMI in women for quartile 1 and 2 compared to quartile 4: -6.5(-11.2;-1.8) and -7.2(-11.9;-2.6) (g/m2.7) respectively, adjusted for model 1 (P-for trend<0.001). Further adjustment for model 2 slightly attenuated the association, and only quartile 2 was still significant: -6.8 (-11.8; -1.8). However the P-for trend remained strongly significant <0.001. In men, no significant association was observed. Evaluation of the continuous associations of vitamin K status with LVMI using splines revealed a similar pattern for men and women with some non-linearity in the tails (Figure 1). Vitamin K status was not associated with either LVEF or LAVI after follow-up with estimates of 1.1 (-2.4;4.5) (%) and -0.1 (-3.3;3.3) (mL/m2) for quartile 1 compared to quartile 4, respectively, adjusted for model 2 (Table 2).

Continuous association of vitamin K status with left ventricular mass index stratified by sex among the inner 95% of concentrations. Women N=199; men N=206. Splines are adjusted for age, follow-up time, glucose status and baseline left ventricular mass index. Below each spline is the histogram depicted to illustrate the distribution of dp-ucMGP (pmol/L). High dp-ucMGP is indicative for low vitamin K status
Vitamin K intake
Mean total vitamin K intake was 220±78 mg/day (184 mg/day vitamin K1 and 35.5 mg/day vitamin K2). We did not observe significant associations between any of the forms of energy-adjusted vitamin K intake at baseline and LVMI at follow-up adjusted for CVD risk factors and dietary factors (Table 3). Similarly, for LVEF we observed no significant associations for any of the forms of vitamin K intake. Although we found some evidence of a non-linear association for total vitamin K (P=0.041) and vitamin K1 (P=0.059) with LVEF, the spline regression did not provide evidence for a significant association (Additional file 4).
In addition, we observed effect modification by presence of CVD for energy-adjusted vitamin K2 and long-chain vitamin K2 intake with LVEF (P-interaction<0.01), but no significant associations were observed when stratified for presence of CVD (Additional file 5). None of the forms of vitamin K intake at baseline were associated with changes in LAVI during follow-up.
Sensitivity analyses
Excluding participants who developed CVD during follow-up (n=7) and adjusting for updated measurements of BMI, physical activity and smoking status at follow-up did not materially change our findings (Additional file 6). Adjusting for selection bias due to loss-to-follow-up using inverse probability weighting did not alter our findings as well (Additional file 6).
Discussion
This study showed that a higher vitamin K status at baseline was associated with decreased LVMI after 7.6 years of follow-up, only among women. Vitamin K status was not associated with other cardiac measures. Vitamin K intake was not associated with cardiac structure and function.
This study is the first prospective study investigating the association between vitamin K status and cardiac structure and function measures. Our results are in line with earlier cross-sectional studies showing that a low vitamin K status was associated with reduced LV systolic function [21] or a higher prevalence of LV diastolic dysfunction [23]. However, in our study, a higher vitamin K status was associated with LVMI only among women and not among men, but such effect modification by sex was not investigated in earlier studies. We didn’t observe any association between vitamin K status and LVEF or LAVI. Nevertheless, the studies that found an associations between vitamin K status and LV systolic or diastolic function were performed in populations with different features than those of the present study, the participants being affected by valvular diseases, HF or cardiomyopathy. Despite this association between vitamin K status and LVMI, we could not detect any significant associations between any of the forms of vitamin K intake and any of the cardiac structure and function measures. This is inconsistent with the study by Eshak et al. showing that a higher vitamin K intake was associated with a 37% reduced risk of HF mortality after 19 years of follow-up among Japanese women [20]. The inconsistent findings between both studies could be due to the relatively low sample size of our study combined with the relatively low validity of the FFQ to accurately assess vitamin K intake.
The underlying mechanism of vitamin K status and intake, cardiac structure and function and risk of HF may be explained by improved arterial stiffness with increased vitamin K intake and status. Animal experiments indeed showed that antagonism of vitamin K leads to vascular calcification, in particular of the medial layer of the arteries [36]. Medial calcification leads to vascular stiffness [37, 38], which in turn is consistently associated with LV diastolic dysfunction [39]. In fact, vascular stiffness may increase the systolic load on the ventricles and decrease aortic pressure during diastole, thereby increasing pulse pressure [40]. Increased pulse pressure increases myocardial oxygen demand during systole and is associated with LV hypertrophy. These changes can lead to impaired relaxation and eventually LV diastolic dysfunction and HFpEF [41]. Indeed, earlier studies have shown vitamin K status to be associated with increased arterial stiffness [22, 42, 43]. One possible explanation of why in our study vitamin K status affected LV structure only in women, is that women, especially after menopause, seem to be more prone to develop LV hypertrophy in response to pressure overload compared to men. Consequently, the effect of vitamin K status on arterial stiffness and cardiac overload might manifest itself only in women [32].
Strengths of this study include its prospective design and detailed phenotyping of the participants, allowing to adjust for multiple confounders. However, certain limitations need to be addressed. First, the high loss to follow-up rates in this study reduced our sample size and might have biased the prospective associations. Although we observed similar results in our analyses after inverse probability weighting, we cannot exclude some selection bias by the high loss of follow-up rates from baseline to the second cardiovascular assessment. Second, because our study population included only people of West-European origin, the generalizability of our findings is limited to studies performed in people of Western descent. Third, for the assessment of vitamin K intake we relied on self-reported data. Although the FFQ was validated for the assessment of vitamin K intake, the relative validity in particular for the assessment of vitamin K1 and short-chain vitamin K2 was low. In combination with the relatively small sample size, this may have yielded the study insufficiently sensitive to detect associations with vitamin K intake. Finally, the definition of vitamin K status was based on a single baseline measurement of dp-ucMGP, which may only reflect short-term vitamin K status. Therefore these associations should be interpreted with caution.
Conclusions
This study showed that a high vitamin K status is associated with decreased LVMI in women. Altogether these results further extend previous associations of vitamin K status with improved cardiac structure and function and a decreased risk of HF. An adequate vitamin K status, achieved via proper intake or possibly supplementation, might therefore be important to improve cardiac structure and function and prevent HF.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
09 December 2021
An amendment to this paper has been: One of the co-authors name should be tagged as Elisa (givenname) and Dal Canto (surname)
References
Schurgers LJ, Vermeer C. Determination of phylloquinone and menaquinones in food. Effect of food matrix on circulating vitamin K concentrations. Haemostasis. 2000;30(6):298–307.
Willems BA, Vermeer C, Reutelingsperger CP, Schurgers LJ. The realm of vitamin K dependent proteins: shifting from coagulation toward calcification. Mol Nutr Food Res. 2014;58(8):1620–35.
Luo G, Ducy P, McKee MD, Pinero GJ, Loyer E, Behringer RR, et al. Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature. 1997;386(6620):78–81.
Cancela ML, Laize V, Conceicao N, Kempf H, Murshed M. Keutel syndrome, a review of 50 years of literature. Front Cell Dev Biol. 2021;9:642136.
Cranenburg EC, Schurgers LJ, Vermeer C. Vitamin K: the coagulation vitamin that became omnipotent. Thromb Haemost. 2007;98(1):120–5.
Shea MK, O'Donnell CJ, Hoffmann U, Dallal GE, Dawson-Hughes B, Ordovas JM, et al. Vitamin K supplementation and progression of coronary artery calcium in older men and women. Am J Clin Nutr. 2009;89(6):1799–807.
Spronk HM, Soute BA, Schurgers LJ, Thijssen HH, De Mey JG, Vermeer C. Tissue-specific utilization of menaquinone-4 results in the prevention of arterial calcification in warfarin-treated rats. J Vasc Res. 2003;40(6):531–7.
Dalmeijer GW, van der Schouw YT, Magdeleyns E, Ahmed N, Vermeer C, Beulens JW. The effect of menaquinone-7 supplementation on circulating species of matrix Gla protein. Atherosclerosis. 2012;225(2):397–402.
Zwakenberg SR, de Jong PA, Bartstra JW, van Asperen R, Westerink J, de Valk H, et al. The effect of menaquinone-7 supplementation on vascular calcification in patients with diabetes: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2019;110(4):883–90.
Dalmeijer GW, van der Schouw YT, Magdeleyns EJ, Vermeer C, Elias SG, Velthuis BK, et al. Circulating species of matrix Gla protein and the risk of vascular calcification in healthy women. Int J Cardiol. 2013;168(6):e168–70.
Dalmeijer GW, van der Schouw YT, Magdeleyns EJ, Vermeer C, Verschuren WM, Boer JM, et al. Matrix Gla protein species and risk of cardiovascular events in type 2 diabetic patients. Diabetes Care. 2013;36(11):3766–71.
van den Heuvel EG, van Schoor NM, Lips P, Magdeleyns EJ, Deeg DJ, Vermeer C, et al. Circulating uncarboxylated matrix Gla protein, a marker of vitamin K status, as a risk factor of cardiovascular disease. Maturitas. 2014;77(2):137–41.
Dalmeijer GW, van der Schouw YT, Magdeleyns EJ, Vermeer C, Verschuren WM, Boer JM, et al. Circulating desphospho-uncarboxylated matrix gamma-carboxyglutamate protein and the risk of coronary heart disease and stroke. J Thromb Haemost. 2014;12(7):1028–34.
Liu YP, Gu YM, Thijs L, Knapen MH, Salvi E, Citterio L, et al. Inactive matrix Gla protein is causally related to adverse health outcomes: a Mendelian randomization study in a Flemish population. Hypertension. 2015;65(2):463–70.
Schurgers LJ, Aebert H, Vermeer C, Bultmann B, Janzen J. Oral anticoagulant treatment: friend or foe in cardiovascular disease? Blood. 2004;104(10):3231–2.
Schurgers LJ, Spronk HM. Differential cellular effects of old and new oral anticoagulants: consequences to the genesis and progression of atherosclerosis. Thromb Haemost. 2014;112(5):909–17.
Chen HG, Sheng LT, Zhang YB, Cao AL, Lai YW, Kunutsor SK, et al. Association of vitamin K with cardiovascular events and all-cause mortality: a systematic review and meta-analysis. Eur J Nutr. 2019;58(6):2191–205.
Ueland T, Dahl CP, Gullestad L, Aakhus S, Broch K, Skardal R, et al. Circulating levels of non-phosphorylated undercarboxylated matrix Gla protein are associated with disease severity in patients with chronic heart failure. Clin Sci (Lond). 2011;121(3):119–27.
Mayer O Jr, Seidlerova J, Vanek J, Karnosova P, Bruthans J, Filipovsky J, et al. The abnormal status of uncarboxylated matrix Gla protein species represents an additional mortality risk in heart failure patients with vascular disease. Int J Cardiol. 2016;203:916–22.
Eshak ES, Iso H, Yamagishi K, Cui R, Tamakoshi A. Dietary intakes of fat soluble vitamins as predictors of mortality from heart failure in a large prospective cohort study. Nutrition. 2018;47:50–5.
Ueland T, Gullestad L, Dahl CP, Aukrust P, Aakhus S, Solberg OG, et al. Undercarboxylated matrix Gla protein is associated with indices of heart failure and mortality in symptomatic aortic stenosis. J Intern Med. 2010;268(5):483–92.
Hashmath Z, Lee J, Gaddam S, Ansari B, Oldland G, Javaid K, et al. Vitamin K status, warfarin use, and arterial stiffness in heart failure. Hypertension. 2019;73(2):364–70.
Wei FF, Trenson S, Monney P, Yang WY, Pruijm M, Zhang ZY, et al. Epidemiological and histological findings implicate matrix Gla protein in diastolic left ventricular dysfunction. PLoS One. 2018;13(3):e0193967.
Rutters F, Nijpels G, Elders P, Stehouwer CDA, van der Heijden AA, Groeneveld L, et al. Cohort profile: the hoorn studies. Int J Epidemiol. 2018;47(2):396-j.
Ocke MC, Bueno-de-Mesquita HB, Goddijn HE, Jansen A, Pols MA, van Staveren WA, et al. The Dutch EPIC food frequency questionnaire. I. Description of the questionnaire, and relative validity and reproducibility for food groups. Int J Epidemiol. 1997;26(Suppl 1):S37–48.
Dutch Food Composition Table 2001. Den Haag.
Zwakenberg SR, Engelen AIP, Dalmeijer GW, Booth SL, Vermeer C, Drijvers J, et al. Reproducibility and relative validity of a food frequency questionnaire to estimate intake of dietary phylloquinone and menaquinones. Eur J Clin Nutr. 2017;71(12):1423–8.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233–70.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016;17(12):1321–60.
Wendel-Vos GC, Schuit AJ, Saris WH, Kromhout D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol. 2003;56(12):1163–9.
World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a WHO consultation. Geneva: Department of Noncommunicable Disease Surveillance; 1999.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Boomsma F, Deinum J, van den Meiracker AH. Relationship between natriuretic peptide concentrations in plasma and posture during blood sampling. Clin Chem. 2001;47(5):963–5.
Willett WC, Howe GR, Kushi LH. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. 1997;65(4 Suppl):1220S–8S discussion 9S-31S.
Greenland S. Tests for interaction in epidemiologic studies: a review and a study of power. Stat Med. 1983;2(2):243–51.
Kruger T, Oelenberg S, Kaesler N, Schurgers LJ, van de Sandt AM, Boor P, et al. Warfarin induces cardiovascular damage in mice. Arterioscler Thromb Vasc Biol. 2013;33(11):2618–24.
Mitchell GF. Arterial stiffness and wave reflection: biomarkers of cardiovascular risk. Artery Res. 2009;3(2):56–64.
O'Rourke MF. Arterial aging: pathophysiological principles. Vasc Med. 2007;12(4):329–41.
Chow B, Rabkin SW. The relationship between arterial stiffness and heart failure with preserved ejection fraction: a systemic meta-analysis. Heart Fail Rev. 2015;20(3):291–303.
Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107(22):2864–9.
O'Rourke MF. Diastolic heart failure, diastolic left ventricular dysfunction and exercise intolerance. J Am Coll Cardiol. 2001;38(3):803–5.
Pivin E, Ponte B, Pruijm M, Ackermann D, Guessous I, Ehret G, et al. Inactive matrix gla-protein is associated with arterial stiffness in an adult population-based study. Hypertension. 2015;66(1):85–92.
Fain ME, Kapuku GK, Paulson WD, Williams CF, Raed A, Dong Y, et al. Inactive matrix gla protein, arterial stiffness, and endothelial function in African American hemodialysis patients. Am J Hypertens. 2018;31(6):735–41.
Acknowledgements
The authors thank the other investigators, the staff, and the participants of the Hoorn Study participants for their valuable contributions
Funding
JWJ Beulens is supported by a ZonMw-VIDI grant (nr: 91718304) and AJ van Ballegooijen is supported by junior Kolff grant 16OKG02. No commercial funding was involved.
Author information
Authors and Affiliations
Contributions
Joline W.J. Beulens, Coen D.A. Stehouwer, Roger J.M.W. Rennenberg and Adriana Johanne van Ballegooijen contributed to the study conception and design; Joline W.J. Beulens, Coen D.A. Stehouwer and Adriana Johanne van Ballegooijen contributed to data collection, assembly, analysis and interpretation of the data; Joline W.J. Beulens, Elisa Dal Canto and Adriana Johanne van Ballegooijen contributed to the revising of the manuscript; Joline W.J. Beulens, Elisa Dal Canto, Coen D.A. Stehouwer, Roger J.M.W. Rennenberg, Petra Elders and Adriana Johanne van Ballegooijen contributed to the manuscript drafting and approval of the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided written informed consent and the local ethics committee of the VU University Medical Center approved the study.
Consent for publication
All participants provided informed consent for publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Flow chart of the Study Population selection.
Additional file 2.
Baseline characteristics of 427 participants stratified by quartiles of vitamin K intake.
Additional file 3.
Baseline characteristics of participants included and excluded for this study
Additional file 4.
Prospective non-linear association between intake of energy-adjusted vitamin K intake with LVEF in 427 participants.
Additional file 5.
Prospective association between vitamin K intake and left ventricular ejection fraction stratified by prior cardiovascular disease
Additional file 6.
Sensitivity analyses for the prospective association between vitamin K status and echocardiographic measurements
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Beulens, J.W.J., Dal Canto, E., Stehouwer, C.D.A. et al. High vitamin K status is prospectively associated with decreased left ventricular mass in women: the Hoorn Study. Nutr J 20, 85 (2021). https://doi.org/10.1186/s12937-021-00742-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-021-00742-0