
Abstract
Background
The main aim of this systematic review and meta-analysis was to identify peer-reviewed scholarly journal articles reporting the significance of physiotherapy interventions in managing TMJ ankylosis. In addition, this study aimed to critically appraise the existing evidence on the prevalence and clinical presentation, physiotherapy intervention approaches, efficacy of physiotherapy interventions, adverse effects, and safety of physiotherapy interventions in TMJ ankylosis management.
Methods
An all-inclusive literature search was conducted using the PubMed, Google Scholar, and Scopus electronic databases. The researchers screened the potential articles and assessed for eligibility based on the reported inclusion and exclusion criteria. The quality evaluation tool for observational cohort and cross-sectional studies developed by the National Institutes of Health (NIH) and the Cochrane Collaboration's Risk of Bias Tool were used to assess the quality of the included studies. Researchers also comprehensively analyzed the data, reported the results, and discussed them according to the predominant themes.
Results
The primary electronic database search yielded 409 articles, of which 25 were included in this review. A secondary search was conducted from citations of the included studies, yielding 74 articles, of which six were included in the study. A significantly higher prevalence of bony ankylosis than fibrous ankylosis, with an overall effect size of p < 0.00001. In addition, there were significantly more unilateral than bilateral presentations with an overall effect size of p < 0.00001. Moreover, there were 78 reported complications out of 245 subjects according to five included studies demonstrating a significant effect size with p = 0.001 following the treatment protocols.
Conclusion
This study highlighted the prevalence of bony ankylosis in temporomandibular joint ankylosis, emphasizing its impact on patients' well-being. On the other hand, the results show that physiotherapy is essential to optimize postoperative outcomes and minimize adverse events such as re-ankylosis. Practitioners and healthcare professionals must monitor postoperative recovery and ensure strict adherence to physiotherapy protocols for optimal outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Temporomandibular joint (TMJ) ankylosis is a complex and debilitating disorder characterized by the TMJ's abnormal fusion or limited range of motion [1]. This condition significantly affects essential mandibular functions [2]. The predominant etiology of this pathological amalgamation is commonly attributed to the formation of fibrous or osseous adhesions, which hinder the physiological functioning of the joint. TMJ Ankylosis has considerable implications for afflicted individuals, significantly affecting their oral health, dietary intake, and overall quality of life [3, 4].
The etiology of TMJ ankylosis is multifactorial, encompassing various variables such as trauma, infection, inflammation, and congenital anomalies [5]. Injuries, such as fractures affecting the mandible or temporal bone, can disrupt the complex joint structure and trigger a reparative mechanism that results in abnormal adhesions [6]. Infections, regardless of origin from trauma or secondary sources, can trigger inflammatory processes that lead to tissue damage and subsequent ankylosis [7, 8]. Although congenital anomalies are less common, they can heighten an individual's vulnerability to TMJ Ankylosis, presenting challenges in promptly identifying and treating this problem.
TMJ ankylosis clinically manifests as bony or fibrous ankylosis. Bony ankylosis occurs when bones in a joint fuse abnormally, forming osseous tissues and stiff links. Fibrous ankylosis is caused by abundant fibrous connective tissue that restricts joint mobility [6].
Diagnosing ankylosis involves evaluating the extent of adhesions, age at which the problem manifests, etiology, and duration of the ailment. Consequently, effective care of TMJ ankylosis necessitates a comprehensive approach encompassing surgical techniques, orthodontic modalities, and physiotherapeutic procedures [9].
Physiotherapy, a crucial component of this interdisciplinary approach, offers a variety of therapeutic interventions to improve jaw mobility, alleviate pain, and strengthen muscle strength [10, 11]. The interventions involve a variety of therapeutic exercises, manual techniques, and modalities such as heat, cold, or electrical stimulation [12, 13]. The primary goal of personalized physiotherapy interventions is to optimize oral function and alleviate the limitations associated with TMJ ankylosis, ultimately improving overall well-being [10].
There is a notable deficiency in our understanding of the efficacy of physiotherapy in managing TMJ ankylosis. Therefore, this study comprehensively analyzed the existing literature for evidence of the role of physiotherapy in the management of TMJ ankylosis. This research will provide insights into the prevalence and manifestations of TMJ ankylosis. Additionally, it seeks to investigate various physiotherapy intervention approaches, assess their efficacy, and evaluate the associated safety concerns and potential adverse consequences linked to these interventions.
The study's main aim is to emphasize the role of physiotherapy interventions by critically appraising the existing evidence on the prevalence and clinical presentation, physiotherapy intervention approaches, the efficacy of physiotherapy interventions, adverse effects, and safety of physiotherapy interventions in TMJ ankylosis management.
Materials and methods
The methods and results of this investigation are presented per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [14]. The protocol for this systematic review was registered at the International Platform of Registered Systematic Review and Meta-Analysis Protocols (INPLASY) (2023100029). The main research question was, "What is the efficacy of physiotherapy interventions in individuals with TMJ Ankylosis?".
Search strategy
A comprehensive electronic database search up to 8 October 2023 was conducted independently by two reviewers (SAM and AH) to identify peer-reviewed literature published in scholarly journals that reported on the role of physiotherapy interventions in managing TMJ ankylosis. Scopus, Google Scholar, and PubMed were searched using the following search terms: temporomandibular joint ankylosis, TMJ ankylosis, ankylosis of a TMJ, physiotherapy, physical therapy, rehabilitation, exercise therapy, manual therapy, therapeutic exercise, and orofacial exercises.
A secondary search was conducted from the reference lists of the included studies to identify potential articles that reported the significance of physiotherapy interventions in managing TMJ ankylosis.
Eligibility criteria
This study included current published research on the role of physiotherapy interventions in managing TMJ ankylosis adhering to the PICOS criteria [15]. The included studies reported the prevalence and clinical presentation, physiotherapy intervention approaches, efficacy of physiotherapy interventions, adverse effects, and safety of TMJ ankylosis management. Furthermore, the current investigation encompassed research involving human subjects, specifically those with at least eight participants. Moreover, the present study included reports with access to the full text and available in English. However, Reviews and meta-analyses, reports without methods and results, letters, and editorial notes were excluded from the study.
The PICOS criteria for eligible studies were defined as follows:
-
Population (P): Patients diagnosed with TMJ ankylosis.
-
Intervention (I): Physiotherapy interventions.
-
Comparison (C): No specific comparison is stated in the question.
-
Outcome (O): Efficacy in the management of TMJ ankylosis.
-
Study Design (S): This study considered Randomized Controlled Trials and other empirical research study designs.
Data selection and extraction
Article selection was conducted using a procedural screening process. Articles that did not meet the eligibility criteria were omitted from the study based on an assessment of their titles and abstracts. Two reviewers (MI and AK) examined the research titles and abstracts separately, followed by the full text of all papers that fulfilled the eligibility criteria. The reviewers' perspectives were thereafter discussed in order to reach a consensus. All discrepancies or concerns were addressed by engaging a third independent reviewer (MK) and resolved accordingly. Data from the included studies were systematically extracted and double-checked for consistency, as presented in Table 1, including the author, study design, sample size, mean age, study objectives, etiology, clinical presentation, physiotherapy techniques, and study findings.
Methodological quality assessment
The 17 prospective, retrospective, and observational studies included in this analysis were assessed using the quality evaluation tool for observational cohort and cross-sectional studies developed by the National Institutes of Health (NIH) [16]. On the other hand, 14 clinical and experimental studies were methodically evaluated using the Cochrane Collaboration's Risk of Bias Tool [34]. The quality assessment process for all selected articles was performed independently by two scorers (RS and AH).
Data analysis
Data from the included studies were systematically extracted and are presented in Table 1. The results were reported according to the prevalence, clinical presentation, physiotherapy intervention approaches, efficacy of physiotherapy interventions, adverse effects, and safety in TMJ ankylosis management. In addition, an intervention review approach was applied in analyzing quantitative data using Review Manager version 5.4.1. Moreover, proportion meta-analyses were conducted using the random effects analysis approach, the Mantel–Haenszel statistical method, and the odds ratio as the effect measure. A 95% confidence interval was applied in the analyses. The assessment of publication bias was conducted using Egger's test within the Review Manager 5 (RevMan 5) software (Version 5.4. Copenhagen: The Cochrane Collaboration, 2020).
Results
Study selection
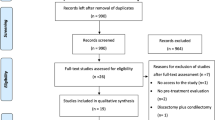
The literature search yielded 409 articles, of which 170 duplicates were removed. After title and abstract screening, 119 articles were excluded. The remaining 120 articles were retrieved, after which 25 studies that met the eligibility criteria were included. In addition, a secondary search of the reference lists yielded 74 articles, of which seven duplicate records were eliminated. Two articles could not be retrieved, and 67 were assessed for eligibility, after which six met the eligibility criteria and were included in the study. Figure 1 displays the obtained data.

PRISMA flow diagram showing the results of the study selection process
Methodological quality assessment
The results of the National Institutes of Health (NIH) quality assessment are presented in Table 2. In addition, Figs. 2 and 3 show the Cochrane Collaboration's Risk of Bias assessment results.

Summary plot showing the results of Cochrane Collaboration's Risk of Bias [34]

Traffic light plots showing the Cochrane Collaboration's Risk of Bias results [34]
Study characteristics
The results of the data analysis are thematically reported according to the predominant themes: prevalence and clinical presentation of TMJ ankylosis; physiotherapy interventions approach for TMJ ankylosis, the efficacy of physiotherapy interventions in TMJ ankylosis management, adverse effects and safety of physiotherapy interventions [49].
Prevalence and clinical presentation of TMJ ankylosis
These studies reported quantitative data comparing the clinical manifestations of TMJ ankylosis. Nevertheless, the findings of these two investigations were incorporated into the meta-analysis. A proportion meta-analysis showed a significantly higher prevalence of bony ankylosis than fibrous ankylosis with an overall effect size of p < 0.00001 (Fig. 4). The total events were 75 out of 80 subjects, as reported by two of the included studies.

In contrast, Bayat et al. [18] reported that all participants had bony ankylosis. Bony ankylosis was found in 77 (71%), fibrous ankylosis in 6 (6%), and fibro-osseous ankylosis in 26 (24%) patients by Elgazzar et al. [35]. On the other hand, a study by Dowgierd et al. [20] reported that 82% of the joints under study had bony-type ankylosis. The study by Jain et al. [21] had nine out of 18 joints manifesting fibro-osseous ankylosis. Computed tomography scans revealed fibro-osseous in 9 joints, fibrous in 5, and bony ankylosis in 4 [22]. Khalifa [41] investigated bony ankylosis and reported type II manifestation in three patients (11.54), type III in 22 patients (84.61), and type IV in one patient (3.85).
There were 189 bilateral events and 558 events out of 747 subjects, as reported by 21 of the included studies, demonstrating significantly more unilateral than bilateral presentations with an overall effect size of p < 0.00001, as shown in Fig. 5. Figure 6 shows the publication bias of the clinical manifestation of the temporomandibular joint ankylosis analysis.


Physiotherapy interventions approaches for TMJ ankylosis
The studies that were included reported active physiotherapy as part of the treatment protocol. Various devices have been used, including wooden spoons [17]. The participants were instructed to utilize wooden spoons positioned between their incisors, gradually increasing the quantity of spoons at predefined intervals. According to Bayat et al. [18], patients used Therabite devices for continuous passive exercise. Elgazzar et al. [35] reported mouth opening and jaw exercises, massage, and deep heat therapy.
Customized mouth gags were used by patients, including inter-incisal acrylic gags with a jack screw, according to Güven et al. [38]. The study participants used wooden tongue blades, increasing the numbers gradually depending on the subjects' tolerance in the study by Hegab [39]. Similarly, a study [21] reported patients using Ferguson's mouth gag and wooden tongue blades for active jaw physiotherapy. According to Kaban et al. [22], physiotherapy was performed using heat, massage, ultrasonography, gum chewing, manual stretching exercises, and a bell dynamic jaw exerciser.
In addition, mouth gags, props, and chewing gum have been used for aggressive physiotherapy [41].
Efficacy of physiotherapy interventions in TMJ ankylosis management
Ahmad et al. [17] reported the simplicity and ease of measuring mouth opening using wooden spoons, demonstrating physiotherapy's effectiveness in managing TMJ ankylosis. The number of spoons accommodated was used to measure the extent of the mouth opening.
On the other hand, physiotherapy is essential in preventing re-ankylosis [18,19,20,21]. Studies by Elgazzar et al. [35] and Lin et al. [32] have reported non-compliance with physiotherapy protocols as a significant cause of postoperative complications. According to Singh et al. [30], physiotherapy is essential for preserving the postoperative outcomes of surgical intervention.
Adverse effects and safety of physiotherapy interventions
There were 78 reported complications out of 245 subjects according to five included studies demonstrating a significant effect size with p = 0.001 following the treatment protocols, as shown in Fig. 7. Figure 8 shows the risk of bias assessment of the safety profile analysis.


Ahmad et al. [17] reported that complication rates were significantly low in modified T-plate interposition arthroplasty, reporting three patients with complications, including hematoma, infection, and re-ankylosis. In contrast, Bayat et al. [18] reported complications, including re-ankylosis, postoperative infection, and temporary facial palsy. Some patients had a severe hemorrhage, facial nerve palsy, and re-ankylosis [19].
According to Dowgierd et al. [20], six patients reported complications, including ectopic bone formation on the TMJ in one patient, relapse in three patients, and infection in two patients. In addition, Elgazzar et al. [35] reported persistent pain, limited mouth opening, facial weakness, partial graft resorption, intraoperative bleeding, slight condylar overgrowth, transient facial nerve weakness, loose hardware, infection, and re-ankylosis. Patients reported temporary paresis of the facial nerve, open bite, re-ankylosis, and Frey's syndrome [36].
Patients reported pain during physiotherapy in the early postoperative days [26, 39, 45, 47]. Excessive bleeding, wound hematoma, re-ankylosis, facial nerve injury, and wound infections have been reported by patients [21]. Conversely, no complications have been observed [26, 28, 39, 42]. According to Park et al. [44], one patient reported an anterior open bite.
Discussion
TMJ ankylosis manifests clinically in various ways. The study results showed that bony ankylosis is more common than fibrous ankylosis. Bony ankylosis is characterized by stiffness, limiting joint movements, and significantly affecting the patient's general health [50]. In addition, most patients reported unilateral manifestations rather than bilateral cases. Understanding the clinical manifestations is critical for developing effective treatment protocols for managing TMJ ankylosis while minimizing recurrence and adverse effects.
Higher bony ankylosis prevalence compared to fibrous may be associated with various factors. Bony-type ankylosis may result from more severe inflammatory processes or trauma, leading to increased clinical manifestations and patient reporting. In addition, bony ankylosis is more visible diagnostically, manifesting in the form of joint stiffness, thus easily identifiable, contributing to its higher reported prevalence in the included studies. Moreover, the adverse effect of bony ankylosis on the patient's quality of life prompts diagnosis and intervention, which are more prevalent in clinical studies.
In addition, the results show various treatment protocols incorporating different physiotherapy techniques to optimize the postoperative results of TMJ ankylosis. Physiotherapy techniques use multiple tools, including wooden spoons, Therabite devices, personalized mouth gags, and various exercises [17, 18]. Physiotherapy techniques optimize mouth opening and accelerate healing after surgery. The included studies emphasized the significance of physiotherapy in minimizing re-ankylosis and other postoperative complications.
On the other hand, most physiotherapy techniques were considered safe and effective in minimizing adverse events [18,19,20,21, 27]. There were considerably fewer postoperative adverse events, as shown in Fig. 6. However, pain during physiotherapy has been reported. Nevertheless, the pain reduced over time, gradually making it easy to continue physiotherapy. In addition, evidence shows that physiotherapy therapies are essential for optimizing postoperative outcomes and preventing re-ankylosis. The devices employed, such as wooden spoons in the treatment protocols, are simple to use and can be used to measure mouth opening and keep track of progress. These studies emphasize compliance with physiotherapy protocols for optimal results.
The incidence of postoperative complications was significantly lower. Nevertheless, understanding the possible adverse events of physiotherapy treatments is vital for providing complete patient care. Therefore, it is essential to carefully monitor patients after surgery and emphasize compliance with predefined protocols to minimize hematomas, infections, facial nerve palsy, and re-ankylosis.
The physiotherapy protocols have a relatively good reported safety and compliance due to the customized and gradual nature of specific individual needs. Appropriate protocols emphasize patient comfort, enhancing compliance while minimizing adverse effects and postoperative complications. In addition, simple tools used and regular monitoring strengthen the safety of the treatment protocols.
This comprehensive analysis of the clinical manifestations and treatment protocols for TMJ ankylosis highlights the importance of understanding the various aspects of this condition. Bony ankylosis, more prevalent than fibrous ankylosis, can significantly impact the patient's quality of life. Incorporating physiotherapy techniques into the treatment plans is crucial for optimizing postoperative outcomes, minimizing re-ankylosis, and reducing complications.
While physiotherapy techniques have proven safe and effective, healthcare professionals should remain vigilant in monitoring patients after surgery and ensuring compliance with predefined protocols. This proactive approach can help minimize adverse events and provide complete patient care. By continuing to advance our knowledge of the clinical manifestations and treatment options for TMJ ankylosis, we can improve patient outcomes and enhance the overall management of this condition.
Limitations of the evidence included in the review
While the evidence presented in the previous discussion provides valuable insights into the clinical manifestations and treatment protocols for TMJ (TMJ) ankylosis, it is essential to acknowledge the limitations of the reviewed studies. These limitations may affect the generalizability and reliability of the findings.
-
1.
Small Sample Size: Some of the included studies in the analysis had a small sample size, which could impact the statistical power and generalizability of the results.
-
2.
Heterogeneity of Study Designs: The studies encompassed a range of designs, leading to heterogeneity in methodology and outcome measurements. This variance in study designs may make it challenging to draw definitive conclusions or establish standardized treatment protocols for TMJ ankylosis.
-
3.
Lack of Randomization and Blinding: Several studies did not employ randomization or blinding techniques, which raises the potential for bias in the results. Without randomization, there is an increased risk of selection bias, as participants may not be representative of the overall population or the specific subgroups being studied.
-
4.
Lack of Long-term Follow-up: Many of the included studies had a relatively short follow-up period, which limits the ability to assess the long-term effectiveness and potential complications associated with the treatment protocols.
It is crucial to consider these limitations when interpreting the evidence presented. Further research with larger sample sizes, standardized study designs, randomized controlled trials, and long-term follow-up periods is needed to address these limitations and provide more robust evidence on the clinical manifestations and treatment protocols for TMJ ankylosis.
Implications for clinical practice
The findings presented in the above article have several implications for clinical practice in the management of TMJ (TMJ) ankylosis:
-
1. Treatment Protocol Optimization: Clinicians should consider incorporating physiotherapy techniques, such as wooden spoons, Therabite devices, personalized mouth gags, and specific exercises, to improve postoperative outcomes and minimize the chances of re-ankylosis.
-
2. Patient Compliance and Education: Healthcare professionals should educate patients about the benefits of physiotherapy and the potential consequences of non-compliance, including re-ankylosis and other postoperative complications.
-
3. Risk and Complication Management: Healthcare practitioners should be vigilant in monitoring patients after surgery, mainly to prevent complications such as hematomas, infections, facial nerve palsy, and re-ankylosis. Adherence to predefined protocols for postoperative care is crucial in minimizing the incidence of adverse events. Regular follow-up appointments are essential to evaluate the long-term outcomes and address emerging complications.
Implications for policy
The research findings have several implications for healthcare policies related to TMJ ankylosis:
-
1. Standardized Treatment Guidelines: Policymakers should consider developing standardized treatment guidelines for TMJ ankylosis. These guidelines should include recommendations for incorporating physiotherapy techniques as an integral part of the treatment process.
-
2. Access to Physiotherapy Services: Policymakers should evaluate the availability and accessibility of physiotherapy services for patients with TMJ ankylosis. Ensuring that these services are readily available to patients, regardless of geographical location or financial barriers, would support optimal postoperative outcomes and reduce the likelihood of complications or re-ankylosis.
Implications for future research
While the discussed study contributes to the understanding of TMJ ankylosis, there are opportunities for further research:
-
1. Randomized Controlled Trials: Future research should focus on conducting well-designed randomized controlled trials with larger sample sizes. These trials would provide a higher level of evidence on the effectiveness and safety of physiotherapy techniques for TMJ ankylosis.
-
2. Long-term Follow-up Studies: Longitudinal studies with extended follow-up periods are needed to evaluate the sustained outcomes of various treatment protocols for TMJ ankylosis. These studies would provide insights into the long-term functional improvements, rates of recurrence, and potential complications associated with different treatment approaches.
-
3. Comparative Effectiveness Research: Comparative effectiveness research comparing various physiotherapy techniques and treatment approaches would help determine the most effective interventions for TMJ ankylosis. This research would assist clinicians in making informed decisions regarding selecting treatment protocols for individual patients.
Conclusion
The present study evaluated the prevalence and clinical presentation of physiotherapy intervention approaches, efficacy of physiotherapy interventions, adverse effects, and safety of physiotherapy interventions in TMJ ankylosis management. This study highlighted the prevalence of bony ankylosis in temporomandibular joint ankylosis, emphasizing its impact on patients' well-being. On the other hand, the results show that physiotherapy is essential to optimize postoperative outcomes and minimize adverse events such as re-ankylosis. Practitioners and healthcare professionals need to monitor postoperative recovery and ensure strict adherence to physiotherapy protocols for optimal outcomes. However, there is limited empirical research directly investigating the role of physiotherapy interventions in managing TMJ ankylosis. Therefore, further studies should be carried out to verify the results of this study.
Availability of data and materials
No datasets were generated or analysed during the current study.
References
Movahed R, Mercuri LG. Management of temporomandibular joint ankylosis. Oral Maxillofac Surg Clin North Am. 2015;27(1):27–35.
Goswami D, Singh S, Bhutia O, Baidya D, Sawhney C. Management of young patients with temporomandibular joint ankylosis-a surgical and anesthetic challenge. Indian J Surg. 2016;78(6):482–9.
Jafarian M, Dehghani N. Simultaneous chin onlay bone graft using elongated coronoid in the treatment of temporomandibular joint ankylosis. J Craniofac Surg. 2014;25(1):e38-44.
Minervini G, Franco R, Marrapodi MM, Ronsivalle V, Shapira I, Cicciù M. Prevalence of temporomandibular disorders in subjects affected by Parkinson disease: A systematic review and metanalysis. J Oral Rehabil. 2023;50(9):877–85. https://doi.org/10.1111/joor.13496. Epub 2023 May 24.
Mokhtar EA, Fatima Q, Akbar S, Equbal S, Salahudeen A. Rhino-orbital cerebral mucormycosis causing temporomandibular joint ankylosis: a case series of two patients. Cureus. 2023;15(2):e35194.
Yan YB, Liang SX, Shen J, Zhang JC, Zhang Y. Current concepts in the pathogenesis of traumatic temporomandibular joint ankylosis. Head Face Med. 2014;10:35.
Parrino D, Val M, Lovato A, de Filippis C, Nardini LG. Pediatric temporomandibular joint ankylosis and arthritis: forgotten complications of acute otitis media. Am J Otolaryngol. 2022;43(5):103599.
Minervini G, D’Amico C, Cicciù M, Fiorillo L. Temporomandibular joint disk displacement: etiology, diagnosis, imaging, and therapeutic approaches. J Craniofac Surg. 2023;34(3):1115–21.
Amarista FJ, Perez DE. Concomitant Temporomandibular Joint Replacement and Orthognathic Surgery. Diagnostics (Basel). 2023;13(15):2486. https://doi.org/10.3390/diagnostics13152486.
McNeely ML, Armijo Olivo S, Magee DJ. A systematic review of the effectiveness of physical therapy interventions for temporomandibular disorders. Phys Ther. 2006;86(5):710–25.
Minervini G, Lucchese A, Perillo L, Serpico R, Minervini G. Unilateral superior condylar neck fracture with dislocation in a child treated with an acrylic splint in the upper arch for functional repositioning of the mandible. Cranio. 2017;35(5):337–41.
Kumar SP, Jim A. Physical therapy in palliative care: from symptom control to quality of life: a critical review. Indian J Palliat Care. 2010;16(3):138–46.
Minervini G, Franco R, Marrapodi MM, Di Blasio M, Isola G, Cicciù M. Conservative treatment of temporomandibular joint condylar fractures: a systematic review conducted according to PRISMA guidelines and the Cochrane handbook for systematic reviews of interventions. J Oral Rehabil. 2023;50(9):886–93.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89.
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. 2014;14(1):579.
Ma L-L, Wang Y-Y, Yang Z-H, Huang D, Weng H, Zeng X-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. 2020;7(1):7.
Ahmad I, Mir MA, Bariar LM. Modified T-plate interpositional arthroplasty for temporomandibular joint ankylosis: a new and versatile option. Arch Plast Surg. 2015;42(6):716–20.
Bayat M, Badri A, Moharamnejad N. Treatment of temporomandibular joint ankylosis: gap and interpositional arthroplasty with temporalis muscle flap. Oral Maxillofac Surg. 2009;13(4):207–12.
Braimah R, Taiwo A, Ibikunle A, Oladejo T, Adeyemi M, Adejobi F, Abubakar S. Clinical experience in managing temporomandibular joint ankylosis: five-year appraisal in a Nigerian subpopulation. J Korean Assoc Oral Maxillofac Surg. 2018;44(3):112–9.
Dowgierd K, Pokrowiecki R, Kulesa Mrowiecka M, Dowgierd M, Woś J, Szymor P, Kozakiewicz M, Lipowicz A, Roman M, Myśliwiec A. Protocol for Multi-Stage Treatment of Temporomandibular Joint Ankylosis in Children and Adolescents. J Clin Med. 2022;11(2):428. https://doi.org/10.3390/jcm11020428.
Jain G, Kumar S, Rana AS, Bansal V, Sharma P, Vikram A. Temporomandibular joint ankylosis: a review of 44 cases. Oral Maxillofac Surg. 2008;12(2):61–6.
Kaban LB, Perrott DH, Fisher K. A protocol for management of temporomandibular joint ankylosis. J Oral Maxillofacial Surg. 1990;48(11):1145–51 discussion 1152.
Kohli S, Mohanty S, Singh S, Sandeep, Dabas J, Patel R. The autogenous graft versus transport distraction osteogenesis for reconstruction of the ramus-condyle unit: a prospective comparative study. Int J Oral Maxillofacial Surg. 2017;46(9):1106–17.
Longobardi G, Boniello R, Gasparini G, Pelo S. A new 3-phase therapy protocol in temporomandibular joint ankylosis: our experience. J Craniofac Surg. 2009;20(2):483–7.
Nitzan DW, Abu Tair J, Lehman H. Is entire removal of a post-traumatic temporomandibular joint ankylotic site necessary for an optimal outcome? J Oral Maxillofacial Surg. 2012;70(12):e683-699.
Sami A, Hashmi GS, Rahman SA, Rahman T, Ansari MK. Comparative evaluation of temporal fascia and dermal fat graft in the management of temporomandibular joint ankylosis. Natl J Maxillofac Surg. 2023;14(2):277–81.
Shetty V, Nanda Kishore P, Khanum A, Yadav A, Sailer HF. Retrospective analysis of a TMJ ankylosis protocol with a 9 year follow up. J Craniomaxillofac Surg. 2019;47(12):1903–12.
Shivakotee S, Menon CS, Sham ME, Kumar V, Archana S. TMJ ankylosis management: our experience. J Maxillofac Oral Surg. 2020;19(4):579–84.
Singh V, Bhagol A, Dhingra R, Kumar P, Sharma N, Singhal R. Management of temporomandibular joint ankylosis type III: lateral arthroplasty as a treatment of choice. Int J Oral Maxillofac Surg. 2014;43(4):460–4.
Singh V, Dhingra R, Bhagol A. Prospective analysis of temporomandibular joint reconstruction in ankylosis with sternoclavicular graft and buccal fat pad lining. J Oral Maxillofacial Surg. 2012;70(4):997–1006.
Tauro DP, Manay RS. The nuances of temporomandibular joint ankylosis surgery: tips and tricks. J Maxillofac Oral Surg. 2020;19(2):178–83.
Lin X, Li HY, Xie QT, Zhang T, Huang XP, Zhou N. Surgical treatment of type III temporomandibular joint ankylosis with a lateral arthroplasty while retaining the medially displaced condyle. Ann R Coll Surg Engl. 2019;101(6):415–21.
Yadav P, Roychoudhury A, Bhutia O. Strategies to reduce re-ankylosis in temporomandibular joint ankylosis patients. Br J Oral Maxillofac Surg. 2021;59(7):820–5.
Corbett MS, Higgins JP, Woolacott NF. Assessing baseline imbalance in randomised trials: implications for the Cochrane risk of bias tool. Res Synth Methods. 2014;5(1):79–85.
Elgazzar RF, Abdelhady AI, Saad KA, Elshaal MA, Hussain MM, Abdelal SE, Sadakah AA. Treatment modalities of TMJ ankylosis: experience in Delta Nile, Egypt. Int J Oral Maxillofacial Surg. 2010;39(4):333–42.
Erol B, Tanrikulu R, Görgün B. A clinical study on ankylosis of the temporomandibular joint. J Craniomaxillofac Surg. 2006;34(2):100–6.
Fariña R, Canto L, Gunckel R, Alister JP, Uribe F. Temporomandibular joint ankylosis: algorithm of treatment. J Craniofac Surg. 2018;29(2):427–31.
Güven O. A clinical study on temporomandibular joint ankylosis. Auris Nasus Larynx. 2000;27(1):27–33.
Hegab AF. Outcome of surgical protocol for treatment of temporomandibular joint ankylosis based on the pathogenesis of ankylosis and re-ankylosis. A prospective clinical study of 14 patients. J Oral Maxillofacial Surg. 2015;73(12):2300–11.
Jakhar SK, Agarwal M, Gupta DK, Tiwari AD. Preservation of condyle and disc in the surgical treatment of type III temporomandibular joint ankylosis: a long-term follow-up clinical study of 111 joints. Int J Oral Maxillofac Surg. 2013;42(6):746–51.
Khalifa GA. Monitoring of incremental changes in maximum interincisal opening after gap arthroplasty omits the risk of re-ankylosis. J Craniomaxillofac Surg. 2018;46(1):75–81.
Lo LJ, Lin CL, Chen YR. A device for temporomandibular joint exercise and trismus correction: design and clinical application. J Plast Reconstr Aesthet Surg. 2008;61(3):297–301.
Nouman D, Hassan K. Post operative physiotherapy management of temporomandibular joint ankylosis. Int J Physiother Res. 2017;5(5):2320–4.
Park MW, Eo MY, Seo BY, Nguyen TTH, Kim SM. Gap arthroplasty with active mouth opening exercises using an interocclusal splint in temporomandibular joint ankylosis patients. Maxillofac Plast Reconstr Surg. 2019;41(1):18.
Rahman SA, Rahman T, Hashmi GS, Ahmed SS, Ansari MK, Sami A. A clinical and radiological investigation of the use of dermal fat graft as an interpositional material in temporomandibular joint ankylosis surgery. Craniomaxillofac Trauma Reconstr. 2020;13(1):53–8.
Sahoo NK, Tomar K, Kumar A, Roy ID. Selecting reconstruction option for TMJ ankylosis: a surgeon’s dilemma. J Craniofac Surg. 2012;23(6):1796–801.
Younis M, Shah AA, Hassan S, Kapoor M, Rashid A. Abdominal dermis-fat graft versus conventional temporalis myofascial flap interposition in temporomandibular joint ankylosis: a prospective clinical comparative study. J Maxillofac Oral Surg. 2021;20(1):54–62.
Zhang Y, He DM. Clinical investigation of early post-traumatic temporomandibular joint ankylosis and the role of repositioning discs in treatment. Int J Oral Maxillofac Surg. 2006;35(12):1096–101.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Hagen KB, Dagfinrud H, Moe RH, Østerås N, Kjeken I, Grotle M, Smedslund G. Exercise therapy for bone and muscle health: an overview of systematic reviews. BMC Med. 2012;10:167.
Acknowledgements
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through a Small Group Research Project under grant number RGP1/331/44.
Funding
All authors thank King Khalid University, Saudi Arabia, for the financial Support.
Author information
Authors and Affiliations
Contributions
Conceptualization and Methodology: Saeed Hassan, Ravinder Saini; Data Curation and Formal Analysis: Saeed Hassan, Mohammed Ibrahim, Mohasin Khader; Investigation and Resources: Masroor Kanji, Abdulhamid Ghwainem; Original draft preparation: Ravinder S Saini, Artak Heboyan, Seyed Ali Mosaddad; Writing, Reviewing, and Editing: Masroor Kanji, Mohammed Ibrahim, Mohasin Khader, Seyed Ali Mosaddad; Supervision and Project Administration: Ravinder Saini, Artak Heboyan; Funding Acquisition: Saeed Hassan.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable due to the design of the study as a systematic review.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Saini, R.S., Ibrahim, M., Khader, M.A. et al. The role of physiotherapy interventions in the management of temporomandibular joint ankylosis: a systematic review and meta-analysis. Head Face Med 20, 15 (2024). https://doi.org/10.1186/s13005-024-00416-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13005-024-00416-2